Cancer Res Treat.
2018 Jul;50(3):1039-1050. 10.4143/crt.2017.252.
The Impact of Surgical Timing on Pathologic Tumor Response after Short Course and Long Course Preoperative Chemoradiation for Locally Advanced Rectal Adenocarcinoma
- Affiliations
-
- 1Department of Radiation Oncology, Seoul St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea. hsjang11@catholic.ac.kr
- 2Department of Radiation Oncology, St. Vincent’s Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea.
- 3Department of Colorectal Surgery, Seoul St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea.
- 4Center for Colorectal Cancer, Research Institute and Hospital, National Cancer Center, Goyang, Korea.
- 5Department of Radiation Oncology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- 6Department of Surgery, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- 7Department of Radiation Oncology, Seoul National University College of Medicine, Seoul, Korea.
- 8Department of Radiation Oncology, Chonnam National University Medical School, Gwangju, Korea.
- KMID: 2417891
- DOI: http://doi.org/10.4143/crt.2017.252
Abstract
- PURPOSE
A pooled analysis of multi-institutional trials was performed to analyze the effect of surgical timing on tumor response by comparing short course concurrent chemoradiotherapy (CCRT) with long course CCRT followed by delayed surgery in locally advanced rectal cancer.
MATERIALS AND METHODS
Three hundred patients with cT3-4N0-2 rectal adenocarcinoma were included. Long course patients from KROG 14-12 (n=150) were matched 1:1 to 150 short course patients from KROG 10-01 (NCT01129700) and KROG 11-02 (NCT01431599) according to stage, age, and other risk factors. The primary endpoint was to determine the interval between surgery and the last day of neoadjuvant CCRT which yields the best tumor response after the short course and long course CCRT. Downstaging was defined as ypT0-2N0M0 and pathologic complete response (ypCR) was defined as ypT0N0M0, respectively.
RESULTS
Both the long and short course groups achieved lowest downstaging rates at < 6 weeks (long 20% vs. short 8%) and highest downstaging rates at 6-7 weeks (long 44% vs. short 40%). The ypCR rates were lowest at < 6 weeks (both long and short 0%) and highest at 6-7 weeks (long 21% vs. short 11%) in both the short and long course arms. The downstaging and ypCR rates of long course group gradually declined after the peak at 6-7 weeks and those of the short course group trend to constantly increase afterwards.
CONCLUSION
It is optimal to perform surgery at least 6 weeks after both the short course and long course CCRT to obtain maximal tumor regression in locally advanced rectal adenocarcinoma.
Figure
-
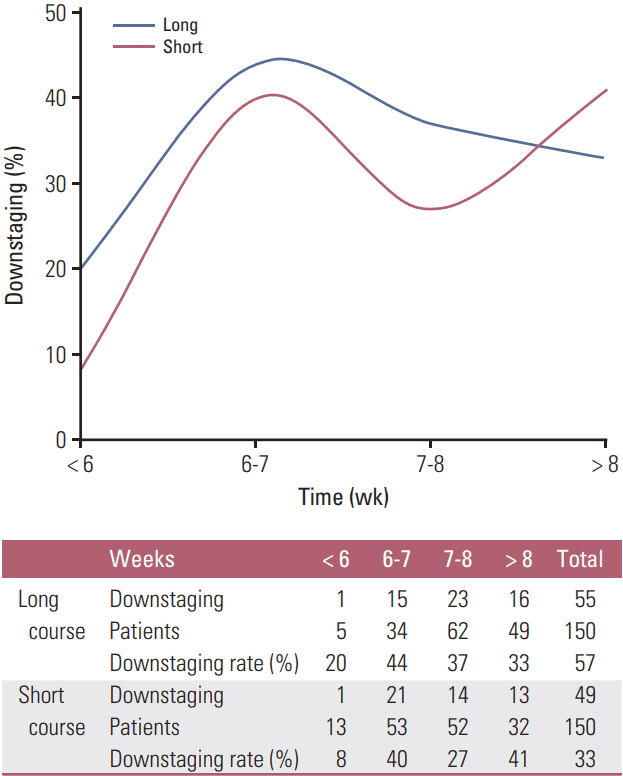
Fig. 1. Distribution of downstaging rates by weeks since completion of radiotherapy to surgery in short course and long course patients.
