Normal Postoperative Computed Tomography Findings after a Variety of Pancreatic Surgeries
- Affiliations
-
- 1Department of Radiology, Severance Hospital, Research Institute of Radiological Science, Yonsei University College of Medicine, Seoul 03722, Korea. yelv@yuhs.ac
- 2Department of Surgery, Yonsei University College of Medicine, Seoul 03722, Korea.
- KMID: 2427942
- DOI: http://doi.org/10.3348/kjr.2017.18.2.299
Abstract
- Pancreatic surgery remains the only curative treatment for pancreatic neoplasms, and plays an important role in the management of medically intractable diseases. Since the original Whipple operation in the 20th century, surgical techniques have advanced, resulting in decreased postoperative complications and better clinical outcomes. Normal postoperative imaging findings vary greatly depending on the surgical technique used. Radiologists are required to be familiar with the normal postoperative imaging findings, in order to distinguish from postoperative complications or tumor recurrence. In this study, we briefly review a variety of surgical techniques for the pancreas, and present the normal postoperative computed tomography findings.
MeSH Terms
Figure
-

Fig. 1 Schema (lower left corner in A) and postoperative computed tomography coronal (A and B) and axial (C) images of Whipple operation. Distal stomach is resected together with duodenum, distal common bile duct, and pancreas head. Choledochojejunostomy (arrow in A), gastrojejunostomy (arrow in B), and pancreaticojejunostomy (arrow in C) are made.

Fig. 2 Schema of pancreaticoduodenectomy (lower left corner in A) and postoperative coronal (A) and axial (B) computed tomography images. Stomach and proximal portion of duodenum are preserved, and choledochojejunostomy, duodenojejunostomy (arrow in A), and pancreaticojejunostomy (black arrow in B) are made.

Fig. 3 Invagination pancreaticojejunostomy (dunking method) (schema: lower left corner in A). Entire pancreatic remnant is dunked into jejunal lumen (arrow in A). Pancreaticojejunal anastomosis is anterior to superior mesenteric artery and splenic vein. Remnant pancreas can protrude into jejunal lumen, which can mimic tumor recurrence (arrow in B).

Fig. 4 (A-C) Postoperative computed tomography image (schema: lower left corner in A) and intraoperative images of duct-to-mucosa pancreaticojejunostomy (B, C). Main pancreatic duct of remnant pancreas is sutured to jejunal mucosa (B). Reinforcement sutures are done between remnant pancreas and jejunal serosa (C). At pancreaticojejunostomy site (arrow in A), pancreatic parenchyma is not protruding into jejunal lumen.

Fig. 5 Postoperative computed tomography image and schema of pancreaticogastrostomy (lower left corner). Remnant pancreas is attached to posterior wall of proximal stomach (arrow) usually with duct-to-mucosa method.

Fig. 6 Schema and postoperative computed tomography image of distal pancreatectomy. A. Schema of standard retrograde distal pancreatosplenectomy (dashed arrow) and radical antegrade modular pancreatosplenectomy (RAMPS) (arrow). Standard retrograde distal pancreatosplenectomy starts from spleen and proceeds to pancreas neck. In contrast, RAMPS begins from neck of pancreas and dissection is continued in opposite direction. B. Surgical planes on computed tomography (CT) image of anterior and posterior RAMPS. In anterior RAMPS, dissection is done along Gerota fascia and anterior to adrenal gland (arrow). In posterior RAMPS, dissection is done posterior to adrenal gland (dashed arrow). C. Postoperative CT images of anterior RAMPS. Note that left adrenal gland is preserved (arrow). D. Postoperative CT image of posterior RAMPS. Note that left adrenal gland is not seen.

