Retrograde Suction Decompression with an Inahara Carotid Shunt for Clipping a Large Distal Internal Carotid Artery Aneurysm
- Affiliations
-
- 1Department of Neurosurgery, Chung-Ang University Hospital, Seoul, Korea. nsnam@cau.ac.kr
- KMID: 2427136
- DOI: http://doi.org/10.3349/ymj.2017.58.2.449
Abstract
- We describe a technique to clip a large internal carotid artery (ICA) aneurysm via a retrograde suction decompression (RSD). A large aneurysm in the right distal ICA involving the bifurcation region measuring 1.2×1.1×0.7 cm with posterior projection was managed with assisted RSD technique. The anterior choroidal artery emerged from the side wall of the aneurysm. An Inahara shunt was inserted into the ICA with neck dissection, and RSD was applied after completely clipping the aneurysm. RSD with an Inahara carotid shunt is useful for complete visualization of the aneurysm, including its surrounding structures, and for proximal control of the parent vessels, subsequently achieving satisfactory clip placement.
Keyword
MeSH Terms
Figure
-
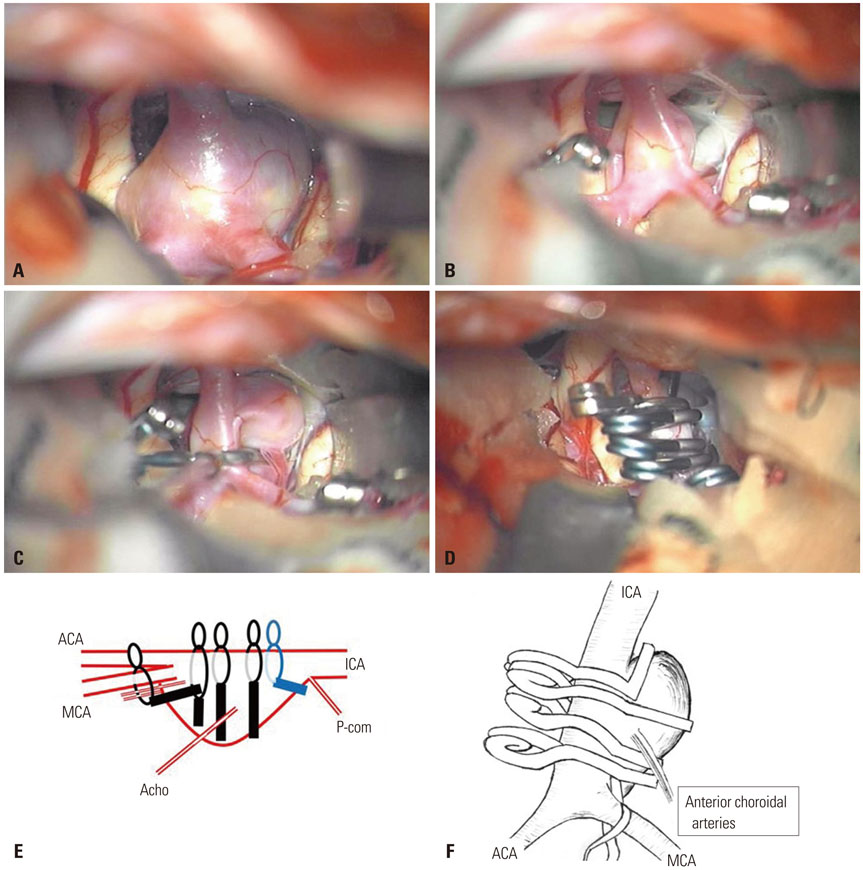
Fig. 1 (A) Intraoperative photographs of a large aneurysm located in the right distal internal carotid artery. (B) After retrograde suction decompression, the aneurysm was deflated. (C) The anterior choroidal artery arising from the side wall of the aneurysm. (D) Clipping with 5 fenestrated clips. (E) Diagram of the 5 fenestration clips. (F) Illustrations of clip placement. ICA, internal carotid artery; ACA, anterior cerebral artery; MCA, middle cerebral artery.

Fig. 2 The process of retrograde suction decompression through the internal carotid artery with a Pruitt-Inahara® carotid shunt. (A) Neck dissection was performed to expose the common carotid artery (CCA). Proximal and distal vascular loops entwine the CCA. A purse string suture is placed midway between the two loops. (B) The Pruitt-Inahara® carotid shunt catheter was inserted into the internal carotid artery (ICA) through the incision at the center of the purse string suture. (C) Illustrations of the technique.