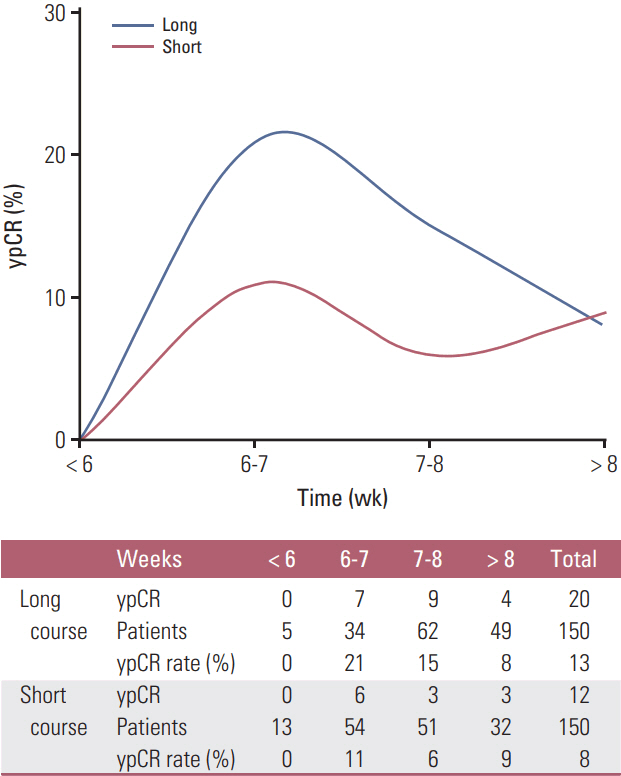
Fig. 2. Distribution of pathologic complete response (ypCR) rates by weeks since completion of radiotherapy to surgery in short course and long course patients.
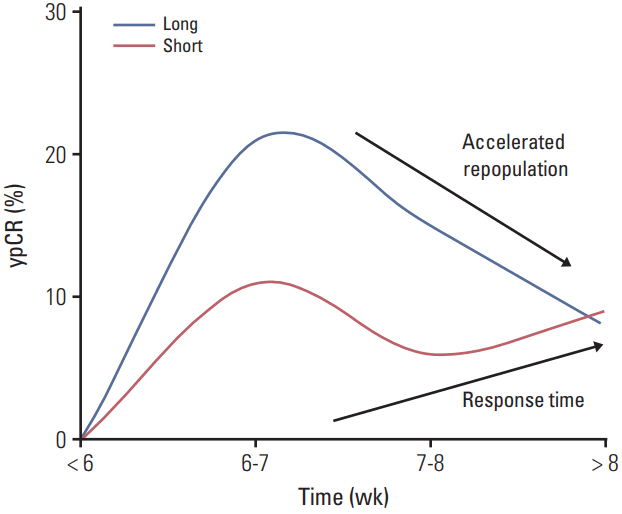
Fig. 3. A hypothesis of radiobiology behind the difference in distribution of pathologic complete response (ypCR) rates by weeks since completion of radiotherapy to surgery in short course and long course chemoradiation.
Reference
-
References
1. Oh CM, Won YJ, Jung KW, Kong HJ, Cho H, Lee JK, et al. Cancer statistics in Korea: incidence, mortality, survival, and prevalence in 2013. Cancer Res Treat. 2016; 48:436–50.
Article2. Lee HS, Choi DH, Park HC, Park W, Yu JI, Chung K. Correlation between tumor regression grade and rectal volume in neoadjuvant concurrent chemoradiotherapy for rectal cancer. Radiat Oncol J. 2016; 34:186–92.
Article3. Yeo SG, Oh JH, Kim DY, Baek JY, Kim SY, Park JW, et al. Preoperative short-course concurrent chemoradiation therapy followed by delayed surgery for locally advanced rectal cancer: a phase 2 multicenter study (KROG 10-01). Int J Radiat Oncol Biol Phys. 2013; 86:34–9.
Article4. Lee JH, Kim JG, Oh ST, Lee MA, Chun HG, Kim DY, et al. Two-week course of preoperative chemoradiotherapy followed by delayed surgery for rectal cancer: a phase II multiinstitutional clinical trial (KROG 11-02). Radiother Oncol. 2014; 110:150–4.
