Opening Wedge High Tibia Osteotomy
- Affiliations
-
- 1Department of Orthopedic Surgery, Inje University Ilsan Paik Hospital, Goyang, Korea.
- 2Department of Orthopedic Surgery, Daegu Fatima Hospital, Daegu, Korea. hjh8434@daum.net
- KMID: 2419464
- DOI: http://doi.org/10.4055/jkoa.2018.53.4.293
Abstract
- Proximal tibial osteotomy is the preferred method for treating medial compartment knee arthritis with varus deformity. The purpose of this treatment is to reduce the weight burden of the lesion by correcting the mechanical axis of the patient with degenerative arthritis of medial tibiofemoral joint and abnormal alignment. In general, the proximal tibial osteotomy provides satisfactory clinical results when suitable patient are selected by considering the extent of cartilaginous injury and the age of the patient and the correct technique is performed. In tibial osteotomy, medial open wedge osteotomy is used widely because of its short operation time and relatively simple technique. This review describes the current knowledge of patient selection, preoperative evaluation and planning, treatment principles, surgical techniques, rehabilitation procedures and complications in open wedge high tibial osteotomy.
MeSH Terms
Figure
-

Figure 1 Intraoperative C-arm method. Check whether the mechanical axis is located at 62% to 65% of the outer side of the articular surface using iron or steel tape.

Figure 2 Bilateral weight bearing anteroposterior whole lower limb X-ray. (A) Miniaci method. A new mechanical axis Line 1 passing through the desired position is drawn and the angle formed by line 2 and 3 passing through the hinge section (X) is defined as the correcting angle. (B) Dugdale method. Line 1 is drawn formo the center of the femoral head to the 62.5% of the tibial width. Line 2 is drawn from the center of the talus to the 62.5%. The angle formed by line 1 and 2 is the correcting angle.
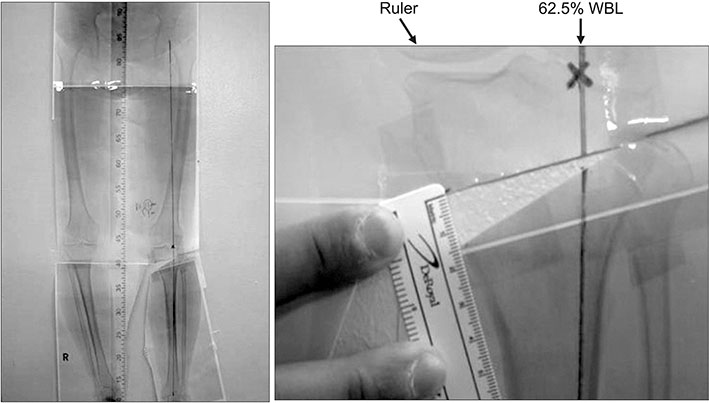
Figure 3 Weight-bearing scanography measure method: a template was cut through the osteotomy site and the tibia was rotated until the weight bearing line (WBL) through the 62.5% coordinate.
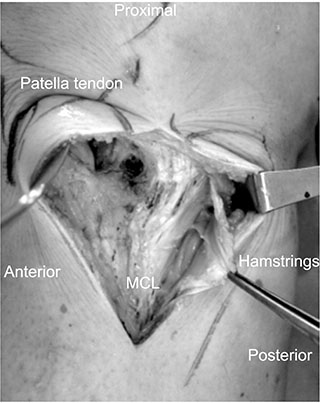
Figure 4 Pes anserinus was detached from the attachment and then pulled inward. The metaphyseal flare could be identified. MCL, medial collateral ligament.

Figure 5 Anteroposterior fluoroscopy view of the knee showing the safe zone. A, tip of the fibular head; B, circumference line of the fibular head.

Figure 6 An osteotomy should be performed until only 5 to 10 mm of the lateral cortex is left.
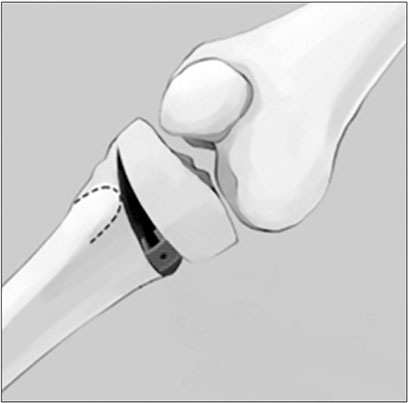
Figure 7 Space can be maintained by inserting the metal block into the osteotomy surface.

Figure 8 (A) Second osteotomy was performed with a 100°–110° tilt to the first osteotomy site. (B) The 3 or 4 chisel technique is used to open the site of osteotomy.

