Comparative Study between Sentinel Lymph Node Biopsy and Axillary Dissection in Patients with One or Two Lymph Node Metastases
- Affiliations
-
- 1Department of Surgery, Daejeon St. Mary's Hospital, The Catholic University of Korea College of Medicine, Daejeon, Korea. sun2729@naver.com
- 2Department of Surgery, Yeungnam University College of Medicine, Daegu, Korea.
- 3Department of Surgery, Inha University Hospital, Inha University College of Medicine, Incheon, Korea.
- 4Department of Surgery, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea.
- 5Department of Surgery, Korea Cancer Center Hospital, Korea Institute of Radiological & Medical Sciences, Seoul, Korea.
- 6Department of Surgery, Yonsei University College of Medicine, Seoul, Korea.
- 7Department of Surgery, Cheil General Hospital and Women's Healthcare Center, Dankook University College of Medicine, Seoul, Korea.
- KMID: 2421371
- DOI: http://doi.org/10.4048/jbc.2018.21.e44
Abstract
- PURPOSE
Sentinel lymph node biopsy (SLNB) is a standard axillary surgery in early breast cancer. If the SLNB result is positive, subsequent axillary lymph node dissection (ALND) is a routine procedure. In 2011, the American College of Surgeons Oncology Group Z0011 trial revealed that ALND may not be necessary in early breast cancer with one or two positive sentinel lymph nodes. The purpose of this study was to compare outcomes among Korean patients with one or two positive axillary lymph nodes in the final pathology who did and did not undergo ALND.
METHODS
A total of 131,717 patients from the Korea Breast Cancer Society registry database received breast cancer surgery from January 1995 to December 2014. Inclusion criteria were T stage 1 or 2, one or two positive lymph nodes, and having received breast-conserving surgery (BCS), whole breast radiation therapy, and no neoadjuvant therapy. We analyzed the differences in disease-specific survival (DSS) and overall survival (OS) between patients who received SLNB only and those who underwent SLNB+ALND.
RESULTS
A total 4,442 patients met the inclusion criteria, with 1,268 (28.6%) in the SLNB group and 3,174 (71.4%) in the SLNB+ALND group. There were no differences in DSS and OS between the two groups (p=0.378 and p=0.925, respectively). The number of patients who underwent SLNB alone for one or two positive lymph nodes increased continuously from 2004 to 2014.
CONCLUSION
Korean patients with early breast cancer and 1 or 2 positive axillary lymph nodes who received BCS plus SLNB showed no significant difference in DSS and OS regardless of whether they received ALND. The findings of this retrospective study demonstrate that omitting ALND can be considered when treating selected patients with early breast cancer who have one or two positive lymph nodes.
MeSH Terms
Figure
-

Figure 1 Selection and categorization of patients with one or two positive axillary lymph nodes in the study cohort.SLNB=sentinel lymph node biopsy; ALND=axillary lymph node dissection.

Figure 2 Survival outcomes by sentinel lymph node biopsy (SLNB) versus SLNB+axillary lymph node dissection (ALND) in early breast cancer. (A) Disease-specific survival. (B) Overall survival.
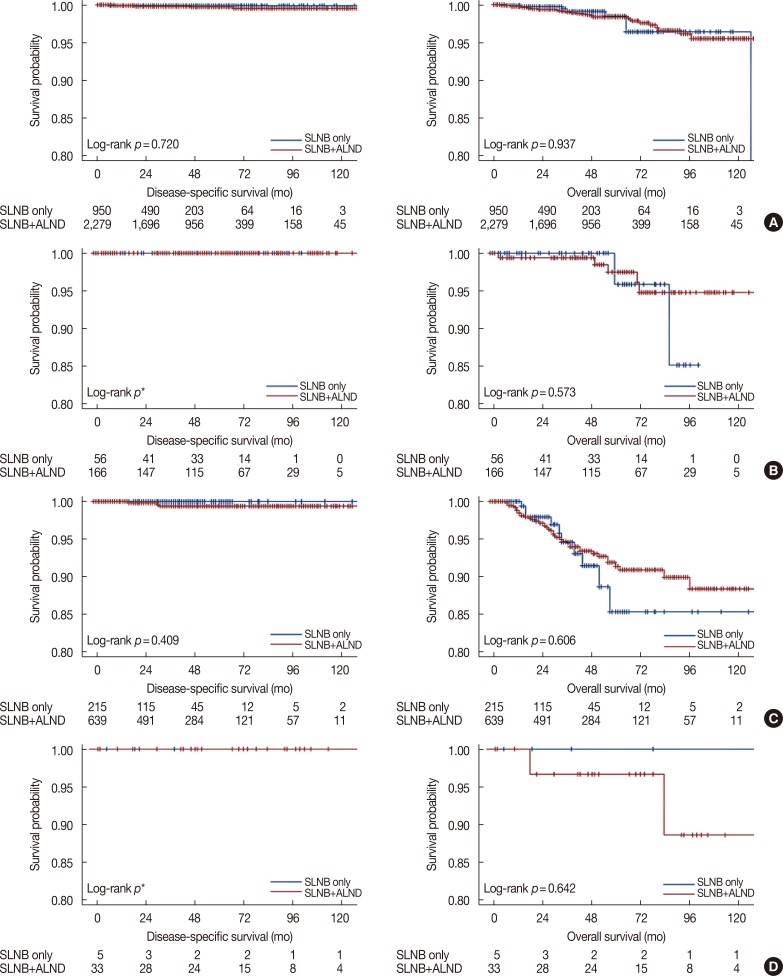
Figure 3 Disease-specific survival and overall survival according to molecular subtype. (A) Luminal A-like. (B) Luminal B-like. (C) Triple-negative. (D) HER2-enriched.SLNB=sentinel lymph node biopsy; ALND=axillary lymph node dissection; HER2=human epidermal growth factor receptor 2. *Luminal B-like and HER2-enriched type has no disease-related death.
