Two Cases of Orbital Apex Syndrome after Blunt Orbital Trauma
- Affiliations
-
- 1Department of Ophthalmology, Pusan National University School of Medicine, Yangsan, Korea. lovcindy02@naver.com
- 2Biomedical Research Institute, Pusan National University Hospital, Busan, Korea.
- KMID: 2420341
- DOI: http://doi.org/10.3341/jkos.2018.59.9.893
Abstract
- PURPOSE
To report two cases of orbital apex syndrome caused by blunt orbital trauma without structural damage of the orbit.
CASE SUMMARY
(Case 1) A 50-year-old male came to our clinic complaining of visual loss after blunt orbital trauma by a metal bar. The best-corrected visual acuity was no light perception and light reflex was not observed in the affected eye. He also presented with complete ptosis and ophthalmoplegia with relative sparing of adduction and depression. High signal intensity of the orbital soft tissue including the optic nerve sheath was revealed using a T2-weighted image in magnetic resonance imaging. After starting steroid pulse therapy, his visual acuity improved to counting fingers on the third day. Ocular movement and levator function recovered to the normal range while visual acuity remained counting fingers. (Case 2) A 64-year-old female presented with complete ptosis after trauma to her right eyeball. The best-corrected visual acuity was 20/25 in the right eye. Complete ptosis and ophthalmoplegia with relative sparing of abduction and depression in the right eye were observed at the initial presentation. Magnetic resonance images showed enhancement of the right periphery optic nerve and distal rectus muscle. Two months after undergoing steroid pulse therapy, levator function and ocular movement recovered completely, and visual acuity improved to 20/20.
