The Treatment of Grade 3 Acute Acromioclavicular Joint Injuries with Modified Neviaser Technique
- KMID: 2423596
- DOI: http://doi.org/10.4055/jkoa.1996.31.2.205
Abstract
- There has been considerable controversy in the treatment of acute grade 3 injuries of acromioclavicular joint. Neviaser reported that the possibility of a latent degenerative arthritis occurring in the acromioclavicular joint as the result of passing Kirschner wire through the joint was more theoretical than real and any changes that may take place in the acromioclavicular joint were the result of trauma. The acromioclavicular joint and the articular disc were not disturbed at the time of operation in Neviaser technique, but we excised the articular disc that were torn for the purpose of preventing acromioclavicular joint from degenerative arthritis. We had treated 26 cases of grade 3 injuries of acromioclavicular joint with modified Neviaser technique from June 1990 to May 1994 at the Pohang St. Mary's Hospital. The results were as follows. 1. The clinical results by Weitzman were consisted of 18 cases(69%) of excellent, 6 cases(23%) of good, 2 cases(8%) of fair and 0 case(0%) of poor. 2. Loss of reduction was 1.6mm by stress views of final reviews and didn't affect to functional result. 3. There were no cases of redislocation of acromioclavicular joint after removal of Kirschner wires. 4. There were no cases of degenerative arthritis of acromioclavicular joint in final review. There result suggest that excision of the articular disc that were torn may be helpful in preventing acromioclavicular joint from degenerative arthritis.
Figure
-
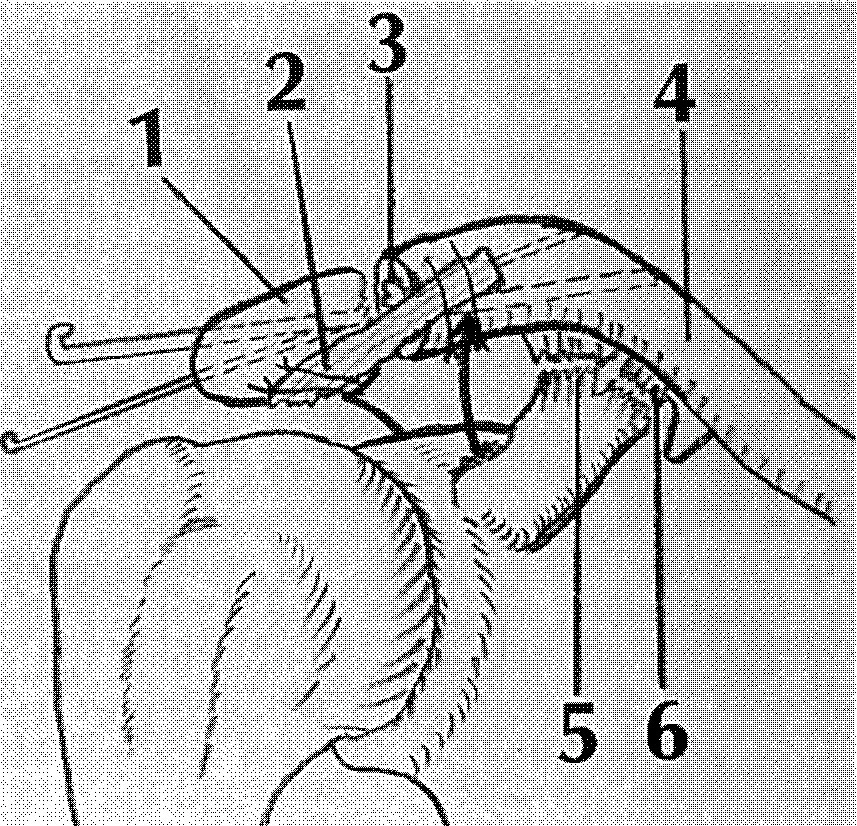
Fig. 1 Modified Neviaser technique for reconstruction of acromioclavicular ligament with coracoacromial ligament 1: Acromion 2: Coracoacromial ligament; detached from its coracoid attachment and fixed to clavicle 3: Torn articular disc of acromioclavicular joint; excised at the time of operation 4: Clavicle, 5: Trapezoid ligament, 6: Conoid ligament
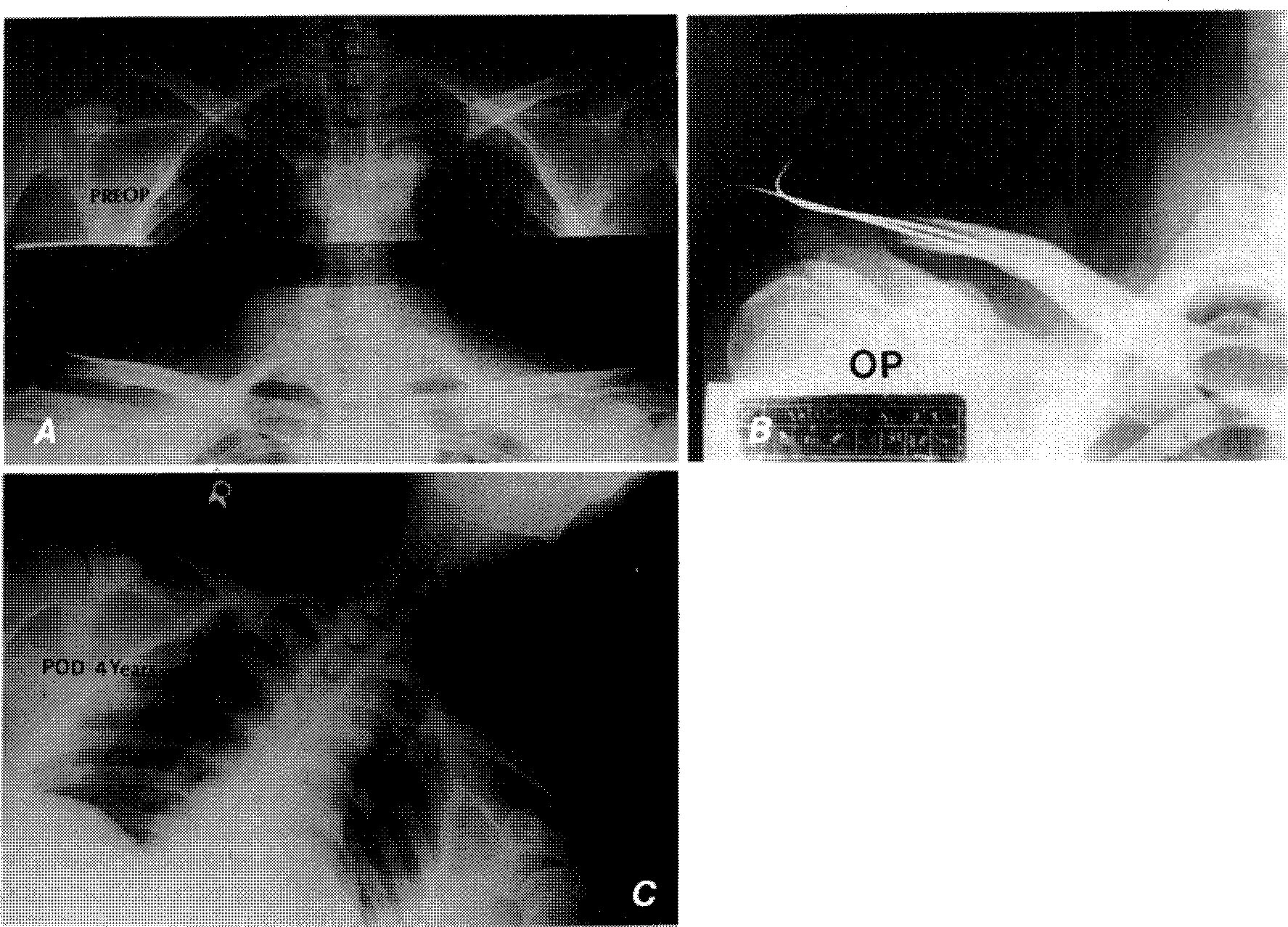
Fig. 2-A A 32-year old male patient had a grade 3 acromioclavicular joint injury to the right shoulder in initial stress view. B. The patient was managed with modified Neviaser technique. C. Roentgenogram of last follow-up at four years after surgery showed no redislocation of acromioclavicular joint and there’s no radiolucent density at distal end of the clavicle.
