Are We Predicting Disease Progress of the Rectal Cancer Patients without Surgery after Neoadjuvant Chemoradiotherapy?
- Affiliations
-
- 1Department of Surgery, Ewha Womans University School of Medicine, Seoul, Korea.
- 2Department of Surgery, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea. jungwook.huh@gmail.com, lwy555@skku.edu
- 3Department of Surgery, Kangbuk Samsung Hospital, Sungkyunkwan University School of Medicine, Seoul, Korea.
- KMID: 2417853
- DOI: http://doi.org/10.4143/crt.2017.069
Abstract
- PURPOSE
There are patients who do not undergo surgery, regardless of tumor response for neoadjuvant chemoradiotherapy (nCRT) in rectal cancer. However, there have been few reports focused on how oncologic outcomes are worse in these patients. We sought to investigate oncologic outcomes for these non-operated patients with rectal cancer after nCRT.
MATERIALS AND METHODS
A total of 1,063 records of patients with rectal cancer who were treated with nCRT from January 2002 to December 2013 were retrospectively reviewed. We categorized patients into the non-operated group (n=77), transanal local excision (TLE) group (n=54), ortotal mesorectal excision (TME) group (n=932) and compared each group using propensity score matching.
RESULTS
In the non-operated group, the most common reason for no surgery was patient refusal (n=64). Eleven patients were considered to have achieve clinical complete response (cCR), which was an independent prognostic factor of progression-free survival (p=0.045). In patients with disease progression in the non-operated group, the overall survival did not improved according to salvage treatments (p=0.451). The non-operated group showed worse survivals compared to the TLE or TME group before and after matching (p < 0.001). This finding was also noted in the analysis of survival only in patients with cCR.
CONCLUSION
In this study, non-operated patients did not secure oncologic safety regardless of cCR after nCRT. Our results suggest that a non-operative management must be carefully considered even if cCR is achieved.
MeSH Terms
Figure
-
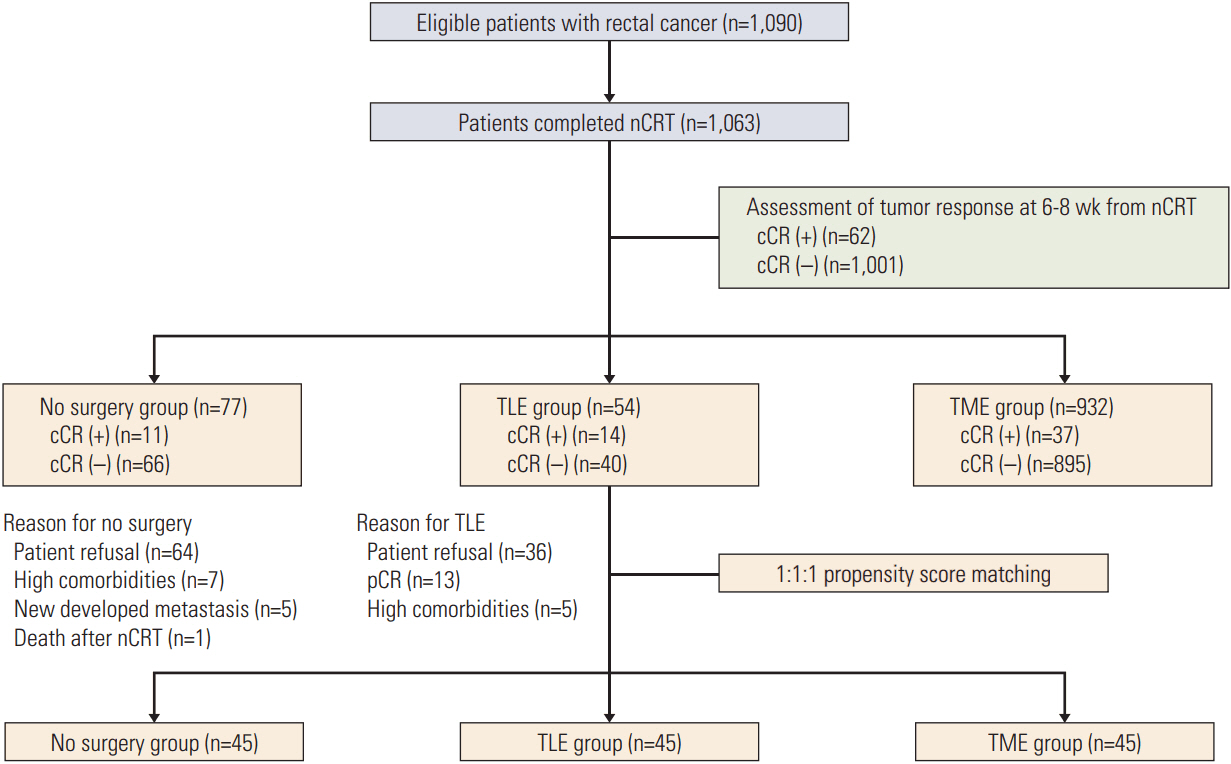
Fig. 1. Flow chart for patient selection. nCRT, neoadjuvant chemoradiotherapy; cCR, clinical complete response; TLE, transanal local excision; TME, total mesorectal excision; pCR, pathologic complete response.