CONCLUSIONS
The orbital apex syndrome caused by blunt orbital trauma showed good response to steroid pulse therapy. Steroid treatments may therefore be considered for the treatment of traumatic orbital apex syndrome.
MeSH Terms
Figure
-

Figure 1. Nine diagnostic position of gaze field in case 1. Complete ptosis and ophthalmoplegia with partial sparing of adduction and depression in left eye was observed at initial presentation (A). At 5 months after treatment, ptosis and ophthalmoplegia were completely recovered (B).

Figure 2. Pattern visual evoked potential (VEP) of Case 1. Pattern VEP showed low amplitude in the affected left eye.
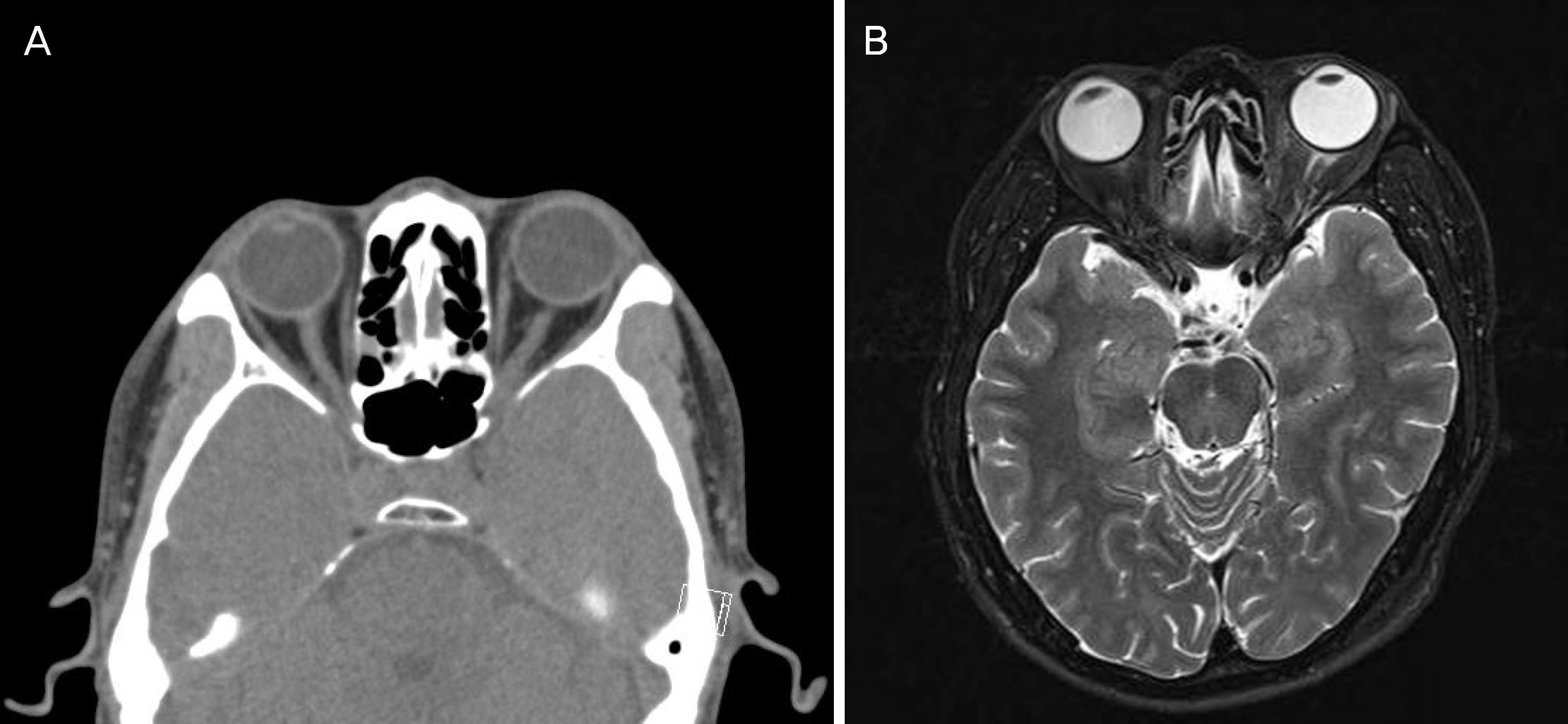
Figure 3. Computed tomography (CT) and magnetic resonance image (MRI) of the case 1 patient. Axial (A) CT scan showed no sign of orbital wall fracture and retrobulbar hemorrhage. Axial (B) T2-weighted image of magnetic resonance scan presented high signal intensity of the intraconal space including left optic nerve and soft tissue.
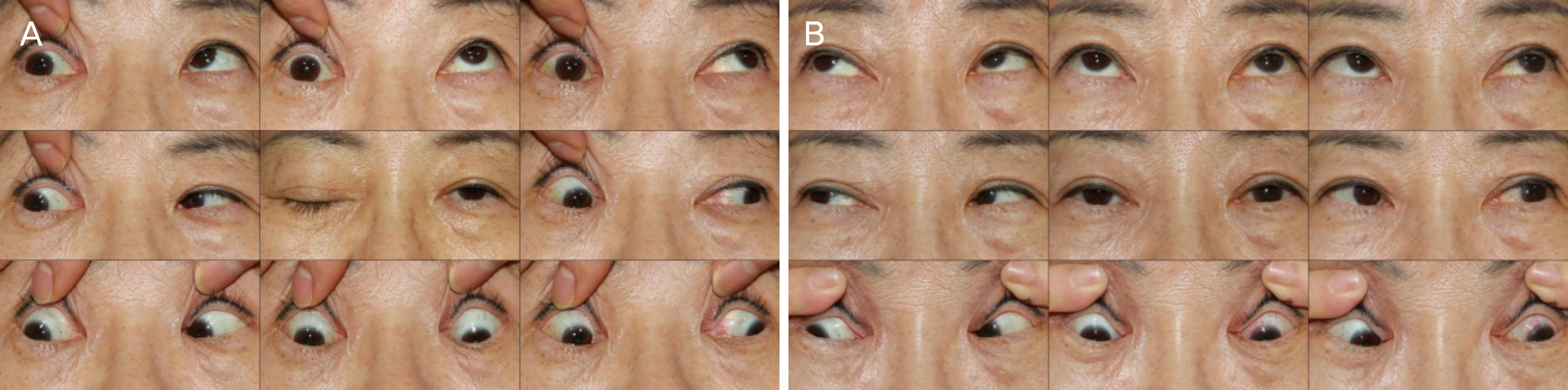
Figure 4. Nine diagnostic position of gaze field in case 2. Complete ptosis and ophthalmoplegia with partial sparing of abduction and depression in right eye was observed at initial presentation (A). Ptosis and ophthalmoplegia recovered completely at 2 months after treatment (B).