Fig. 7 Schema of spleen-preserving distal pancreatectomy (Warshaw procedure) (lower left corner). Note that spleen is preserved. Dilated collateral vessels are seen (arrow).
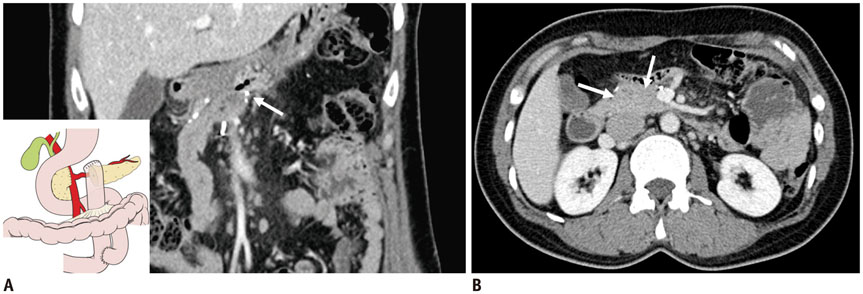
Fig. 8 Schema (lower left corner of A) and postoperative coronal (A) and axial (B) computed tomography images after central pancreatectomy. A. Distal part of remnant pancreas is anastomosed to jejunum (arrow). B. Pancreas head (arrows) is preserved while maintaining physiologic biliary drainage route.

Fig. 9 Postoperative axial (A) and coronal (B) computed tomography image of total pancreatectomy. Entire parenchyma of pancreas was removed and 2 anastomoses, choledochojejunostomy for biliary drainage (arrows in A, B) and gastrojejunostomy for food passage (arrowhead in A), were reconstructed.

Fig. 10 Schema (lower left corner) and postoperative computed tomography (CT) image of side-to-side pancreaticojejunostomy (Partington and Rochelle procedure). Main pancreatic duct is opened from neck to tail of pancreas. Pancreaticojejunostomy is then performed in side-to-side manner. Note that pancreatic duct at body portion (arrows) is anastomosed with jejunal lumen (arrowheads) on postoperative CT image.

Fig. 11 Schema (upper right corner), intraoperative image (lower left corner), and postoperative computed tomography (CT) image of Frey operation. Because anterior shell of pancreas head is removed (thick arrow), cavitary lesion with air bubble and fluid collection can be seen at pancreas head on CT (thin arrow). Pancreatic duct is incised from head to tail, followed by anastomosis to jejunal Y-rim (arrowheads) in side-to-side manner.
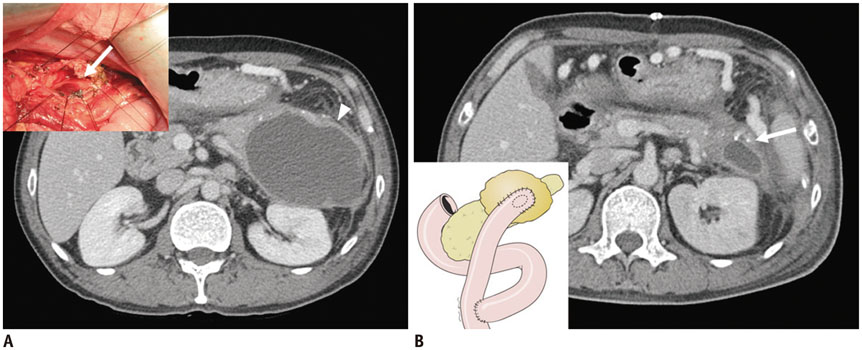
Fig. 12 Computed tomography (CT) and schema of cystojejunostomy. A. Intraoperative image (upper left corner) and preoperative CT image of cystojejunostomy. Pseudocyst is opened (arrow) and anastomosed to jejunal Y-rim. Note that pancreatic pseudocyst is seen in pancreas tail on preoperative CT image (arrowhead). B. Schema of cystojejunostomy (lower left corner). Postoperative CT image shows that pancreatic pseudocyst is anastomosed to jejunal Y-rim (arrow).

Fig. 13 Preoperative (A) and postoperative (B) computed tomography image of cystogastrostomy. Pseudocyst is seen posterior to stomach (arrow in A). After cystogastromy, pseudocyst is decreased in size. Note anastomosis site between pseudocyst and posterior wall of stomach (arrow in B).