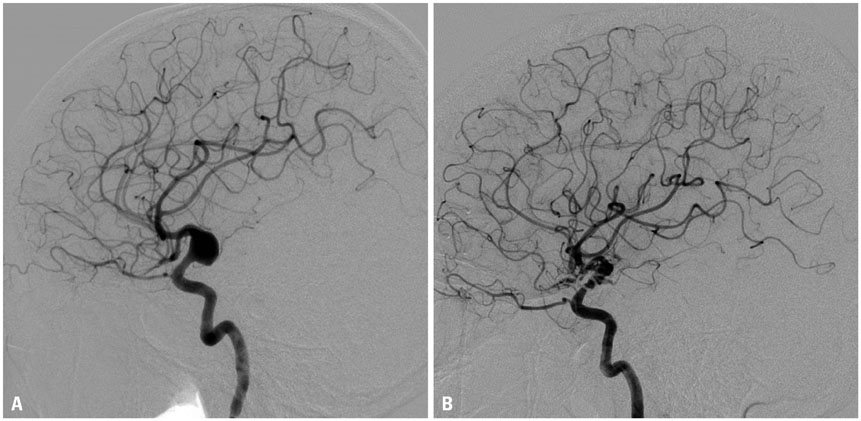
Fig. 3 Pre (A) and post (B) operative angiograms of the aneurysm. (A) Fusiform dilation of the distal internal carotid artery and eccentric posterior aneurysmal formation measuring 1.2×1.1×0.7 cm. The right M1 and A1 portions were incorporated and the aneurysm was located just distal to the orifice of the posterior communicating artery. The anterior choroidal artery emerged from the side wall of the aneurysm. (B) The aneurysm was completely secured and the anterior choroidal artery was preserved.
Reference
-
1. Batjer HH, Samson DS. Retrograde suction decompression of giant paraclinoidal aneurysms. Technical note. J Neurosurg. 1990; 73:305–306.2. Tamaki N, Kim S, Ehara K, Asada M, Fujita K, Taomoto K, et al. Giant carotid-ophthalmic artery aneurysms: direct clipping utilizing the “trapping-evacuation” technique. J Neurosurg. 1991; 74:567–572.
Article3. Fan YW, Chan KH, Lui WM, Hung KN. Retrograde suction decompression of paraclinoid aneurysm--a revised technique. Surg Neurol. 1999; 51:129–131.
Article4. Mattingly T, Kole MK, Nicolle D, Boulton M, Pelz D, Lownie SP. Visual outcomes for surgical treatment of large and giant carotid ophthalmic segment aneurysms: a case series utilizing retrograde suction decompression (the “Dallas technique”). J Neurosurg. 2013; 118:937–946.
Article5. Xu BN, Sun ZH, Jiang JL, Wu C, Zhou DB, Yu XG, et al. Surgical management of large and giant intracavernous and paraclinoid aneurysms. Chin Med J (Engl). 2008; 121:1061–1064.
Article6. Arnautovic´ KI, Al-Mefty O, Angtuaco E. A combined microsurgical skull-base and endovascular approach to giant and large paraclinoid aneurysms. Surg Neurol. 1998; 50:504–518.
Article7. Steiger HJ, Lins F, Mayer T, Schmid-Elsaesser R, Stummer W, Turowski B. Temporary aneurysm orifice balloon occlusion as an alternative to retrograde suction decompression for giant paraclinoid internal carotid artery aneurysms: technical note. Neurosurgery. 2005; 56:2 Suppl. E442.
Article8. Hoh DJ, Larsen DW, Elder JB, Kim PE, Giannotta SL, Liu CY. Novel use of an endovascular embolectomy device for retrograde suction decompression-assisted clip ligation of a large paraclinoid aneurysm: technical case report. Neurosurgery. 2008; 62:5 Suppl 2. ONSE412–ONSE413.
Article9. Fulkerson DH, Horner TG, Payner TD, Leipzig TJ, Scott JA, Denardo AJ, et al. Endovascular retrograde suction decompression as an adjunct to surgical treatment of ophthalmic aneurysms: analysis of risks and clinical outcomes. Neurosurgery. 2009; 64:3 Suppl. ons107–ons111.
Article10. Mizoi K, Takahashi A, Yoshimoto T, Fujiwara S, Koshu K. Combined endovascular and neurosurgical approach for paraclinoid internal carotid artery aneurysms. Neurosurgery. 1993; 33:986–992.
Article11. Pruitt JC, Morales RE. Carotid endarterectomy: a report of 7854 procedures using local anesthesia, electroencephalographic monitoring, occlusion catheters, and the pruitt-inahara carotid shunt. Surg Technol Int. 1995; IV:325–332.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Surgical Experience of Carotid Pseudoaneurysm
- Surgical Experience of the Distal Internal Carotid Artery Aneurysm
- Aneurysm at the Origin of the Uncal Artery Arising from the Internal Carotid Artery
- Giant Aneurysm of Internal Carotid Artery: Three cases report
- Five Aneurysms Arising from the Ipsilateral Internal Carotid Artery : Case Report