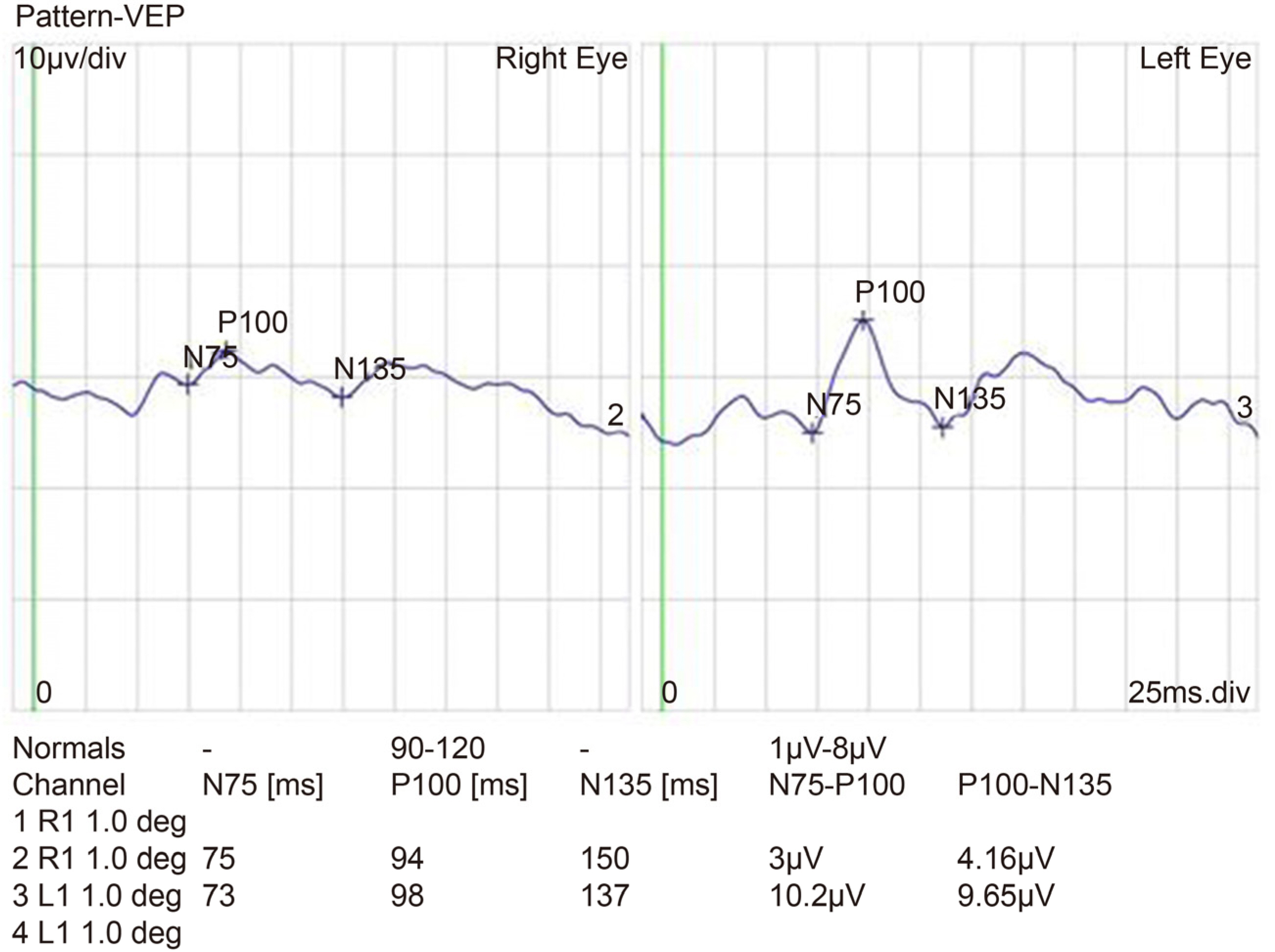
Figure 5. Pattern visual evoked potential (VEP) of Case 2. Pattern VEP showed reduction in the amplitude in the right eye.