Fig. 14 Computed tomography (CT) and schema of transduodenal ampullectomy. A. Schema of transduodenal ampullectomy. Different resection margins between ampullectomy and papillectomy are shown. Red line shows resection margin of ampullectomy, cutting pancreatic duct and common bile duct (CBD). In contrast, resection margin of papillectomy does not include pancreatic duct and CBD (blue line). B, C. Intraoperative image (upper right corner) showing ampulla removed through transduodenal approach. Postoperative CT image shows irregular wall of duodenum and adjacent fluid collection and fat infiltration. Postoperative coronal (B) and axial (C) CT images show irregular thickening of duodenal wall with adjacent fluid collection and fat infiltration. Inserted t-tube within duct is noted in coronal CT image and intraoperative photography just before repositioning between duodenal mucosa and bile duct and pancreatic duct. Internal short stents are inserted to bile duct and pancreatic duct (arrow in B).
Cited by 1 articles
-
Measurement of Pancreatic Fat Fraction by CT Histogram Analysis to Predict Pancreatic Fistula after Pancreaticoduodenectomy
Wonju Hong, Hong Il Ha, Jung Woo Lee, Sang Min Lee, Min-Jeong Kim
Korean J Radiol. 2019;20(4):599-608. doi: 10.3348/kjr.2018.0557.
Reference
-
1. Ozawa F, Friess H, Künzli B, Shrikhande SV, Otani T, Makuuchi M, et al. Treatment of pancreatic cancer: the role of surgery. Dig Dis. 2001; 19:47–56.2. Strasberg SM, Drebin JA, Linehan D. Radical antegrade modular pancreatosplenectomy. Surgery. 2003; 133:521–527.3. Roggin KK, Rudloff U, Blumgart LH, Brennan MF. Central pancreatectomy revisited. J Gastrointest Surg. 2006; 10:804–812.4. Ho CK, Kleeff J, Friess H, Büchler MW. Complications of pancreatic surgery. HPB (Oxford). 2005; 7:99–108.5. Casadei R, Ricci C, Antonacci N, Minni F. Indications and technique of central pancreatectomy. In : Siquini W, editor. Surgical treatment of pancreatic disease. Milan: Springer Milan;2009. p. 329–336.6. Kim MJ, Choi JY, Chung YE. Evaluation of biliary malignancies using multidetector-row computed tomography. J Comput Assist Tomogr. 2010; 34:496–505.7. Bhosale P, Fleming J, Balachandran A, Charnsangavej C, Tamm EP. Complications of Whipple surgery: imaging analysis. Abdom Imaging. 2013; 38:273–284.8. Diener MK, Fitzmaurice C, Schwarzer G, Seiler CM, Hüttner FJ, Antes G, et al. Pylorus-preserving pancreaticoduodenectomy (pp Whipple) versus pancreaticoduodenectomy (classic Whipple) for surgical treatment of periampullary and pancreatic carcinoma. Cochrane Database Syst Rev. 2014; (11):CD006053.9. Yamauchi FI, Ortega CD, Blasbalg R, Rocha MS, Jukemura J, Cerri GG. Multidetector CT evaluation of the postoperative pancreas. Radiographics. 2012; 32:743–764.10. Poon RT, Lo SH, Fong D, Fan ST, Wong J. Prevention of pancreatic anastomotic leakage after pancreaticoduodenectomy. Am J Surg. 2002; 183:42–52.11. Kennedy EP, Yeo CJ. Dunking pancreaticojejunostomy versus duct-to-mucosa anastomosis. J Hepatobiliary Pancreat Sci. 2011; 18:769–774.12. Bassi C, Dervenis C, Butturini G, Fingerhut A, Yeo C, Izbicki J, et al. Postoperative pancreatic fistula: an international study group (ISGPF) definition. Surgery. 2005; 138:8–13.13. El Nakeeb A, El Hemaly M, Askr W, Abd Ellatif M, Hamed H, Elghawalby A, et al. Comparative study between duct to mucosa and invagination pancreaticojejunostomy after pancreaticoduodenectomy: a prospective randomized study. Int J Surg. 2015; 16(Pt A):1–6.14. Bassi C, Falconi M, Molinari E, Mantovani W, Butturini G, Gumbs AA, et al. Duct-to-mucosa versus end-to-side pancreaticojejunostomy reconstruction after pancreaticoduodenectomy: results of a prospective randomized trial. Surgery. 