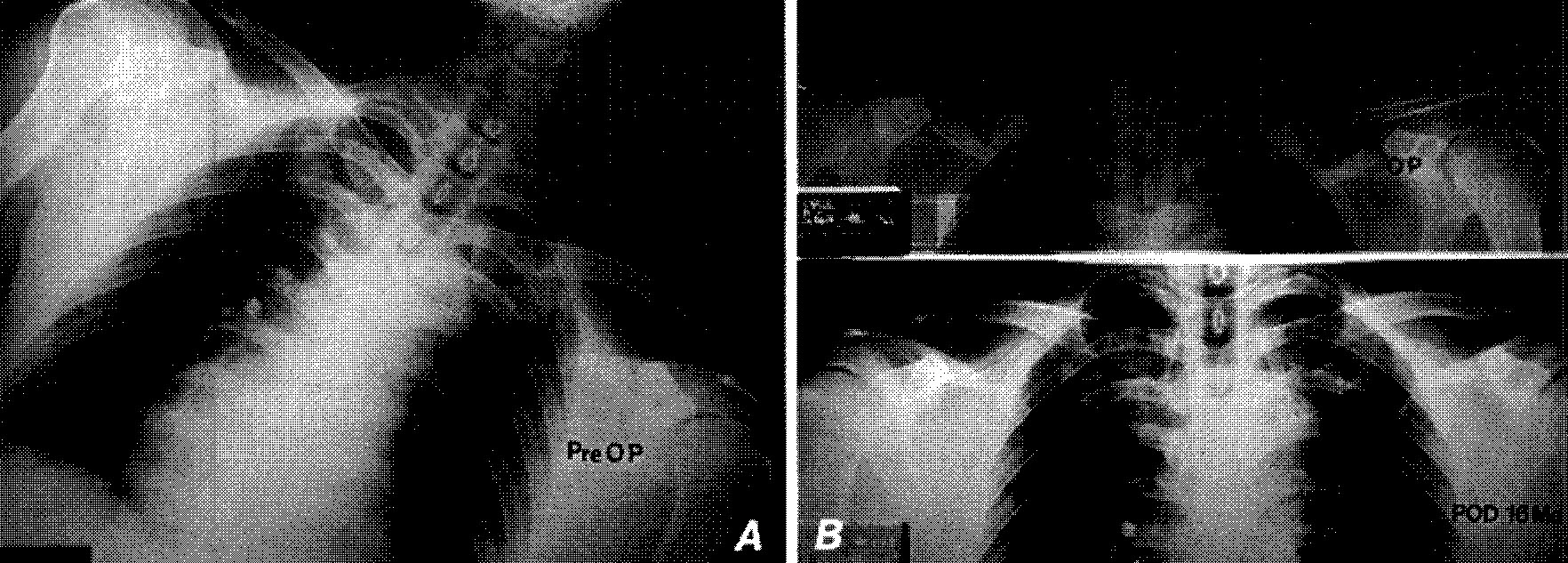
Fig. 3-A 45-year old man patient had a grade 3 acute acromioclavicular joint injury to the left shoulder in initial stress view. B. Above; The patient was managed with modified Neviaser technique. There was intraoperative fracture of lateral end of the clavicle. Below; The functional result was good. Stress view at sixteen months after surgery showed good union of lateral end of the clavicle.