Article5. Stein DE, Mahmoud NN, Anne PR, Rose DG, Isenberg GA, Goldstein SD, et al. Longer time interval between completion of neoadjuvant chemoradiation and surgical resection does not improve downstaging of rectal carcinoma. Dis Colon Rectum. 2003; 46:448–53.
Article6. Tulchinsky H, Shmueli E, Figer A, Klausner JM, Rabau M. An interval > 7 weeks between neoadjuvant therapy and surgery improves pathologic complete response and disease-free survival in patients with locally advanced rectal cancer. Ann Surg Oncol. 2008; 15:2661–7.7. Habr-Gama A, Perez RO, Proscurshim I, Nunes Dos Santos RM, Kiss D, Gama-Rodrigues J, et al. Interval between surgery and neoadjuvant chemoradiation therapy for distal rectal cancer: does delayed surgery have an impact on outcome? Int J Radiat Oncol Biol Phys. 2008; 71:1181–8.
Article8. Coucke PA, Notter M, Matter M, Fasolini F, Calmes JM, Schlumpf R, et al. Effect of timing of surgery on survival after preoperative hyperfractionated accelerated radiotherapy (HART) for locally advanced rectal cancer (LARC): is it a matter of days? Acta Oncol. 2006; 45:1086–93.
Article9. Lefevre JH, Mineur L, Kotti S, Rullier E, Rouanet P, de Chaisemartin C, et al. Effect of interval (7 or 11 weeks) between neoadjuvant radiochemotherapy and surgery on complete pathologic response in rectal cancer: a multicenter, randomized, controlled trial (GRECCAR-6). J Clin Oncol. 2016; 34:3773–80.
Article10. Lim SB, Choi HS, Jeong SY, Kim DY, Jung KH, Hong YS, et al. Optimal surgery time after preoperative chemoradiotherapy for locally advanced rectal cancers. Ann Surg. 2008; 248:243–51.
Article11. van den Broek CB, Vermeer TA, Bastiaannet E, Rutten HJ, van de Velde CJ, Marijnen CA. Impact of the interval between short-course radiotherapy and surgery on outcomes of rectal cancer patients. Eur J Cancer. 2013; 49:3131–9.
Article12. Hatfield P, Hingorani M, Radhakrishna G, Cooper R, Melcher A, Crellin A, et al. Short-course radiotherapy, with elective delay prior to surgery, in patients with unresectable rectal cancer who have poor performance status or significant co-morbidity. Radiother Oncol. 2009; 92:210–4.
Article13. Francois Y, Nemoz CJ, Baulieux J, Vignal J, Grandjean JP, Partensky C, et al. Influence of the interval between preoperative radiation therapy and surgery on downstaging and on the rate of sphincter-sparing surgery for rectal cancer: the Lyon R90-01 randomized trial. J Clin Oncol. 1999; 17:2396.
Article14. Lee JH, Kim DY, Kim SH, Cho HM, Shim BY, Kim TH, et al. Carcinoembryonic antigen has prognostic value for tumor downstaging and recurrence in rectal cancer after preoperative chemoradiotherapy and curative surgery: a multi-institutional and case-matched control study of KROG 14-12. Radiother Oncol. 2015; 116:202–8.
Article15. Heald RJ, Husband EM, Ryall RD. The mesorectum in rectal cancer surgery: the clue to pelvic recurrence? Br J Surg. 1982; 69:613–6.16. Folkesson J, Birgisson H, Pahlman L, Cedermark B, Glimelius B, Gunnarsson U. Swedish Rectal Cancer Trial: long lasting benefits from radiotherapy on survival and local recurrence rate. J Clin Oncol. 2005; 23:5644–50.
Article17. Sauer R, Becker H, Hohenberger W, Rodel C, Wittekind C, Fietkau R, et al. Preoperative versus postoperative chemoradiotherapy for rectal cancer. N Engl J Med. 2004; 351:1731–40.
Article18. Bujko K, Nowacki MP, Nasierowska-Guttmejer A, Michalski W, Bebenek M, Kryj M. Long-term results of a randomized trial comparing preoperative short-course radiotherapy with preoperative conventionally fractionated chemoradiation for rectal cancer. Br J Surg. 2006; 93:1215–23.
