The Effects of Breathing Motion on DCE-MRI Images: Phantom Studies Simulating Respiratory Motion to Compare CAIPIRINHA-VIBE, Radial-VIBE, and Conventional VIBE
- Affiliations
-
- 1Department of Radiology and Research Institute of Radiology, Asan Medical Center, University of Ulsan College of Medicine, Seoul 05505, Korea. kyungwon_kim@amc.seoul.kr
- 2Department of Radiology, Yonsei University College of Medicine, Severance Hospital, Seoul 03722, Korea.
- 3Department of Radiology, Ajou Unversity School of Medicine, Suwon 16499, Korea.
- 4Department of Radiology, Ulsan University Hospital, Ulsan 44033, Korea.
- 5Siemens Healthcare Korea, Seoul 03737, Korea.
- 6MR Application Predevelopment, Siemens Healthcare, Erlangen 91052, Germany.
- KMID: 2427941
- DOI: http://doi.org/10.3348/kjr.2017.18.2.289
Abstract
OBJECTIVE
To compare the breathing effects on dynamic contrast-enhanced (DCE)-MRI between controlled aliasing in parallel imaging results in higher acceleration (CAIPIRINHA)-volumetric interpolated breath-hold examination (VIBE), radial VIBE with k-space-weighted image contrast view-sharing (radial-VIBE), and conventional VIBE (c-VIBE) sequences using a dedicated phantom experiment.
MATERIALS AND METHODS
We developed a moving platform to simulate breathing motion. We conducted dynamic scanning on a 3T machine (MAGNETOM Skyra, Siemens Healthcare) using CAIPIRINHA-VIBE, radial-VIBE, and c-VIBE for six minutes per sequence. We acquired MRI images of the phantom in both static and moving modes, and we also obtained motion-corrected images for the motion mode. We compared the signal stability and signal-to-noise ratio (SNR) of each sequence according to motion state and used the coefficients of variation (CoV) to determine the degree of signal stability.
RESULTS
With motion, CAIPIRINHA-VIBE showed the best image quality, and the motion correction aligned the images very well. The CoV (%) of CAIPIRINHA-VIBE in the moving mode (18.65) decreased significantly after the motion correction (2.56) (p < 0.001). In contrast, c-VIBE showed severe breathing motion artifacts that did not improve after motion correction. For radial-VIBE, the position of the phantom in the images did not change during motion, but streak artifacts significantly degraded image quality, also after motion correction. In addition, SNR increased in both CAIPIRINHA-VIBE (from 3.37 to 9.41, p < 0.001) and radial-VIBE (from 4.3 to 4.96, p < 0.001) after motion correction.
CONCLUSION
CAIPIRINHA-VIBE performed best for free-breathing DCE-MRI after motion correction, with excellent image quality.
Keyword
MeSH Terms
Figure
-
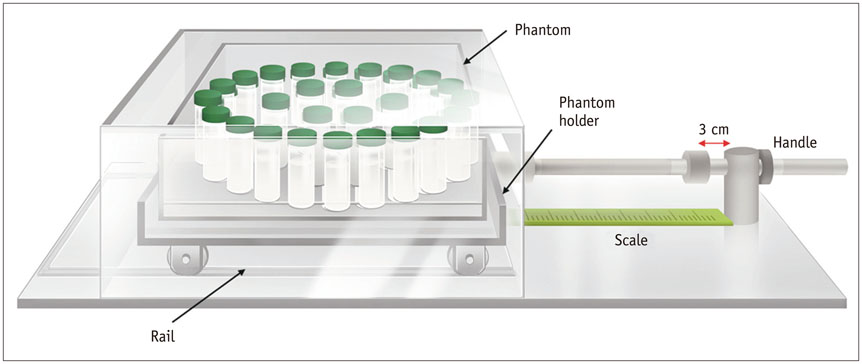
Fig. 1 Schematic figure of DCE-MRI phantom and moving platform. Moving platform consists of phantom holder with wheels, plastic cover box, handle, and rail; MR body coil (not illustrated) was placed on top of cover box. Well-trained researcher manually moved moving platform. DCE-MRI = dynamic contrast-enhanced-magnetic resonance imaging
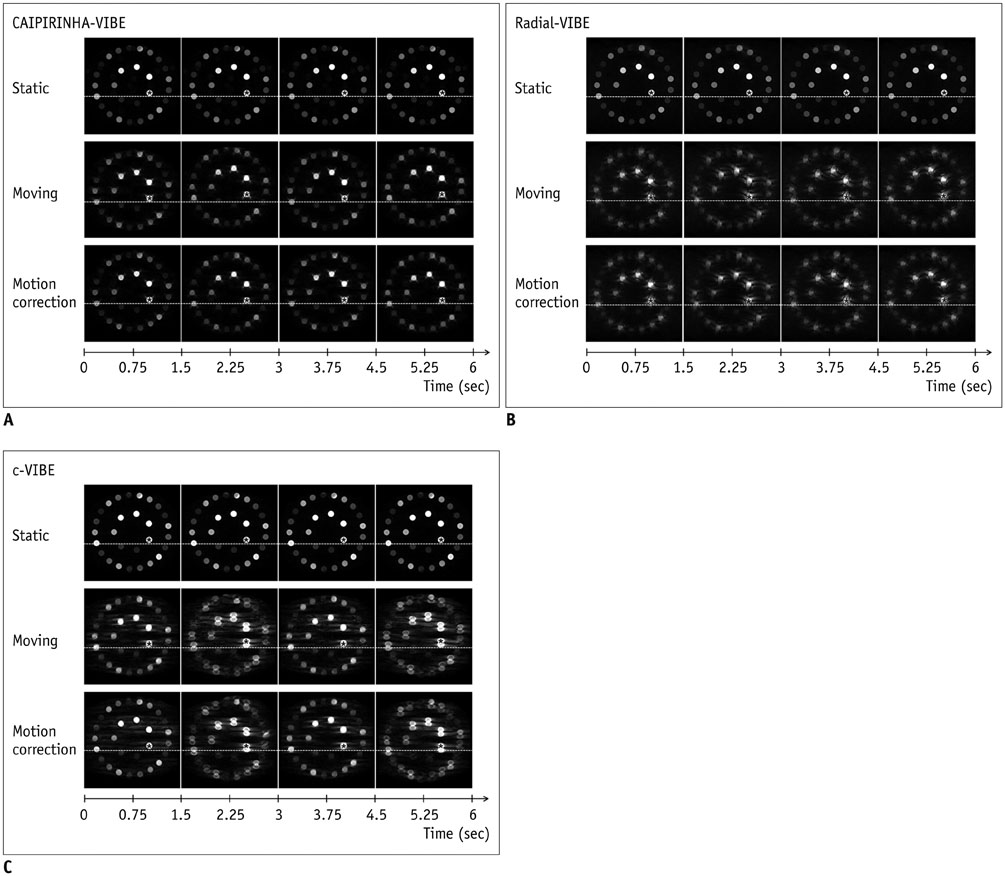