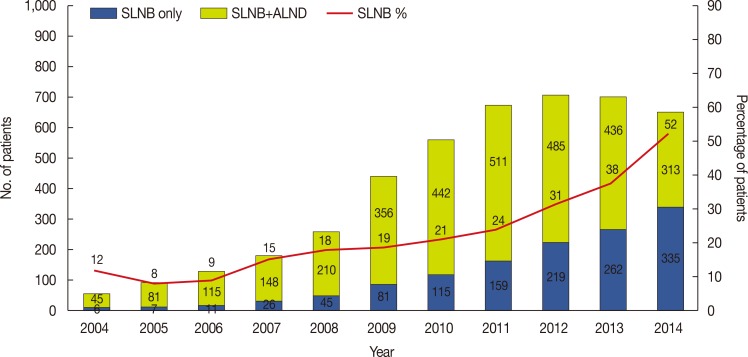
Figure 4 Annual incidence of sentinel lymph node biopsy (SLNB) versus SLNB+axillary lymph node dissection (ALND) in patients with one or two positive axillary lymph nodes.
Reference
-
1. Bergkvist L, de Boniface J, Jönsson PE, Ingvar C, Liljegren G, Frisell J, et al. Axillary recurrence rate after negative sentinel node biopsy in breast cancer: three-year follow-up of the Swedish Multicenter Cohort Study. Ann Surg. 2008; 247:150–156. PMID: 18156935.2. Giuliano AE, Haigh PI, Brennan MB, Hansen NM, Kelley MC, Ye W, et al. Prospective observational study of sentinel lymphadenectomy without further axillary dissection in patients with sentinel node-negative breast cancer. J Clin Oncol. 2000; 18:2553–2559. PMID: 10893286.
Article3. Veronesi U, Paganelli G, Viale G, Luini A, Zurrida S, Galimberti V, et al. A randomized comparison of sentinel-node biopsy with routine axillary dissection in breast cancer. N Engl J Med. 2003; 349:546–553. PMID: 12904519.
Article4. Ashikaga T, Krag DN, Land SR, Julian TB, Anderson SJ, Brown AM, et al. Morbidity results from the NSABP B-32 trial comparing sentinel lymph node dissection versus axillary dissection. J Surg Oncol. 2010; 102:111–118. PMID: 20648579.
Article5. Fant JS, Grant MD, Knox SM, Livingston SA, Ridl K, Jones RC, et al. Preliminary outcome analysis in patients with breast cancer and a positive sentinel lymph node who declined axillary dissection. Ann Surg Oncol. 2003; 10:126–130. PMID: 12620906.
Article6. Guenther JM, Hansen NM, DiFronzo LA, Giuliano AE, Collins JC, Grube BL, et al. Axillary dissection is not required for all patients with breast cancer and positive sentinel nodes. Arch Surg. 2003; 138:52–56. PMID: 12511150.
Article7. Jeruss JS, Winchester DJ, Sener SF, Brinkmann EM, Bilimoria MM, Barrera E Jr, et al. Axillary recurrence after sentinel node biopsy. Ann Surg Oncol. 2005; 12:34–40. PMID: 15827776.
Article8. Giuliano AE, McCall L, Beitsch P, Whitworth PW, Blumencranz P, Leitch AM, et al. Locoregional recurrence after sentinel lymph node dissection with or without axillary dissection in patients with sentinel lymph node metastases: the American College of Surgeons Oncology Group Z0011 randomized trial. Ann Surg. 2010; 252:426–432. PMID: 20739842.9. Giuliano AE, Ballman K, McCall L, Beitsch P, Whitworth PW, Blumencranz P, et al. Locoregional recurrence after sentinel lymph node dissection with or without axillary dissection in patients with sentinel lymph node metastases: long-term follow-up from the American College of Surgeons Oncology Group (Alliance) ACOSOG Z0011 randomized trial. Ann Surg. 2016; 264:413–420. PMID: 27513155.10. Giuliano AE, Ballman KV, McCall L, Beitsch PD, Brennan MB, Kelemen PR, et al. Effect of axillary dissection vs no axillary dissection on 10-year overall survival among women with invasive breast cancer and sentinel node metastasis: the ACOSOG Z0011 (Alliance) randomized clinical trial. JAMA. 2017; 318:918–926. PMID: 28898379.11. Miller CL, Specht MC, Skolny MN, Horick N, Jammallo LS, O'Toole J, et al. Risk of lymphedema after mastectomy: potential benefit of applying ACOSOG Z0011 protocol to mastectomy patients. Breast Cancer Res Treat. 2014; 144:71–77. PMID: 24500108.