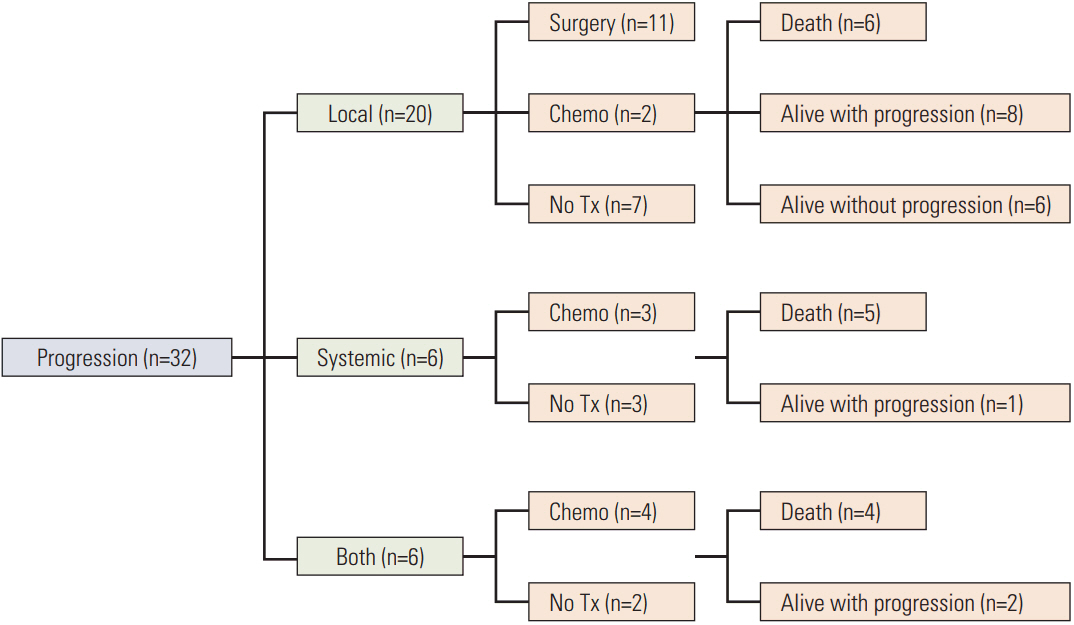
Fig. 2. Clinical course of patients who did not receive surgery after neoadjuvant chemoradiotherapy. Tx, treatment.
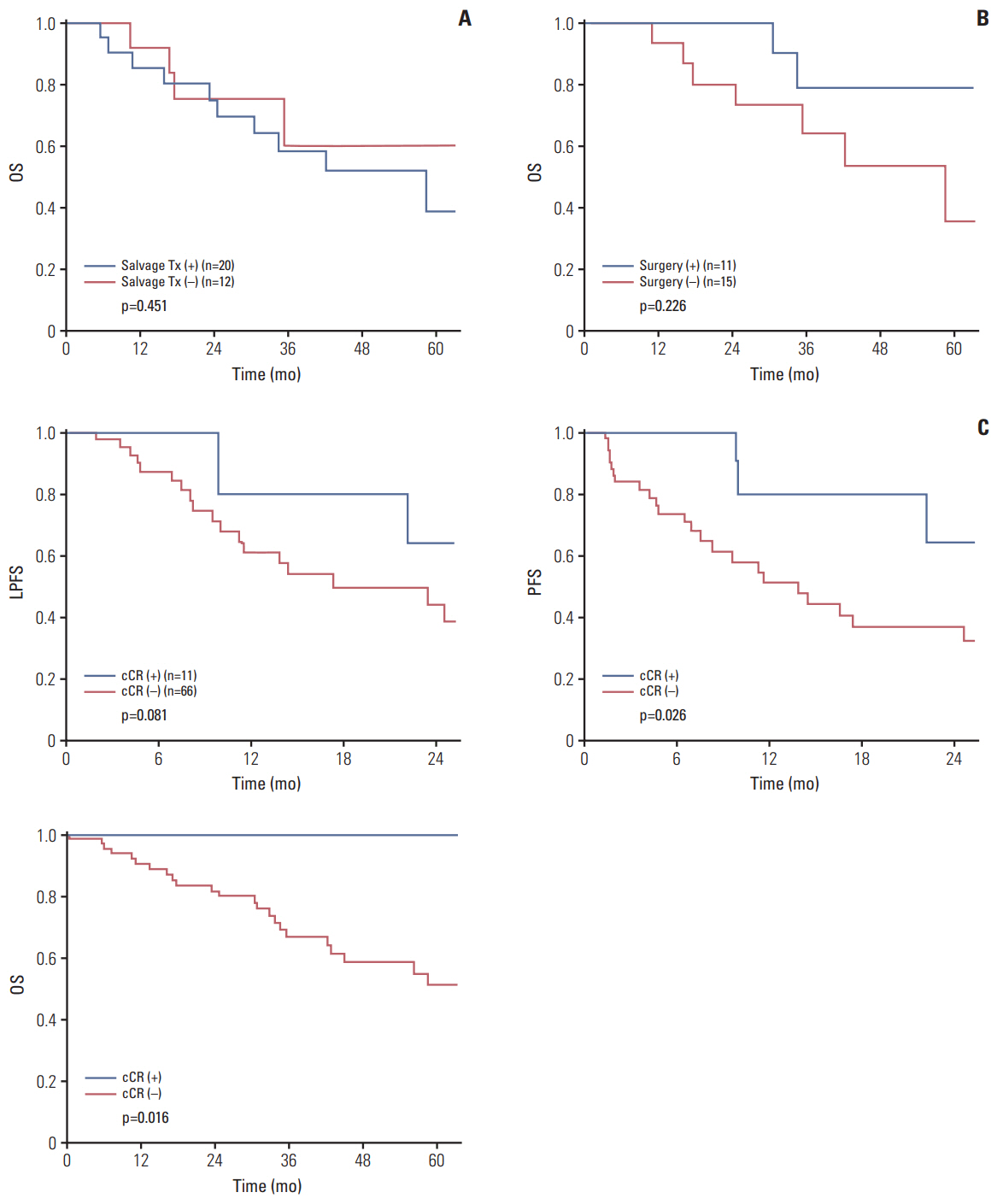
Fig. 3. Kaplan-Meir plots of non-operated group. (A) Overall survival (OS) according to salvage treatment (Tx) in progressed patients (n=32). (B) OS according to salvage surgery in locally progressed patients (n=26). (C) Local progression-free survival (LPFS), progression-free survival (PFS), and OS according to clinical complete response (cCR).
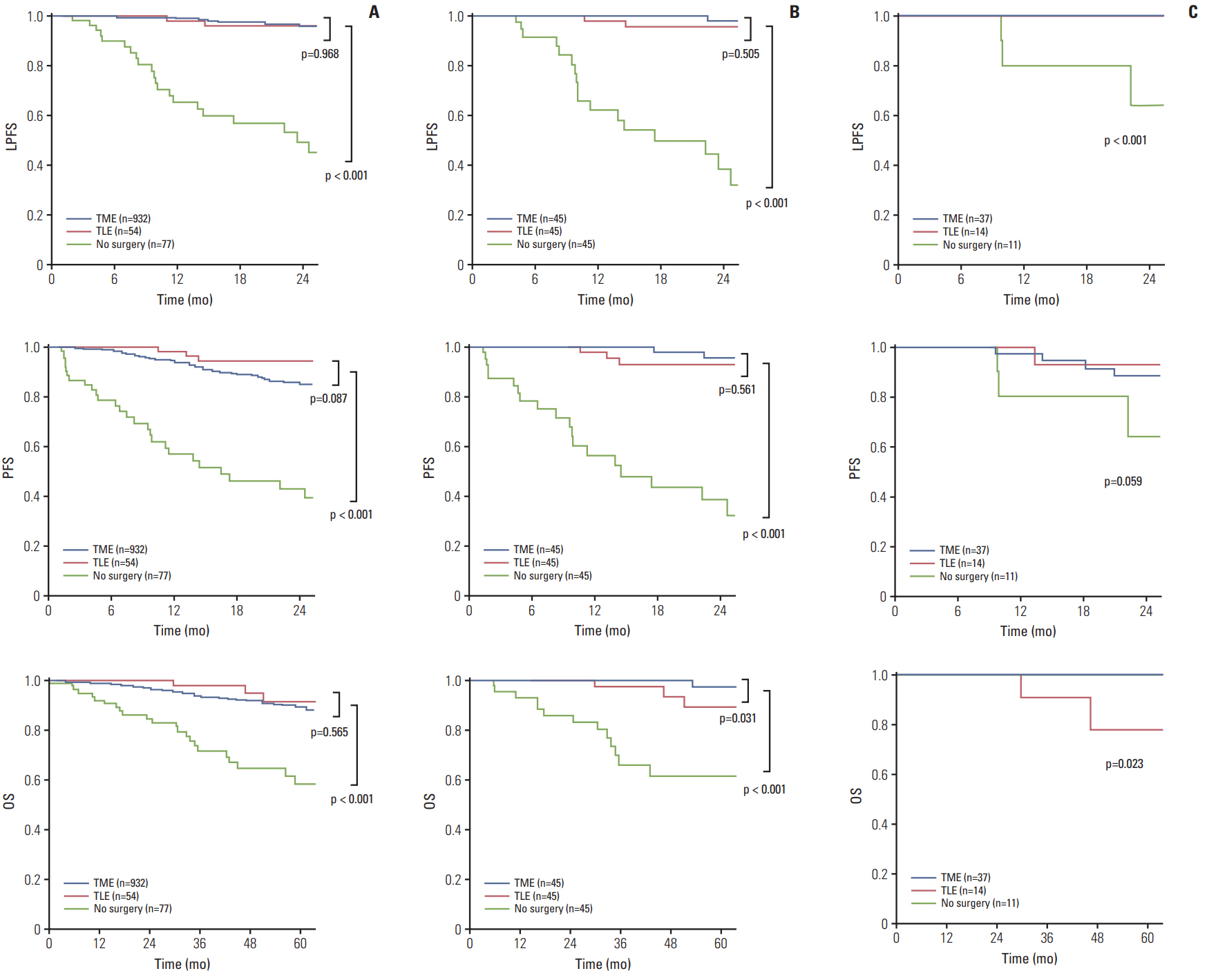
Fig. 4. Kaplan-Meir plots of local progression-free survival (LPFS), progression-free survival (PFS), and overall survival (OS) according to surgery group. (A) Before matching (n=1,063). (B) After matching (n=135). (C) Survival outcomes of patients with clinical complete response (n=62). TME, total mesorectal excision; TLE, transanal local excision.
Reference
-
References