Fig. 2 Captured MRI images of dynamic scanning using each sequence according to motion mode. Each four-image set was arranged in horizontal axis along time points (6 seconds, 1 respiratory cycle in this study). We drew white dotted line below tube (asterisks) that contained highest concentrations of NiCl2 to clearly demonstrate movement. A. MRI images using CAIPIRINHA-VIBE. For static mode (upper row), phantom showed stable location without any artifact. For moving mode (middle row), MR images obtained using CAIPIRINHA-VIBE showed vertical phantom displacement with mildly distorted tube shapes. After motion correction (lower row), phantom displacement had decreased markedly, with remaining ghosting artifacts around each tube. B. MRI images using radial-VIBE. For static mode (upper row), phantom also showed stable location without any artifact. For both moving (middle row) and motion-corrected (lower row) modes, MR images did not show significant displacement of phantom. However, round shape of each tube was significantly distorted due to streak artifacts on radial-VIBE, and these streak artifacts did not grossly improve after motion correction. C. MRI images using c-VIBE. For static mode (upper row), phantom also showed stable location without any artifact. For moving mode (middle row), MR images obtained using c-VIBE showed vertical phantom motion with related artifacts; true image of each tube overlapped with after-image of each tube, which disrupted original round shape. Neither displacement due to motion nor motion-related artifacts significantly improved after motion correction (lower row). c-VIBE = conventional VIBE, CAIPIRINHA = controlled aliasing in parallel imaging results in higher acceleration, VIBE = volumetric interpolated breath-hold examination

Fig. 3 Graphs and CoV (%) for signal stability of each MRI sequence. Signal intensities, which were obtained using each sequence, are plotted along dynamic series over six minutes. Each colored line indicates signal intensities according to motion mode, i.e., blue line, static mode; green line, moving mode; red line, motion-corrected mode. For all three sequences, signal intensities at static mode (blue lines) were stable without variation. Small CoVs, which are close to 0, indicate that variations in MRI signal intensities were negligible, thus suggesting better signal stability. A. CAIPIRINHA-VIBE. Signal intensities for moving mode (green line) showed periodical vertical fluctuations. In motion-corrected mode (red line), variations in signal intensities observed in moving mode had decreased greatly. CoVs in static, moving, and motion-corrected modes were 0.09, 18.65, and 2.56, respectively. B. Radial-VIBE. Variations in signal intensities in radial-VIBE in moving mode (green line) were less prominent than those in CAIPIRINHA-VIBE or c-VIBE; however, these variations in signal intensities did not decrease after motion correction (red line). CoVs for static, moving, and motion-corrected modes were 0.03, 8.90, and 15.84, respectively. C. c-VIBE. Signal intensities in moving mode (green line) fluctuated up and down over time, and with motion correction (red line), variations in signal intensities observed in moving mode did not significantly decrease. CoVs in static, moving, and motion-corrected modes were 0.21, 12.91, and 12.50, respectively. c-VIBE = conventional VIBE, CAIPIRINHA = controlled aliasing in parallel imaging results in higher acceleration, CoV = coefficients of variation, MOCO = motion correction, VIBE = volumetric interpolated breath-hold examination
Cited by 1 articles
-
Rapid Imaging: Recent Advances in Abdominal MRI for Reducing Acquisition Time and Its Clinical Applications
Jeong Hee Yoon, Marcel Dominik Nickel, Johannes M. Peeters, Jeong Min Lee
Korean J Radiol. 2019;20(12):1597-1615. doi: 10.3348/kjr.2018.0931.