Figure 9 During uniplanar osteotomy, a metal block is fixed to the plate using screw.
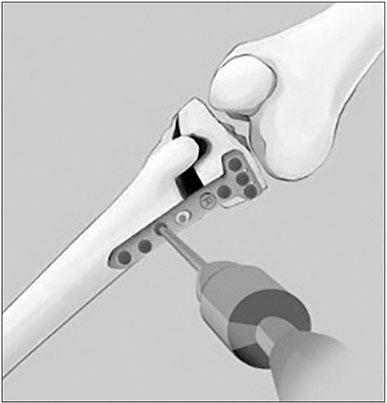
Figure 10 After screw fixation of the proximal part, hyperextension and internal rotation of knee, fix the distal part.
Reference
-
1. Hernigou P, Medevielle D, Debeyre J, Goutallier D. Proximal tibial osteotomy for osteoarthritis with varus deformity. A ten to thirteen-year follow-up study. J Bone Joint Surg Am. 1987; 69:332–354.2. Insall JN, Joseph DM, Msika C. High tibial osteotomy for varus gonarthrosis. A long-term follow-up study. J Bone Joint Surg Am. 1984; 66:1040–1048.
Article3. Fujisawa Y, Masuhara K, Shiomi S. The effect of high tibial osteotomy on osteoarthritis of the knee. An arthroscopic study of 54 knee joints. Orthop Clin North Am. 1979; 10:585–608.4. Mina C, Garrett WE Jr, Pietrobon R, Glisson R, Higgins L. High tibial osteotomy for unloading osteochondral defects in the medial compartment of the knee. Am J Sports Med. 2008; 36:949–955.
Article5. Lee DH, Han SB, Oh KJ, et al. The weight-bearing scanogram technique provides better coronal limb alignment than the navigation technique in open high tibial osteotomy. Knee. 2014; 21:451–455.
Article6. Chae DJ, Shetty GM, Lee DB, Choi HW, Han SB, Nha KW. Tibial slope and patellar height after opening wedge high tibia osteotomy using autologous tricortical iliac bone graft. Knee. 2008; 15:128–133.
Article7. Rossi R, Bonasia DE, Amendola A. The role of high tibial osteotomy in the varus knee. J Am Acad Orthop Surg. 2011; 19:590–599.
Article8. Nha KW, Lee YS, Hwang DH, et al. Second-look arthroscopic findings after open-wedge high tibia osteotomy focusing on the posterior root tears of the medial meniscus. Arthroscopy. 2013; 29:226–231.
Article9. Aglietti P, Rinonapoli E, Stringa G, Taviani A. Tibial osteotomy for the varus osteoarthritic knee. Clin Orthop Relat Res. 1983; 176:239–251.
Article10. Naudie D, Bourne RB, Rorabeck CH, Bourne TJ. The Install Award. Survivorship of the high tibial valgus osteotomy. A 10- to -22-year followup study. Clin Orthop Relat Res. 1999; 367:18–27.11. Rudan JF, Simurda MA. High tibial osteotomy. A prospective clinical and roentgenographic review. Clin Orthop Relat Res. 1990; 255:251–256.12. Dugdale TW, Noyes FR, Styer D. Preoperative planning for high tibial osteotomy. The effect of lateral tibiofemoral separation and tibiofemoral length. Clin Orthop Relat Res. 1992; 274:248–264.13. Phillips CL, Silver DA, Schranz PJ, Mandalia V. The measurement of patellar height: a review of the methods of imaging. J Bone Joint Surg Br. 2010; 92:1045–1053.14. Lee DH, Nha KW, Park SJ, Han SB. Preoperative and postoperative comparisons of navigation and radiologic limb alignment measurements after high tibial osteotomy. Arthroscopy. 2012; 28:1842–1850.
Article15. Miniaci A, Ballmer FT, Ballmer PM, Jakob RP. Proximal tibial osteotomy. A new fixation device. Clin Orthop Relat Res. 1989; 246:250–259.16. Staubli AE, De Simoni C, Babst R, Lobenhoffer P. TomoFix: a new LCP-concept for open wedge osteotomy of the medial proximal tibia: early results in 92 cases. Injury. 2003; 34:Suppl 2. B55–B62.17. Han SB, Lee DH, Shetty GM, Chae DJ, Song JG, Nha KW. A “safe zone” in medial open-wedge high tibia osteotomy to prevent lateral cortex fracture. Knee Surg Sports Traumatol Arthrosc. 2013; 21:90–95.
Article18. Takeuchi R, Ishikawa H, Kumagai K, et al. Fractures around the lateral cortical hinge after a medial opening-wedge high tibial osteotomy: a new classification of lateral hinge fracture. Arthroscopy. 2012; 28:85–94.
Article19. Sabzevari S, Ebrahimpour A, Roudi MK, Kachooei AR. High tibial osteotomy: a systematic review and current concept. Arch Bone Jt Surg. 2016; 4:204–212.20. Han JH, Kim HJ, Song JG, et al. Is bone grafting necessary in opening wedge high tibial osteotomy? A meta-analysis of radiological outcomes. Knee Surg Relat Res. 2015; 27:207–220.
Article21. Spahn G. Complications in high tibial (medial opening wedge) osteotomy. Arch Orthop Trauma Surg. 2004; 124:649–653.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Comparison of High Tibial Osteotomy: Opening versus Closing Wedge Osteotomy
- Basic Principles and Current Trends of Medial Opening-Wedge High Tibial Osteotomy
- Distal Femoral Medial Opening Wedge Osteotomy for Post-Traumatic, Distal Femoral Varus Deformity
- Delayed Onset of the Popliteal Artery Pseudoaneurysm Following Medial Opening Wedge High Tibial Osteotomy
- Factors Affecting the Results of Proximal Tibia Opening Wedge Osteotomy