1. Fokas E, Liersch T, Fietkau R, Hohenberger W, Beissbarth T, Hess C, et al. Tumor regression grading after preoperative chemoradiotherapy for locally advanced rectal carcinoma revisited: updated results of the CAO/ARO/AIO-94 trial. J Clin Oncol. 2014; 32:1554–62.
Article2. Arredondo J, Baixauli J, Rodriguez J, Beorlegui C, Arbea L, Zozaya G, et al. Patterns and management of distant failure in locally advanced rectal cancer: a cohort study. Clin Transl Oncol. 2016; 18:909–14.
Article3. Huang MY, Wu CH, Huang CM, Chung FY, Huang CW, Tsai HL, et al. DPYD, TYMS, TYMP, TK1, and TK2 genetic expressions as response markers in locally advanced rectal cancer patients treated with fluoropyrimidine-based chemoradiotherapy. Biomed Res Int. 2013; 2013:931028.4. Wallin U, Rothenberger D, Lowry A, Luepker R, Mellgren A. CEA: a predictor for pathologic complete response after neoadjuvant therapy for rectal cancer. Dis Colon Rectum. 2013; 56:859–68.5. Lai CL, Lai MJ, Wu CC, Jao SW, Hsiao CW. Rectal cancer with complete clinical response after neoadjuvant chemoradiotherapy, surgery, or "watch and wait". Int J Colorectal Dis. 2016; 31:413–9.
Article6. Beets GL, Figueiredo NL, Habr-Gama A, van de Velde CJ. A new paradigm for rectal cancer: Organ preservation: Introducing the International Watch & Wait Database (IWWD). Eur J Surg Oncol. 2015; 41:1562–4.7. Oh BY, Park YA, Huh JW, Cho YB, Yun SH, Lee WY, et al. Metformin enhances the response to radiotherapy in diabetic patients with rectal cancer. J Cancer Res Clin Oncol. 2016; 142:1377–85.
Article8. Hur H, Kim NK, Min BS, Baik SH, Lee KY, Koom WS, et al. Can a biomarker-based scoring system predict pathologic complete response after preoperative chemoradiotherapy for rectal cancer? Dis Colon Rectum. 2014; 57:592–601.
Article9. Gollins S, Sebag-Montefiore D. Neoadjuvant treatment strategies for locally advanced rectal cancer. Clin Oncol (R Coll Radiol). 2016; 28:146–51.