Reference
-
1. Thng CH, Koh TS, Collins DJ, Koh DM. Perfusion magnetic resonance imaging of the liver. World J Gastroenterol. 2010; 16:1598–1609.2. Kim KW, Lee JM, Jeon YS, Kang SE, Baek JH, Han JK, et al. Free-breathing dynamic contrast-enhanced MRI of the abdomen and chest using a radial gradient echo sequence with k-space weighted image contrast (KWIC). Eur Radiol. 2013; 23:1352–1360.3. Kim B, Lee CK, Seo N, Lee SS, Kim JK, Choi Y, et al. Comparison of CAIPIRINHA-VIBE, Radial-VIBE, and conventional VIBE sequences for dynamic contrast-enhanced (DCE) MRI: a validation study using a DCE-MRI phantom. Magn Reson Imaging. 2016; 34:638–644.4. Hintze C, Stemmer A, Bock M, Kuder TA, Risse F, Dinkel J, et al. A hybrid breath hold and continued respiration-triggered technique for time-resolved 3D MRI perfusion studies in lung cancer. Rofo. 2010; 182:45–52.5. Breuer FA, Blaimer M, Mueller MF, Seiberlich N, Heidemann RM, Griswold MA, et al. Controlled aliasing in volumetric parallel imaging (2D CAIPIRINHA). Magn Reson Med. 2006; 55:549–556.6. McKenzie CA, Lim D, Ransil BJ, Morrin M, Pedrosa I, Yeh EN, et al. Shortening MR image acquisition time for volumetric interpolated breath-hold examination with a recently developed parallel imaging reconstruction technique: clinical feasibility. Radiology. 2004; 230:589–594.7. Vogt FM, Antoch G, Hunold P, Maderwald S, Ladd ME, Debatin JF, et al. Parallel acquisition techniques for accelerated volumetric interpolated breath-hold examination magnetic resonance imaging of the upper abdomen: assessment of image quality and lesion conspicuity. J Magn Reson Imaging. 2005; 21:376–382.8. AlObaidy M, Ramalho M, Busireddy KK, Liu B, Burke LM, Altun E, et al. High-resolution 3D-GRE imaging of the abdomen using controlled aliasing acceleration technique-a feasibility study. Eur Radiol. 2015; 25:3596–3605.9. Jackson E. Technical Committee MR Phantom Development/Data Efforts. Web site. Accessed January 21, 2017. http://qibawiki.rsna.org/images/3/34/RSNA_QIBA_May2010_MR_Phantom.pdf.10. Lin W, Guo J, Rosen MA, Song HK. Respiratory motion-compensated radial dynamic contrast-enhanced (DCE)-MRI of chest and abdominal lesions. Magn Reson Med. 2008; 60:1135–1146.11. Chandarana H, Block TK, Rosenkrantz AB, Lim RP, Kim D, Mossa DJ, et al. Free-breathing radial 3D fat-suppressed T1-weighted gradient echo sequence: a viable alternative for contrast-enhanced liver imaging in patients unable to suspend respiration. Invest Radiol. 2011; 46:648–653.12. Song HK, Dougherty L. Dynamic MRI with projection reconstruction and KWIC processing for simultaneous high spatial and temporal resolution. Magn Reson Med. 2004; 52:815–824.13. Song HK, Dougherty L. k-space weighted image contrast (KWIC) for contrast manipulation in projection reconstruction MRI. Magn Reson Med. 2000; 44:825–832.14. Chefd'hotel C, Hermosillo G, Faugeras O. Flows of diffeomorphisms for multimodal image registration. In : Proceedings of the IEEE International Symposium on Biomedical Imaging; Piscataway, NJ: Institute of Electrical and Electronics Engineers;2002. p. 753–756.15. Reed GF, Lynn F, Meade BD. Use of coefficient of variation in assessing variability of quantitative assays. Clin Diagn Lab Immunol. 