Prenatal diagnosis of isolated coronary arteriovenous fistula
- Affiliations
-
- 1Department of Obstetrics and Gynecology, University of Ulsan College of Medicine, Asan Medical Center, Seoul, Korea. poptwinkle@hanmail.net
- 2Division of Neonatology, Department of Pediatrics, University of Ulsan College of Medicine, Asan Medical Center, Seoul, Korea.
- 3Department of Diagnostic Imaging, University of Ulsan College of Medicine, Asan Medical Center, Seoul, Korea.
- 4Department of Pediatric Cardiology, University of Ulsan College of Medicine, Asan Medical Center, Seoul, Korea.
- 5Division of Pediatric Cardiac Surgery, University of Ulsan College of Medicine, Asan Medical Center, Seoul, Korea.
- KMID: 2420166
- DOI: http://doi.org/10.5468/ogs.2018.61.1.161
Abstract
- Coronary arteriovenous fistula (CAVF) is a rare condition defined as an anomalous termination of the coronary arteries. The etiology of CAVF is either congenital or acquired, and iatrogenic CAVF is most commonly caused by cardiovascular surgery or percutaneous intervention. Most of the prenatally diagnosed CAVFs were related to complex heart disease, and only few cases of an isolated CAVF have been reported to date. We successfully diagnosed an isolated CAVF by fetal echocardiography at 25.3 weeks of gestation. Accurate prenatal diagnosis resulted in the prompt decision for postnatal surgical correction, and the neonate thrived well without any complications.
MeSH Terms
Figure
-
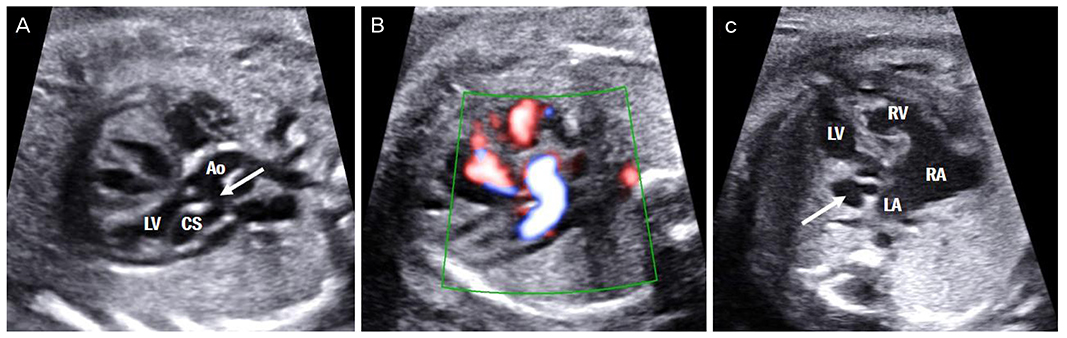
Fig. 1 The 5-chamber view of the heart at 25.3 weeks showing the fistula between the left coronary artery and coronary sinus (arrow, A). Power Doppler imaging confirming the communication between the left coronary artery and coronary sinus (B). The 4-chamber view of the heart at 29.6 weeks showing the dilated coronary sinus (arrow) with the collapsed left atrium (C). Ao, aorta; CS, coronary sinus; LA, left atrium; LV, left ventricle; RA, right atrium; RV, right ventricle.

Fig. 2 Postnatal computed tomography showing the dilated left circumflex artery draining into the enlarged coronary sinus on the axial image (arrow, A) and the 3-dimensional volume rendering image (arrow, B). Ao, aorta; CS, coronary sinus; LAA, left atrial appendage; LCX, left circumflex coronary artery; LMA, left main coronary artery; PA, pulmonary artery.
Reference
-
1. Schumacher G, Roithmaier A, Lorenz HP, Meisner H, Sauer U, Müller KD, et al. Congenital coronary artery fistula in infancy and childhood: diagnostic and therapeutic aspects. Thorac Cardiovasc Surg. 1997; 45:287–294.
Article2. Chaoui R, Tennstedt C, Göldner B, Bollmann R. Prenatal diagnosis of ventriculo-coronary communications in a second-trimester fetus using transvaginal and transabdominal color Doppler sonography. Ultrasound Obstet Gynecol. 1997; 9:194–197.
Article3. Chaoui R, Tennstedt C, Göldner B. Prenatal diagnosis of ventriculocoronary arterial fistula in a fetus with hypoplastic left heart syndrome and aortic atresia. Ultrasound Obstet Gynecol. 2002; 20:75–78.
Article4. Nagiub M, Mahadin D, Gowda S, Aggarwal S. Prenatal diagnosis of coronary artery fistula: a case report and review of literature. AJP Rep. 2014; 4:e83–e86.
Article5. Hayashi G, Inamura N, Kayatani F, Kawazu Y, Hamamichi Y, Hisaaki A. Prenatal diagnosis of a left coronary artery to left atrial fistula. Prenat Diagn. 2012; 32:194–196.
Article6. Matsumoto Y, Hoashi T, Kagisaki K, Ichikawa H. Successful surgical treatment of a gigantic congenital coronary artery fistula immediately after birth. Interact Cardiovasc Thorac Surg. 2012; 15:520–522.
Article7. Cetiner N, Altunyuva Usta S, Akalın F. Coronary arteriovenous fistula causing hydrops fetalis. Case Rep Obstet Gynecol. 2014; 2014:487281.8. Oztunc F, Gokalp S, Yuksel MA, Imamoglu M, Madazli R. Prenatal diagnosis of left coronary artery to right ventricle fistula. J Clin Ultrasound. 2015; 43:129–131.
Article9. Sharland GK, Konta L, Qureshi SA. Prenatal diagnosis of isolated coronary artery fistulas: progression and outcome in five cases. Cardiol Young. 2016; 26:915–920.
Article10. Zeng S, Zhou Q, Tian L, Zhou J, Zhang M, Cao D. Isolated coronary artery fistula in fetal heart: case reports and literature review. Fetal Pediatr Pathol. 2016; 35:348–352.
Article11. Kaldararova M, Tittel P, Zahorec M. Giant coronary artery fistula: prenatal diagnosis, newborn manifestation. Rev Esp Cardiol (Engl Ed). 2016; 69:1100.
Article12. Challoumas D, Pericleous A, Dimitrakaki IA, Danelatos C, Dimitrakakis G. Coronary arteriovenous fistulae: a review. Int J Angiol. 2014; 23:1–10.
Article13. Said SA, Lam J, van der Werf T. Solitary coronary artery fistulas: a congenital anomaly in children and adults. A contemporary review. Congenit Heart Dis. 2006; 1:63–76.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Unusual Three Cases of Adult Coronary Arteriovenous Fistula
- A Case Report of Coronary Arteriovenous Fistula
- Five Cases of Coronary Arteriovenous Fistula from Coronary Artery to Left Ventricle
- Congenital Coronary Arteriovenous Fistula in Adult
- A Case of Giant Aneurysm of Coronary Arteriovenous Fistula Treated by Percutaneous Deployment of Embolization Coil