2003; 134:766–771.15. Raman SP, Horton KM, Cameron JL, Fishman EK. CT after pancreaticoduodenectomy: spectrum of normal findings and complications. AJR Am J Roentgenol. 2013; 201:2–13.16. Ben-Ishay O, Assi Z, Kluger Y. Pancreaticojejunostomy: images of an invagination technique. JOP. 2010; 11:642–643.17. Lepanto L, Gianfelice D, Déry R, Dagenais M, Lapointe R, Roy A. Postoperative changes, complications, and recurrent disease after Whipple's operation: CT features. AJR Am J Roentgenol. 1994; 163:841–846.18. Zhu F, Wang M, Wang X, Tian R, Shi C, Xu M, et al. Modified technique of pancreaticogastrostomy for soft pancreas with two continuous hemstitch sutures: a single-center prospective study. J Gastrointest Surg. 2013; 17:1306–1311.19. Xiong JJ, Tan CL, Szatmary P, Huang W, Ke NW, Hu WM, et al. Meta-analysis of pancreaticogastrostomy versus pancreaticojejunostomy after pancreaticoduodenectomy. Br J Surg. 2014; 101:1196–1208.20. Tamm EP, Jones B, Yeo CJ, Maher MM, Cameron JL. Pancreaticogastrostomy and the Whipple procedure: radiographic appearance and complications. Radiology. 1995; 196:251–255.21. Parikh PY, Lillemoe KD. Surgical management of pancreatic cancer--distal pancreatectomy. Semin Oncol. 2015; 42:110–122.22. Trottman P, Swett K, Shen P, Sirintrapun J. Comparison of standard distal pancreatectomy and splenectomy with radical antegrade modular pancreatosplenectomy. Am Surg. 2014; 80:295–300.23. Strasberg SM, Fields R. Left-sided pancreatic cancer: distal pancreatectomy and its variants: radical antegrade modular pancreatosplenectomy and distal pancreatectomy with celiac axis resection. Cancer J. 2012; 18:562–570.24. Warshaw AL. Distal pancreatectomy with preservation of the spleen. J Hepatobiliary Pancreat Sci. 2010; 17:808–812.25. Ferrone CR, Konstantinidis IT, Sahani DV, Wargo JA, Fernandez-del Castillo C, Warshaw AL. Twenty-three years of the Warshaw operation for distal pancreatectomy with preservation of the spleen. Ann Surg. 2011; 253:1136–1139.26. Crippa S, Tamburrino D, Partelli S, Salvia R, Germenia S, Bassi C, et al. Total pancreatectomy: indications, different timing, and perioperative and long-term outcomes. Surgery. 2011; 149:79–86.27. Santoro R. Total pancreatectomy: indications, technique, and postoperative problems. In : Siquini W, editor. Surgical treatment of pancreatic disease. Milan: Springer Milan;2009. p. 337–348.28. Gavazzi F, Zerbi A, Di Carlo V. Indications for surgery and surgical procedures for chronic pancreatitis. In : Siquini W, editor. Surgical treatment of pancreatic disease. Milan: Springer Milan;2009. p. 127–137.29. Aghdassi AA, Mayerle J, Kraft M, Sielenkämper AW, Heidecke CD, Lerch MM. Pancreatic pseudocysts--when and how to treat? HPB (Oxford). 2006; 8:432–441.30. Maithel SK, Fong Y. Technical aspects of performing transduodenal ampullectomy. J Gastrointest Surg. 2008; 12:1582–1585.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Evaluation of Computed Tomography in Traumatic Injury of Pancreas
- Pancreatic Tumors: Emphasis on CT Findings and Pathologic Classification
- CT Findings of Normal Pancreatic Tail: Variety of Morphology and Location
- A Case of Pancreatic Pseudocyst in the Left Hepatic Lobe
- Pancreas Neuroendocrine Tumor and Its Mimics: Review of Cross-Sectional Imaging Findings for Differential Diagnosis
