Pediatr Gastroenterol Hepatol Nutr.
2018 Oct;21(4):361-364. 10.5223/pghn.2018.21.4.361.
Accessory Hepatic Lobe: A Rare Cause of Prehepatic Portal Hypertension in a Child
- Affiliations
-
- 1Department of Pediatric Gastroenterology, Hepatology and Nutrition, Faculty of Medicine, Karadeniz Technical University, Trabzon, Turkey. drturkmen61@ gmail.com
- 2Department of Radiology, Faculty of Medicine, Karadeniz Technical University, Trabzon, Turkey.
- 3Department of Pediatric Surgery, Faculty of Medicine, Karadeniz Technical University, Trabzon, Turkey.
- KMID: 2422002
- DOI: http://doi.org/10.5223/pghn.2018.21.4.361
Abstract
- Accessory hepatic lobe is noted as and considered a rare disease in children. It can manifest with various symptoms and complications depending on the location, volume, type and position of the disease as presented on a child. The patient presented as a 14-month-old girl who was seen with a notable hepatosplenomegaly and portal hypertension. A diagnosis was made after taking an extensive medical history, observation and radiological examinations. The formal diagnosis was a prehepatic portal hypertension associated with accessory hepatic lobe.
Keyword
Figure
-
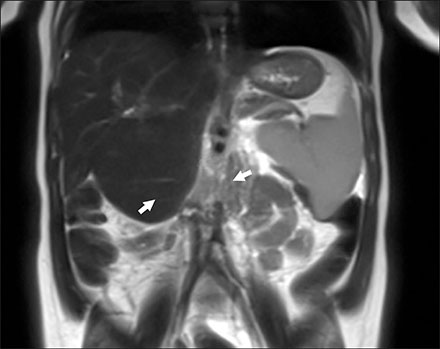
Fig. 1 T2-weighted coronal image demonstrates splenomegaly and 56×55 mm mass with same intensity as liver (accessory hepatic lobe, arrows) extending inferiorly from the segment 5–6 level, with separate portal and hepatic veins and compressing the right upper pole of the kidney.
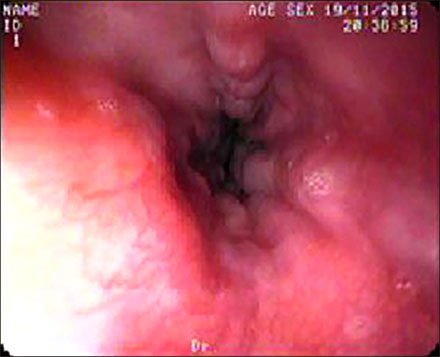
Fig. 2 Upper gastrointestinal endoscopy revealed three strands grade 2 esophageal varices without red spots.
Reference
-
1. Carrabetta S, Piombo A, Podestà R, Auriati L. Torsion and infarction of accessory liver lobe in young man. Surgery. 2009; 145:448–449.
Article2. Tancredi A, Cuttitta A, de Martino DG, Scaramuzzi R. Ectopic hepatic tissue misdiagnosed as a tumor of lung. Updates Surg. 2010; 62:121–123.
Article3. Mehta V, Arora J, Manik P, Suri RK, Rath G. Clinicoanatomical aspects of accessory fissures obscuring the normal hepatic morphology. Clin Ter. 2010; 161:259–260.4. Glenisson M, Salloum C, Lim C, Lacaze L, Malek A, Enriquez A, et al. Accessory liver lobes: anatomical description and clinical implications. J Visc Surg. 2014; 151:451–455.
Article5. Chavhan GB, Parra DA, Mann A, Navarro OM. Normal Doppler spectral waveforms of major pediatric vessels: specific patterns. Radiographics. 2008; 28:691–706.
Article6. Pujari BD, Deodhare SG. Symptomatic accessory lobe of liver with a review of the literature. Postgrad Med J. 1976; 52:234–236.
Article7. Garba ES, Ameh EA. Isolated rupture of an accessory liver from blunt abdominal trauma in childhood. Pediatr Surg Int. 2002; 18:62–63.
Article8. Akbulut S, Cakabay B, Sevinc MM, Basak F. Gastric outlet obstruction caused by Riedel's lobe of the liver: a diagnostic and therapeutic challenge for surgeons. Hepatogastroenterology. 2011; 58:589–592.9. Matley PJ, Rode H, Cywes S. Portal vein obstruction by ectopic liver tissue. J Pediatr Surg. 1989; 24:1163–1164.
Article10. Chandramohan A, Pachuau EL, Eapen A. Accessory hepatic lobe: a rare cause of extra-hepatic portal vein obstruction. Trop Gastroenterol. 2014; 35:190–193.
Article11. Wang C, Cheng L, Zhang Z, Xie T, Ding H, Deng Q, et al. Accessory lobes of the liver: A report of 3 cases and review of the literature. Intractable Rare Dis Res. 2012; 1:86–91.
Article