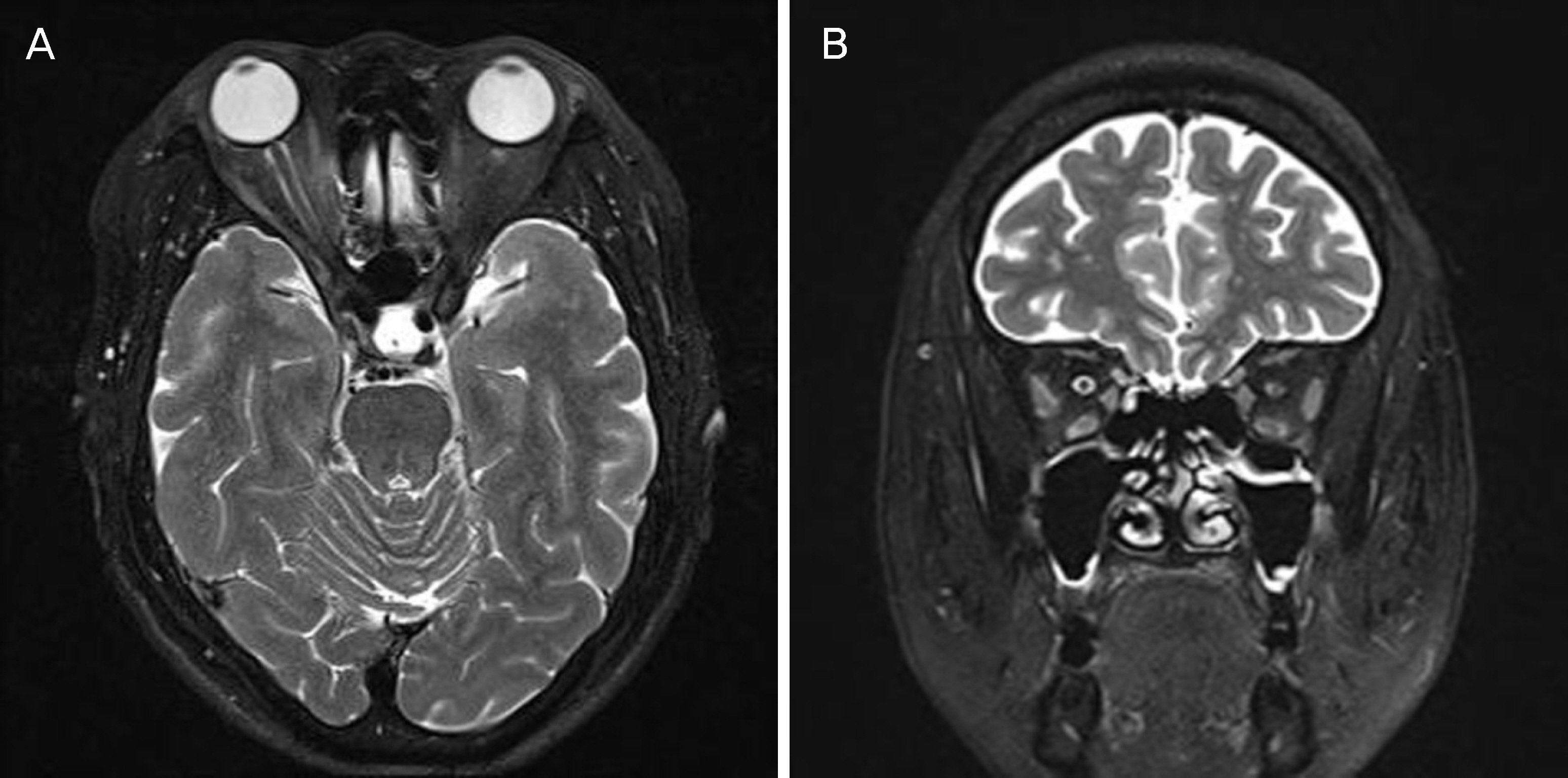
Figure 6. Axial (A) and coronal (B) magnetic resonance imaging (MRI) (T2-weighted image) scan at tenth day after injury. MRI showed enhancement of the right optic nerve sheath, distal rectus muscle and surrounding soft tissue.