Article19. Fang CB, Gomes CM, Formiga FB, Fonseca VA, Carvalho MP, Klug WA. Is the delayed surgery after neoadjuvant chemoradiation beneficial for locally advanced rectal cancer? Arq Bras Cir Dig. 2013; 26:31–5.20. de Campos-Lobato LF, Geisler DP, da Luz Moreira A, Stocchi L, Dietz D, Kalady MF. Neoadjuvant therapy for rectal cancer: the impact of longer interval between chemoradiation and surgery. J Gastrointest Surg. 2011; 15:444–50.
Article21. Chung MJ, Kim DW, Chung WK, Lee SH, Jeong SK, Hwang JK, et al. Preoperative short- vs. long-course chemoradiotherapy with delayed surgery for locally advanced rectal cancer. Oncotarget. 2017; 8:60479–86.
Article22. Kim JJ, Tannock IF. Repopulation of cancer cells during therapy: an important cause of treatment failure. Nat Rev Cancer. 2005; 5:516–25.
Article23. Dhadda AS, Zaitoun AM, Bessell EM. Regression of rectal cancer with radiotherapy with or without concurrent capecitabine: optimising the timing of surgical resection. Clin Oncol (R Coll Radiol). 2009; 21:23–31.24. Sloothaak DA, Geijsen DE, van Leersum NJ, Punt CJ, Buskens CJ, Bemelman WA, et al. Optimal time interval between neoadjuvant chemoradiotherapy and surgery for rectal cancer. Br J Surg. 2013; 100:933–9.
Article25. Wasserberg N. Interval to surgery after neoadjuvant treatment for colorectal cancer. World J Gastroenterol. 2014; 20:4256–62.
Article26. Barton MB, Keane TJ, Gadalla T, Maki E. The effect of treatment time and treatment interruption on tumour control following radical radiotherapy of laryngeal cancer. Radiother Oncol. 1992; 23:137–43.
Article27. Begg AC, Hofland I, Kummermehr J. Tumour cell repopulation during fractionated radiotherapy: correlation between flow cytometric and radiobiological data in three murine tumours. Eur J Cancer. 1991; 27:537–43.
Article28. Gasinska A, Richter P, Darasz Z, Niemiec J, Bucki K, Malecki K, et al. Gender-related differences in repopulation and early tumor response to preoperative radiotherapy in rectal cancer patients. J Gastrointest Surg. 2011; 15:1568–76.
Article29. Peters LJ, Withers HR. Applying radiobiological principles to combined modality treatment of head and neck cancer: the time factor. Int J Radiat Oncol Biol Phys. 1997; 39:831–6.30. Kwak YK, Kim K, Lee JH, Kim SH, Cho HM, Kim DY, et al. Timely tumor response analysis after preoperative chemoradiotherapy and curative surgery in locally advanced rectal cancer: a multi-institutional study for optimal surgical timing in rectal cancer. Radiother Oncol. 2016; 119:512–8.
Article31. Trott KR, Kummermehr J. Rapid repopulation in radiotherapy: a debate on mechanism. Accelerated repopulation in tumours and normal tissues. Radiother Oncol. 1991; 22:159–60.32. Evans J, Bhoday J, Sizer B, Tekkis P, Swift R, Perez R, et al. Results of a prospective randomised control 6 vs 12 trial: is greater tumour downstaging observed on post treatment MRI if surgery is delayed to 12-weeks versus 6-weeks after completion of neoadjuvant chemoradiotherapy? Ann Oncol. 2016; 27(Suppl 6):vi149.
Article33. Rose BS, Winer EP, Mamon HJ. Perils of the pathologic complete response. J Clin Oncol. 2016; 34:3959–62.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- How to Achieve a Higher Pathologic Complete Response in Patients With Locally Advanced Rectal Cancer Who Receive Preoperative Chemoradiation Therapy
- The Outcome of Preoperative Chemoradiation to Locally Advanced Rectal Cancer
- The Effect of Preoperative Concurrent Chemoradiation in Locally Advanced Rectal Cancer
- How Can We Improve the Tumor Response to Preoperative Chemoradiotherapy for Locally Advanced Rectal Cancer?
- The Effects and Surgical Morbidity of Preoperative Combined Chemoradiotherapy for Locally Advanced Rectal Cancer