Article12. Hong R, Dai Z, Zhu W, Xu B. Association between lymph node ratio and disease specific survival in breast cancer patients with one or two positive lymph nodes stratified by different local treatment modalities. PLoS One. 2015; 10:e0138908. PMID: 26513258.
Article13. Giuliano AE, Hunt KK, Ballman KV, Beitsch PD, Whitworth PW, Blumencranz PW, et al. Axillary dissection vs no axillary dissection in women with invasive breast cancer and sentinel node metastasis: a randomized clinical trial. JAMA. 2011; 305:569–575. PMID: 21304082.14. Le VH, Brant KN, Blackhurst DW, Schammel CM, Schammel DP, Cornett WR, et al. The impact of the American College of Surgeons Oncology Group (ACOSOG) Z0011 trial: an institutional review. Breast. 2016; 29:117–119. PMID: 27479042.
Article15. Gannan E, Khoo J, Nightingale S, Suhardja TS, Lippey J, Keane H, et al. Management of early node-positive breast cancer in Australia: a multicentre study. Breast J. 2016; 22:413–419. PMID: 27095381.
Article16. Joyce DP, Lowery AJ, McGrath-Soo LB, Downey E, Kelly L, O'Donoghue GT, et al. Management of the axilla: has Z0011 had an impact? Ir J Med Sci. 2016; 185:145–149. PMID: 25595827.
Article17. Loveland-Jones CE, Ruth K, Sigurdson ER, Egleston BL, Boraas M, Bleicher RJ. Patterns of nodal staging during breast conservation surgery in the medicare patient: will the ACOSOG Z0011 trial change the pattern of care? Breast Cancer Res Treat. 2014; 143:571–577. PMID: 24442687.
Article18. Tsao MW, Cornacchi SD, Hodgson N, Simunovic M, Thabane L, Cheng J, et al. A population-based study of the effects of a regional guideline for completion axillary lymph node dissection on axillary surgery in patients with breast cancer. Ann Surg Oncol. 2016; 23:3354–3364. PMID: 27342830.
Article19. Verheuvel NC, Voogd AC, Tjan-Heijnen VC, Roumen RM. Potential impact of application of Z0011 derived criteria to omit axillary lymph node dissection in node positive breast cancer patients. Eur J Surg Oncol. 2016; 42:1162–1168. PMID: 27265036.
Article20. Bonneau C, Hequet D, Estevez JP, Pouget N, Rouzier R. Impact of axillary dissection in women with invasive breast cancer who do not fit the Z0011 ACOSOG trial because of three or more metastatic sentinel lymph nodes. Eur J Surg Oncol. 2015; 41:998–1004. PMID: 25986854.
Article21. Clinical practice guidelines in oncology: breast, version 2012. National Comprehensive Cancer Network. 2012. Accessed March 26th. http://www.nccn.org.22. Roberts A, Nofech-Mozes S, Youngson B, McCready DR, Al-Assi M, Ramkumar S, et al. The importance of applying ACOSOG Z0011 criteria in the axillary management of invasive lobular carcinoma: a multiinstitutional cohort study. Ann Surg Oncol. 2015; 22:3397–3401. PMID: 26215196.
Article23. Edge SB. American Joint Committee on Cancer. American Cancer Society. American College of Surgeons. AJCC Cancer Staging Manual. 7th ed. New York: Springer;2010.24. Caudle AS, Hunt KK, Tucker SL, Hoffman K, Gainer SM, Lucci A, et al. American College of Surgeons Oncology Group (ACOSOG) Z0011: impact on surgeon practice patterns. Ann Surg Oncol. 2012; 19:3144–3151. PMID: 22847123.
Article25. Delpech Y, Bricou A, Lousquy R, Hudry D, Jankowski C, Willecocq C, et al. The exportability of the ACOSOG Z0011 criteria for omitting axillary lymph node dissection after positive sentinel lymph node biopsy findings: a multicenter study. Ann Surg Oncol. 2013; 20:2556–2561. PMID: 23456432.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Treatment of Malignant Melanoma Using Sentinel Lymph Node Dissection
- Ultrasonography for Staging Axillary Lymph Node in Breast Cancer Patients
- Sentinel Lymph Node Biopsy in the Oral Cavity Cancer
- The Number of Removed Lymph Nodes for an Acceptable False Negative Rate in Sentinel Lymph Node Biopsy for Breast Cancer
- Management of Malignant Melanoma Using Sentinel Lymph Node Biopsy: A Case Report