Reference
-
References
1. Yeh S, Foroozan R. Orbital apex syndrome. Curr Opin Ophthalmol. 2004; 15:490–8.
Article2. Foroozan R, Bhatti MT, Rhoton AL. Transsphenoidal diplopia. Surv Ophthalmol. 2004; 49:349–58.
Article3. Kline LB. The Tolosa-Hunt syndrome. Surv Ophthalmol. 1982; 27:79–95.
Article4. Ing EB, Purvin V. Progressive visual loss and motility deficit. Surv Ophthalmol. 1997; 41:488–92.
Article5. Marcet MM, Yang W, Albert DM, et al. Aspergillus infection of the orbital apex masquerading as Tolosa-Hunt syndrome. Arch Ophthalmol. 2007; 125:563–6.
Article6. Keane JR. Cavernous sinus syndrome. Analysis of 151 cases. Arch Neurol. 1996; 53:967–71.
Article7. Lasky JB, Epley KD, Karesh JW. Household objects as a cause of self-inflicted orbital apex syndrome. J Trauma. 1997; 42:555–8.
Article8. Brent BD, May DR. Orbital apex syndrome after penetrating abdominal trauma. Ann Ophthalmol. 1990; 22:267–8.9. Peter NM, Pearson AR. Orbital apex syndrome from blunt ocular trauma. Orbit. 2010; 29:42–4.
Article10. Baik SH, Yeom DJ, Kang YK, et al. Orbital apex syndrome with nasal type natural killer (NK)/t-cell lymphoma of sphenoid and ethmoid sinus. J Korean Ophthalmol Soc. 2010; 51:286–91.11. Baek SU, Lee MJ. A case of orbital apex syndrome induced by abdominal orbital injury with long-term results. J Korean Ophthalmol Soc. 2013; 54:1275–81.12. Han K, Ahn M. A case of superior orbital fissure syndrome abdominal by penetrating orbital injury. J Korean Ophthalmol Soc. 2015; 56:592–7.13. Aryasit O, Preechawai P, Aui-Aree N. Clinical presentation, abdominal and prognosis of orbital apex syndrome. Orbit. 2013; 32:91–4.14. Zachariades N. The superior orbital fissure syndrome. Review of the literature and report of a case. Oral Surg Oral Med Oral Pathol. 1982; 53:237–40.15. Pogrel MA. The superior orbital fissure syndrome: report of case. J Oral Surg. 1980; 38:215–7.16. Imaizumi A, Ishida K, Ishikawa Y, Nakayoshi I. Successful abdominal of the traumatic orbital apex syndrome due to direct bone compression. Craniomaxillofac Trauma Reconstr. 2014; 7:318–22.17. Antonyshyn O, Gruss JS, Kassel EE. Blow-in fractures of the orbit. Plast Reconstr Surg. 1989; 84:10–20.
Article18. Acartürk S, Seküçoğ lu T, Kesiktäs E. Mega dose corticosteroid treatment for traumatic superior orbital fissure and orbital apex syndromes. Ann Plast Surg. 2004; 53:60–4.19. Hall ED, Braughler JM. Glucocorticoid mechanisms in acute abdominal cord injury: a review and therapeutic rationale. Surg Neurol. 1982; 18:320–7.20. Steinsapir KD, Goldberg RA. Traumatic optic neuropathy. Surv Ophthalmol. 1994; 38:487–518.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Orbital Apex Syndrome Caused by Paranasal Sinusitis
- A Case of Orbital Apex Syndrome Caused by Mucocele in the Sphenoid Sinus
- A Case of Idiopathic Orbital Myositis Involving All Extraocular Muscles of Both Eyes
- Analysis of Ocular Complications and Blowout Fracture in Orbital Blunt Trauma
- Orbital Apex Syndrome after Uneventful Phacoemulsification