2002; 9:1235–1239.16. Dietrich O, Raya JG, Reeder SB, Reiser MF, Schoenberg SO. Measurement of signal-to-noise ratios in MR images: influence of multichannel coils, parallel imaging, and reconstruction filters. J Magn Reson Imaging. 2007; 26:375–385.17. Sodickson DK, Griswold MA, Jakob PM, Edelman RR, Manning WJ. Signal-to-noise ratio and signal-to-noise efficiency in SMASH imaging. Magn Reson Med. 1999; 41:1009–1022.18. Reeder SB, Wintersperger BJ, Dietrich O, Lanz T, Greiser A, Reiser MF, et al. Practical approaches to the evaluation of signal-to-noise ratio performance with parallel imaging: application with cardiac imaging and a 32-channel cardiac coil. Magn Reson Med. 2005; 54:748–754.19. Yu MH, Lee JM, Yoon JH, Kiefer B, Han JK, Choi BI. Clinical application of controlled aliasing in parallel imaging results in a higher acceleration (CAIPIRINHA)-volumetric interpolated breathhold (VIBE) sequence for gadoxetic acid-enhanced liver MR imaging. J Magn Reson Imaging. 2013; 38:1020–1026.20. Block KT, Uecker M, Frahm J. Undersampled radial MRI with multiple coils. Iterative image reconstruction using a total variation constraint. Magn Reson Med. 2007; 57:1086–1098.21. Fujinaga Y, Ohya A, Tokoro H, Yamada A, Ueda K, Ueda H, et al. Radial volumetric imaging breath-hold examination (VIBE) with k-space weighted image contrast (KWIC) for dynamic gadoxetic acid (Gd-EOB-DTPA)-enhanced MRI of the liver: advantages over Cartesian VIBE in the arterial phase. Eur Radiol. 2014; 24:1290–1299.22. Haider CR, Riederer SJ, Borisch EA, Glockner JF, Grimm RC, Hulshizer TC, et al. High temporal and spatial resolution 3D time-resolved contrast-enhanced magnetic resonance angiography of the hands and feet. J Magn Reson Imaging. 2011; 34:2–12.23. Kim BS, Lee KR, Goh MJ. New imaging strategies using a motion-resistant liver sequence in uncooperative patients. Biomed Res Int. 2014; 2014:142658.24. Clifford MA, Banovac F, Levy E, Cleary K. Assessment of hepatic motion secondary to respiration for computer assisted interventions. Comput Aided Surg. 2002; 7:291–299.25. Suramo I, Päivänsalo M, Myllylä V. Cranio-caudal movements of the liver, pancreas and kidneys in respiration. Acta Radiol Diagn (Stockh). 1984; 25:129–131.26. Korin HW, Ehman RL, Riederer SJ, Felmlee JP, Grimm RC. Respiratory kinematics of the upper abdominal organs: a quantitative study. Magn Reson Med. 1992; 23:172–178.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Morphologic Evaluation of Primary Non-Small Cell Lung Cancer by 3 Tesla MRI with Free-Breathing Ultrashort Echo Time and Radial T1-Weighted Gradient Echo Sequences: A Comparison with CT Analysis
- Contrast-Enhanced Three-Dimensional MR Imaging Using a Volumetric Interpolated Breath-hold Examination (VIBE): Clinical Utility in the Evaluation of Renal Tumors
- Feasibility of Quadruple Arterial Phase of Motion Insensitive Radial Volumetric Imaging Breath-Hold Examination with k-Space Weighted Image Contrast in the Detection of Hepatocellular Carcinoma in Patients with Chronic Liver Disease
- The Usefulness of High-Resolution Three-Dimensional Dynamic MR Imaging with Sensitivity Encoding for Evaluating Extrahepatic Bile Duct Cancer
- Bendamustine in combination with ifosfamide, etoposide, and vinorelbine (VIBE) is an effective salvage regimen for heavily pre-treated patients with relapsed or refractory Hodgkin lymphoma: a single-center experience
