Korean J Ophthalmol.
2018 Aug;32(4):319-327. 10.3341/kjo.2017.0086.
Characteristics of Patients Who Are Not Responsive to Alternate Patching for Overcorrected Intermittent Exotropia
- Affiliations
-
- 1Department of Ophthalmology, Haeundae Paik Hospital, Inje University College of Medicine, Busan, Korea. kris9352@hanmail.net
- KMID: 2418153
- DOI: http://doi.org/10.3341/kjo.2017.0086
Abstract
- PURPOSE
To compare the characteristics of patients with surgically overcorrected intermittent exotropia treated with alternate patching.
METHODS
The medical records of 51 patients who underwent bilateral lateral rectus muscle recession for intermittent exotropia and required alternate patching to correct postoperative overcorrection were retrospectively reviewed. Patients with postoperative esodeviation ≥18 prism diopters (PD) were started on alternate patching on postoperative day 1, whereas those with postoperative esodeviation of 10 to 17 PD were started after 2 weeks. Postoperative esodeviation <10 PD was considered as slight intentional overcorrection after exotropia surgery. Patients not responsive to alternate patching treatment were defined as those with postoperative esodeviation ≥10 PD after 3 months of treatment. Sex, family history, age, refractive error, amblyopia, stereopsis, suppression, type of exotropia, surgical method, preoperative and postoperative angle of deviation, and start time of alternate patching were compared.
RESULTS
Among 51 patients, 29 patients responded to alternate patching and 22 patients did not respond. Female sex (p = 0.04), larger preoperative exodeviation at distance (p = 0.04), late onset of postoperative maximal esodeviation (p < 0.01), larger postoperative maximal esodeviation at near (p = 0.02), and late initiation of alternate patching (p = 0.01) were associated with patients in the non-responsive group. Although postoperative angle of deviation was similar for 2 weeks, the angle of postoperative esodeviation was significantly larger in the non-responsive group than in the responsive group, beginning at 1 month postoperatively.
CONCLUSIONS
Female sex, large preoperative exodeviation, late initiation of alternate patching, and large esodeviation 1-month postoperative predisposed patients to be resistant to alternate patching for postoperative overcorrection.
MeSH Terms
Figure
-
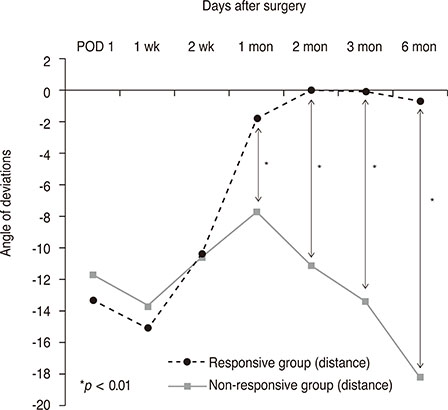
Fig. 1 Postoperative changes in the mean angle of deviation at distance in patients responsive and nonresponsive to alternate patching treatment. There were significant differences between the two groups, with esodeviation nearly recovering in the responsive group after 1 month. (−) means esodeviation and (+) means exodeviation. POD = postoperative day.
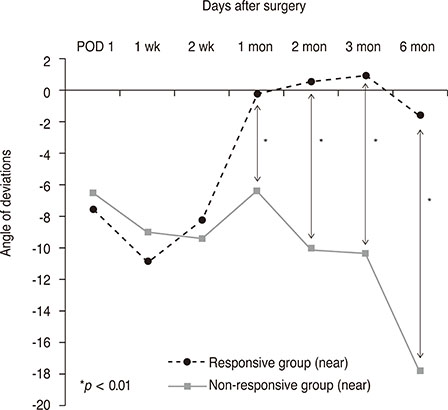
Fig. 2 Postoperative changes in the mean angle of deviation at near in patients responsive and nonresponsive to alternate patching treatment. There were significant differences between the two groups after 1 month. (−) means esodeviation and (+) means exodeviation. POD = postoperative day.
Reference
-
1. Park H, Kim WJ, Kim MM. The stabilization of postoperative exo-drift in intermittent exotropia after surgical treatment. Korean J Ophthalmol. 2016; 30:60–65.
Article2. Yang M, Chen J, Shen T, et al. Clinical characteristics and surgical outcomes in patients with intermittent exotropia: a large sample study in south China. Medicine (Baltimore). 2016; 95:e2590.3. Campos E. Surgical correction and outcome of exotropia. Asia Pac J Ophthalmol (Phila). 2015; 4:185–186.
