Outcomes of Cephalomedullary Nailing in Basicervical Fracture
- Affiliations
-
- 1Department of Orthopedic Surgery, Wonkwang University School of Medicine, Iksan, Korea. osksh@wonkwang.ac.kr
- KMID: 2424254
- DOI: http://doi.org/10.5371/hp.2017.29.4.270
Abstract
- PURPOSE
A basicervical femoral fracture is defined as a fracture of base of neck of femur that occurs medially from intertrochanteric line above lesser trochanter. In this study, we intended to evaluate radiological and clinical results of basicervical femoral fractures treated by intramedullary nailing.
MATERIALS AND METHODS
Fifteen patients, who underwent intramedullary nailing among 50 patients, out of 50 who were diagnosed with basicervical femoral fractures from July 2012 to May 2015 were studied. All of 15 patients' fracture were two-part basicervical fractures. Using radiography, we characterized the: i) state of reduction, ii) location of the lag screw, iii) tip apex distance (TAD), and iv) sliding distance of lag screw and bone union. Additionally, we performed clinical assessment before injury and at final follow-up.
RESULTS
In radiological assessment, we achieved acceptable reduction state in all patients. All lag screws were fixated on appropriate locations. Mean TAD was 17.3 mm (11.0-21.1 mm), which showed insertion point of < 25 mm in all cases. The mean sliding distance of the lag screw was 5.1 mm (0.1-16.0 mm) at the final follow-up. The mean bone union period was 4.8 months (3-10 months) with achieving in all cases. In clinical assessment, Harris hip score, visual analogue scale score and Western Ontario and McMaster Universities Arthritis Index score, all of them significantly improved postoperatively compared with preoperative scores (P < 0.05).
CONCLUSION
In elderly patients with basicervical femoral fractures, treatment with intramedullary nailing showed satisfactory results, considered to be a useful method if performed with skilled technique.
MeSH Terms
Figure
-
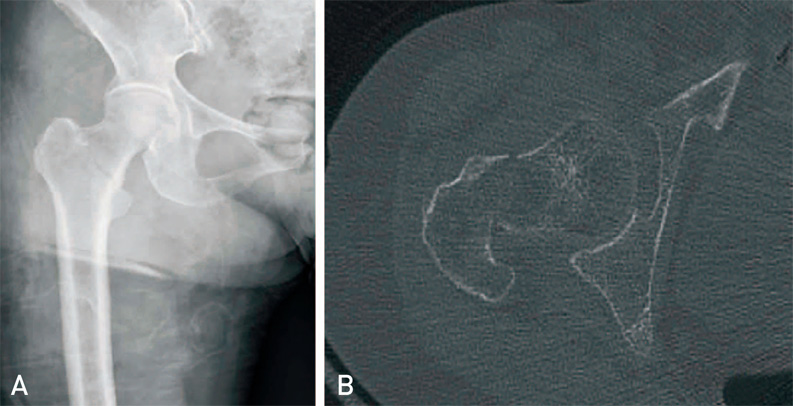
Fig. 1 Images of an female patient aged 90 years old. (A) Anteroposterior X-ray shows a basicervical fracture in the right hip that had occurred after a simple fall. (B) Computed tomography shows the axial section of fracture level.
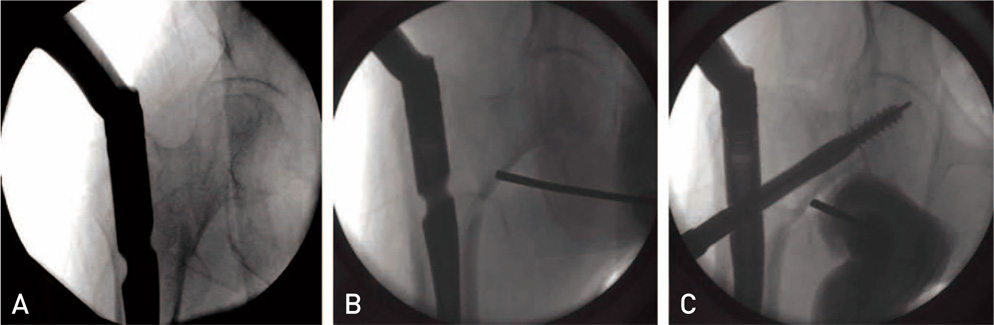
Fig. 2 During insertion of an intramedullary nail's massive empennage, there is a distraction effect (V effect) on the trochanteric fragments, which increases the incidence of hip varus deformity or nonunion (A). With the assistant holding the proximal-medial part of basicervical fracture line in position (B), a reamer with high rotation speed can be used to enlarge the proximal femur; this diminishes the V effect and lag screw malposition (C).
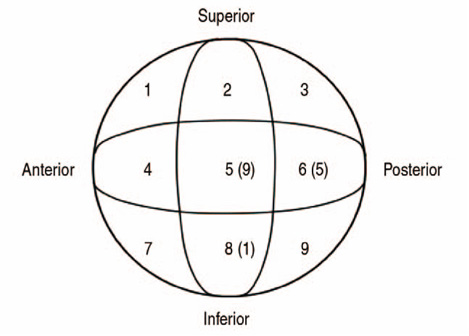
Fig. 3 For the Cleveland index, the femur head is divided into nine zones in the axial view to classify the position of the cervical screw.

Fig. 4 (A) Initial radiograph in 77-year-old female patient show a basicervical fracture in the left hip. (B) Immediate postoperative radiograph shows that fixation was done with Gamma. (C) Radiograph at 12 months shows the bone union at the fracture site.