Reference
-
4. Allman FL Jr. Fracture and ligamentous Injuries of the Clavicle And its articulation. J Bone Joint Surg. 1967; 49-A:774–778.5. Bateman JE. Athletic Injuries About the Shoulder on Throwing and Body-Contract Sports. Clin Orthop. 1962; 23:75–83.6. Bearden JM, Hughston JC, Whatley GS. Acromioclavicular Dislocation. Method of Treatment. J Sports Med. 1973; 1:5–17.
Article7. Bosworth BM. Acromioclavicular separation: New method of repair. Surg Gynecol Obstet. 1941; 73:866–871.8. Dewar FP, Barrington TW. The Treatment of Chronic Acromio-Clavicular Dislocation. J Bone Joint Surg. 1965; 47B:32–35.
Article9. Dias JJ, Steingolod RA, Tes-foyohannes B, Gregg PJ. The Conservative Treatment of Acromioclavicular Dislocation: Review After Five Years. J Bone Joint Surg. 1987; 69B:719–722.
Article10. Imatani RJ, Hanlon JJ, Cady GW. Acute Complete Acromioclavicular Separation. J Bone Joint Surg. 1975; 57-A:328–331.
Article11. Inman VT, Saunders JB, Abbot LC. Observation on the Function of the Shoulder Joint. J Bone Joint Surg. 1944; 26:1–30.12. Kennedy JC, Cameron H. Complete Dislocation of the Acromioclavicular Joint. J Bone Joint Surg. 1954; 36-B:202–208.
Article13. Murray JWG. Reconstruction of the Dislocated Acromioclavicular Joint: A simplified Method. Ortho Rev. 1973; 2:55–66.14. Neviaser JS. Acromioclavicular Dislocation Treated by Transference of the Coracoacromial Ligament. Bull. Hosp. Jt. Disease. 1951; 12:46–54.15. Neviaser JS. Acromioclavicular Dislocation Treated by Transference of the Coracoacromial Ligament. A Long-term Follow-up in a Series of 112 cases. Clin Ortho. 1968; 58:57–68.16. Phemister DB. The Treatment of Dislocation of the Acromioclavicular Joint by Open Reduction and Threaded-wire fixation. J Bone Joint Surg. 1941; 24:166–168.17. Rockwood CA Jr. Green : Fractures. 1991. 3rd Ed. Philadelphia: J.B. Lippincott Co.;p. 1181–1251.18. Salter EG Jr, Nasca RJ, Shelley BS. Anatomi-cal Observations on the Acromioclavicular Joint and Supporting Ligaments. Am J Sports Med. 1987; 15:199–206.
Article19. Urist MR. Complete Dislocation of the Acromioclavicular Joint, The Nature of the Traumatic Lesion and Effective Methods of Treatment and Analysis of 41 Cases. J Bone Joint Surg. 1946; 28:818–837.20. Weaver JD, Dunn HK. Treatment of Acromio-clavicular Injuries, Especially Complete Acromio-clavicular Separation. J Bone Joint Surg. 1972; 54-A:1187–1197.21. Weitzman G. Treatment of Acute Acromioclavicular Joint Dislocation by a Modified Bosworth Method. J Bone Joint Surg,. 1967; 49-A:1167–1178.
Article22. Zaricznjy B. Late Reconstruction of the Ligaments Following Acromiclavicular Separation. J Bone Joint Surg. 1976; 58-A:792–795.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Treatment of Acromioclavicular separation
- The Treatment of Acromioclavicular Separation
- The Treatment of Acromioclayicular Dislocation Comparison Study between Modified Bosworth and Phemister Technique
- Treatment of acute high-grade acromioclavicular joint dislocation
- Surgical Treatment of Acute acromioclavicular Dislocation