Article4. Chang YH, Melvin P, Dagi LR. Goal-determined metrics to assess outcomes of exotropia surgery. J AAPOS. 2015; 19:304–310.5. Clarke WN, Noel LP. Surgical results in intermittent exotropia. Can J Ophthalmol. 1981; 16:66–69.6. Hardesty HH. Prisms in the management of intermittent exotropia. Am Orthopt J. 1972; 22:22–30.
Article7. Kim HJ, Choi DG. Consecutive esotropia after surgery for intermittent exotropia: the clinical course and factors associated with the onset. Br J Ophthalmol. 2014; 98:871–875.
Article8. Raab EL, Parks MM. Recession of the lateral recti: early and late postoperative alignments. Arch Ophthalmol. 1969; 82:203–208.9. Choi YM, Lee JY, Jung JH, et al. Risk factors predicting the need for additional surgery in consecutive esotropia. J Pediatr Ophthalmol Strabismus. 2013; 50:335–339.
Article10. von Noorden GK. Binocular vision and ocular motility. St. Louis: CV Mosby;1994. p. 438–442.11. Hardesty HH. Treatment of overcorrected intermittent exotropia. Am J Ophthalmol. 1968; 66:80–86.
Article12. Park KH, Kim SY. Clinical characteristics of patients that experience different rates of exodrift after strabismus surgery for intermittent exotropia and the effect of the rate of exodrift on final ocular alignment. J AAPOS. 2013; 17:54–58.13. Wagner RS. Consecutive esotropia following surgery for intermittent exotropia. J Pediatr Ophthalmol Strabismus. 2013; 50:334.
Article14. Souza-Dias C. Postoperative evolution of the planned initial overcorrection in intermittent exotropia: 61 cases. Binocul Vis Eye Muscle Surg Q. 1993; 8:141–148.15. Kim DW, Han S, Kim US, Baek SH. Results of conservative management for consecutive esotropia after intermittent exotropia surgery. Eye (Lond). 2015; 29:776–782.
Article16. Pineles SL, Ela-Dalman N, Zvansky AG, et al. Long-term results of the surgical management of intermittent exotropia. J AAPOS. 2010; 14:298–304.
Article17. Kim YH, Choi MY. The effect of fresnel prism treatment in consecutive esotropia. J Korean Ophthalmol Soc. 2006; 47:1623–1629.18. Lee EK, Hwang JM. Prismatic correction of consecutive esotropia in children after a unilateral recession and resection procedure. Ophthalmology. 2013; 120:504–511.
Article19. Lee EK, Yang HK, Hwang JM. Long-term outcome of prismatic correction in children with consecutive esotropia after bilateral lateral rectus recession. Br J Ophthalmol. 2015; 99:342–345.
Article20. Dawson EL, Marshman WE, Lee JP. Role of botulinum toxin A in surgically overcorrected exotropia. J AAPOS. 1999; 3:269–271.
Article21. von Noorden GK, Campos EC. Principles of nonsurgical treatment. 5th ed. St. Louis: Mosby-Year Book;1996. p. 503.22. Na KI, Lee JY. Consecutive esotropia after lateral rectus muscle recession for intermittent exotropia. J Korean Ophthalmol Soc. 2012; 53:1318–1323.
Article23. Jang JH, Park JM, Lee SJ. Factors predisposing to consecutive esotropia after surgery to correct intermittent exotropia. Graefes Arch Clin Exp Ophthalmol. 2012; 250:1485–1490.
Article24. Buck D, Powell CJ, Sloper JJ, et al. Surgical intervention in childhood intermittent exotropia: current practice and clinical outcomes from an observational cohort study. Br J Ophthalmol. 2012; 96:1291–1295.
Article25. Buck D, Powell C, Sloper J, et al. Authors' response: after intermittent exotropia surgery, consecutive esotropia: good or bad? by K K Shoaib. Br J Ophthalmol. 2013; 97:797–798.
Article26. Choi J, Kim SJ, Yu YS. Initial postoperative deviation as a predictor of long-term outcome after surgery for intermittent exotropia. J AAPOS. 2011; 15:224–229.
Article27. Woo KJ, Choi MY. Clinical course of patients with delayed consecutive esotropia after exotropia surgery. J Korean Ophthalmol Soc. 2008; 49:1812–1818.
Article28. Han DH, Paik HJ. The minimal postoperative follow-up period to determine secondary surgery in patients with intermittent exotropia. J Korean Ophthalmol Soc. 2014; 55:711–718.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Clinical Findings of Constant Exotropia Developed from Intermittent Exotropia
- The Influence of Part-time Patching Therapy on Types of Intermittent Exotropia
- Can we effectively delay surgery for intermittent exotropia in children less than 4 years of age?
- Surgical Results of Intermittent Exotropia in Pediatric versus Adult Group
- Is The Nonsurgical Treatment Effective on Intermittent Exotropia in Children of School-Age?