Cited by 1 articles
-
Outcomes of Combined Neck and Trochanter Fractures of the Femur Treated with Cephallomedullary Nail in Elderly
Hyunseung Yoo, Youngho Cho, Seongmun Hwang
Hip Pelvis. 2019;31(4):200-205. doi: 10.5371/hp.2019.31.4.200.
Reference
-
1. Lieberman JR. AAOS comprehensive orthopaedic review. Rosemont, IL: American Academy of Orthopaedic Surgeons;2009. p. 597–598.2. Saarenpää I, Partanen J, Jalovaara P. Basicervical fracture--a rare type of hip fracture. Arch Orthop Trauma Surg. 2002; 122:69–72.3. Blair B, Koval KJ, Kummer F, Zuckerman JD. Basicervical fractures of the proximal femur. A biomechanical study of 3 internal fixation techniques. Clin Orthop Relat Res. 1994; (306):256–263.4. Deneka DA, Simonian PT, Stankewich CJ, Eckert D, Chapman JR, Tencer AF. Biomechanical comparison of internal fixation techniques for the treatment of unstable basicervical femoral neck fractures. J Orthop Trauma. 1997; 11:337–343.
Article5. Dossick PH, Dorr LD, Gruen T, Saberi MT. Techniques for preoperative planning and postoperative evaluation of noncemented hip arthroplasty. Tech Orthop. 1991; 6(3):1–6.
Article6. Parker MJ, Pryor GA, Thorngren KG. Extramedullary fixation of extracapsular fractures. In : Parker MJ, Pryor GA, Thorngren KG, editors. Handbook of hip fracture surgery. Oxford: Butterworth-Heinemann;1997. p. 63–90.7. Kim KW, Ahn SH. Elderly trochanteric fractures: principles of treatment. J Korean Soc Fract. 1994; 7:227–234.
Article8. Yoon ES, Min HJ, Suh JS, et al. Comparison of clinical results between bipolar hemiarthroplasty and compression hip screw on unstable intertrochanteric fractures of the femur in elderly patients. J Korean Fract Soc. 2004; 17:214–220.
Article9. Gill JM, Johnson GR, Sher JL, Kornjaca NA. Biomechanical aspects of the repair of intertrochanteric fractures. J Biomed Eng. 1989; 11:235–239.
Article10. Ly TV, Swiontkowski MF. Management of femoral neck fractures in young adults. Indian J Orthop. 2008; 42:3–12.
Article11. Jones HW, Johnston P, Parker M. Are short femoral nails superior to the sliding hip screw? A meta-analysis of 24 studies involving 3,279 fractures. Int Orthop. 2006; 30:69–78.
Article12. Parker MJ, Handoll HH. Gamma and other cephalocondylic intramedullary nails versus extramedullary implants for extracapsular hip fractures in adults. Cochrane Database Syst Rev. 2008; (3):CD000093.
Article13. Hu SJ, Yu GR, Zhang SM. Surgical treatment of basicervical intertrochanteric fractures of the proximal femur with cephalomeduallary hip nails. Orthop Surg. 2013; 5:124–129.
Article14. Tasyikan L, Ugutmen E, Sanel S, Soylemez MS, Ozkan K, Solakoglu C. Short-term results of surgical treatment with cephalomedullary nails for basicervical proximal femoral fractures. Acta Orthop Belg. 2015; 81:427–434.15. Fogagnolo F, Kfuri M Jr, Paccola CA. Intramedullary fixation of pertrochanteric hip fractures with the short AO-ASIF proximal femoral nail. Arch Orthop Trauma Surg. 2004; 124:31–37.
Article16. Cleveland M, Bosworth DM, Thompson FR, Wilson HJ Jr, Ishizuka T. A ten-year analysis of intertrochanteric fractures of the femur. J Bone Joint Surg Am. 1959; 41-A:1399–1408.
Article17. Baumgaertner MR, Curtin SL, Lindskog DM, Keggi JM. The value of the tip-apex distance in predicting failure of fixation of peritrochanteric fractures of the hip. J Bone Joint Surg Am. 1995; 77:1058–1064.
Article18. Koval KJ, Skovron ML, Aharonoff GB, Meadows SE, Zuckerman JD. Ambulatory ability after hip fracture. A prospective study in geriatric patients. Clin Orthop Relat Res. 1995; (310):150–159.19. Koval KJ, Zuckerman JD. Functional recovery after fracture of the hip. J Bone Joint Surg Am. 1994; 76:751–758.
Article20. Su BW, Heyworth BE, Protopsaltis TS, et al. Basicervical versus intertrochanteric fractures: an analysis of radiographic and functional outcomes. Orthopedics. 2006; 29:919–925.
Article21. Watson ST, Schaller TM, Tanner SL, Adams JD, Jeray KJ. Outcomes of low-energy basicervical proximal femoral fractures treated with cephalomedullary fixation. J Bone Joint Surg Am. 2016; 98:1097–1102.
Article22. Skála-Rosenbaum J, Bartonícek J, Bartoska R. Is distal locking with IMHN necessary in every pertrochanteric fracture? Int Orthop. 2010; 34:1041–1047.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Cephalomedullary Nailing with an Additional Cannulated Screw Fixation in Basicervical Femur Fractures
- Incidence and Risk Factors of Osteonecrosis of the Femoral Head after Cephalomedullary Nailing for Pertrochanteric Fractures: Observational Single-Center Study
- Risk Factors Associated with Failure of Cephalomedullary Nail Fixation in the Treatment of Trochanteric Hip Fractures
- Cephalomedullary Nailing versus Dynamic Hip Screw Fixation in Basicervical Femoral Neck Fracture: A Systematic Review and Meta-Analysis
- Review on Basicervical Femoral Neck Fracture: Definition, Treatments, and Failures