Article10. Lee SH, Lee KC, Choi JH, Oh JH, Baek JH, Park SH, et al. Chemoradiotherapy followed by surgery in rectal cancer: improved local control using a moderately high pelvic radiation dose. Jpn J Clin Oncol. 2008; 38:112–21.
Article11. Yeh CH, Chen MF, Lai CH, Huang WS, Lee SP, Chen WC. Comparison of treatment results between surgery alone, preoperative short-course radiotherapy, or long-course concurrent chemoradiotherapy in locally advanced rectal cancer. Int J Clin Oncol. 2012; 17:482–90.
Article12. Hingorani M, Hartley JE, Greenman J, Macfie J. Avoiding radical surgery after pre-operative chemoradiotherapy: a possible therapeutic option in rectal cancer? Acta Oncol. 2012; 51:275–84.
Article13. Habr-Gama A, Sabbaga J, Gama-Rodrigues J, Sao Juliao GP, Proscurshim I, Bailao Aguilar P, et al. Watch and wait approach following extended neoadjuvant chemoradiation for distal rectal cancer: are we getting closer to anal cancer management? Dis Colon Rectum. 2013; 56:1109–17.14. Smith FM, Rao C, Oliva Perez R, Bujko K, Athanasiou T, Habr-Gama A, et al. Avoiding radical surgery improves early survival in elderly patients with rectal cancer, demonstrating complete clinical response after neoadjuvant therapy: results of a decision-analytic model. Dis Colon Rectum. 2015; 58:159–71.15. Habr-Gama A, Gama-Rodrigues J, Sao Juliao GP, Proscurshim I, Sabbagh C, Lynn PB, et al. Local recurrence after complete clinical response and watch and wait in rectal cancer after neoadjuvant chemoradiation: impact of salvage therapy on local disease control. Int J Radiat Oncol Biol Phys. 2014; 88:822–8.
Article16. Renehan AG, Malcomson L, Emsley R, Gollins S, Maw A, Myint AS, et al. Watch-and-wait approach versus surgical resection after chemoradiotherapy for patients with rectal cancer (the OnCoRe project): a propensity-score matched cohort analysis. Lancet Oncol. 2016; 17:174–83.
Article17. Li J, Liu H, Yin J, Liu S, Hu J, Du F, et al. Wait-and-see or radical surgery for rectal cancer patients with a clinical complete response after neoadjuvant chemoradiotherapy: a cohort study. Oncotarget. 2015; 6:42354–61.
Article18. Hughes R, Harrison M, Glynne-Jones R. Could a wait and see policy be justified in T3/4 rectal cancers after chemo-radiotherapy? Acta Oncol. 2010; 49:378–81.
Article19. dos Santos LV, dos Anjos Jacome AA, Carcano FM, da Silveira Nogueira Lima JP, Serrano SV. Watch and wait policy remains experimental for the management of rectal cancer. Colorectal Dis. 2010; 12:833.
Article20. Glynne-Jones R, Hughes R. Critical appraisal of the 'wait and see' approach in rectal cancer for clinical complete responders after chemoradiation. Br J Surg. 2012; 99:897–909.
Article21. Yu CS, Yun HR, Shin EJ, Lee KY, Kim NK, Lim SB, et al. Local excision after neoadjuvant chemoradiation therapy in advanced rectal cancer: a national multicenter analysis. Am J Surg. 2013; 206:482–7.
Article22. Noh JM, Park W, Kim JS, Koom WS, Kim JH, Choi DH, et al. Outcome of local excision following preoperative chemoradiotherapy for clinically T2 distal rectal cancer: a multicenter retrospective study (KROG 12-06). Cancer Res Treat. 2014; 46:243–9.
Article23. Lee NK, Kim DY, Kim SY, Oh JH, Park W, Choi DH, et al. Clinical outcomes of local excision following preoperative chemoradiotherapy for locally advanced rectal cancer. Cancer Res Treat. 2014; 46:158–64.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Clinical characteristics of rectal cancer patients with neoadjuvant chemoradiotherapy: a nationwide population-based cohort study in South Korea
- Clinical Implication of Lateral Pelvic Lymph Node Metastasis in Rectal Cancer Treated with Neoadjuvant Chemoradiotherapy
- Selection of Adjuvant Treatment Without Neoadjuvant Chemoradiotherapy for Patients With Rectal Cancer: Room for Further Investigation
- Correlation between tumor regression grade and rectal volume in neoadjuvant concurrent chemoradiotherapy for rectal cancer
- Long-term bowel functional outcomes following anal sphincter-preserving surgery for upper and middle rectal cancer: a single-center longitudinal study
