Early Valuable Risk Stratification with Hemoglobin Level and Neutrophil to Lymphocyte Ratio in Patients with Non-ST-Elevation Myocardial Infarction Having an Early Invasive Strategy
- Affiliations
-
- 1Division of Cardiology, Department of Internal Medicine, Gunsan Medical Center, Gunsan, Korea.
- 2Division of Cardiology, Department of Internal Medicine, Chonnam National University Hospital, Gwangju, Korea. myungho@chollian.net
- 3Division of Cardiology, Department of Internal Medicine, Gangjin Medical Center, Gangjin, Korea.
- 4Division of Cardiology, Department of Internal Medicine, Kyungpook National University Hospital, Daegu, Korea.
- 5Division of Cardiology, Department of Internal Medicine, Yeungnam University Hospital, Daegu, Korea.
- 6Division of Cardiology, Department of Internal Medicine, Chungnam National University Hospital, Daejeon, Korea.
- 7Division of Cardiology, Department of Internal Medicine, Chonbuk National University Hospital, Jeonju, Korea.
- 8Division of Cardiology, Department of Internal Medicine, Seoul National University Hospital, Seoul, Korea.
- KMID: 2416258
- DOI: http://doi.org/10.12997/jla.2018.7.1.50
Abstract
OBJECTIVE
The complete blood count is the most widely available laboratory data in the early in-hospital period after acute myocardial infarction. We assessed the clinical utility of the combined use of hemoglobin (Hb) level and neutrophil to lymphocyte ratio (N/L) for early risk stratification in patients with non-ST-elevation myocardial infarction (STEMI).
METHODS
We analyzed 6,157 consecutive patients with non-STEMI (65±12.4 years, male 69%) were included in the final analysis. Patients were categorized into 3 groups by using the median value of N/L (4.42) and the presence of anemia (Hb <13 mg/dL in men and <12 mg/dL in women): group I, low N/L & no anemia (n=3,170); group II, no group I or III (n=2,168); group III, high N/L & anemia (n=819).
RESULTS
There were significant differences on clinical outcomes during 180-day follow-up among 3 groups. The prognostic discriminatory capacity of the combined use of Hb level and N/L was also significant in high-risk subgroups, such as patients with a renal dysfunction, multivessel coronary disease, low ejection fraction, and even in those having higher mortality risk based on the thrombolysis in myocardial infarction risk score. In a multi-variate logistic regression, after adjusting for multiple covariates, group III had higher incidence of major adverse cardiac events at 180-day (hazard ratio, 2.4; 95% confidence interval, 1.5-4.0;p≤0.001) compared with group I.
CONCLUSIONS
The combined use of Hb level and N/L provides valuable timely information for early risk stratification in patients with non-STEMI.
Keyword
MeSH Terms
Figure
-

Fig. 1 Flow chart of the study population. KAMIR-NIH; Korea Acute Myocardial Infarction Registry-National Institute of Health, STEMI; ST-elevation myocardial infarction, N/L; neutrophil to lymphocyte ratio.
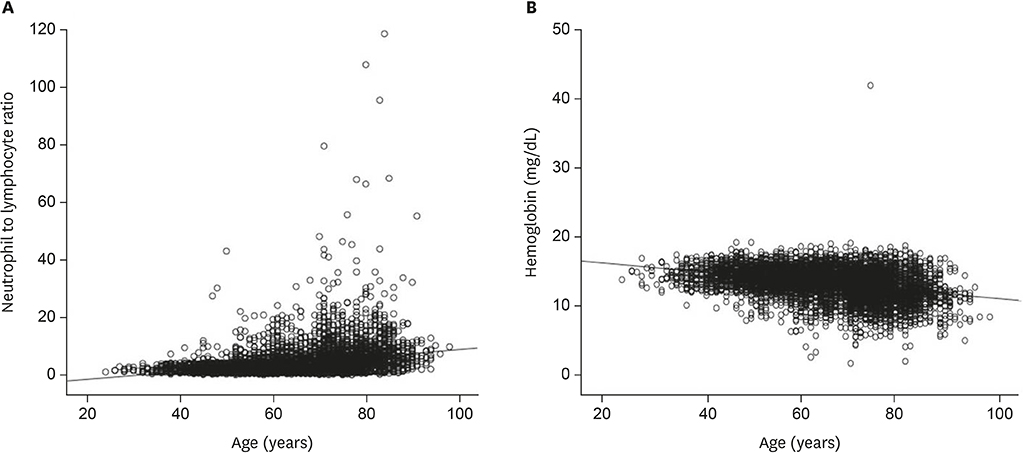
Fig. 2 Simple correlation analysis between age and (A) N/L (r=0.305; p<0.001) and (B) Hb level (r=−0.356; p<0.001). N/L; neutrophil to lymphocyte ratio, Hb; hemoglobin.

Fig. 3 (A) The 180-day mortality and (B) MACEs stratified by Hb level and N/L: no anemia & low N/L (n=3,170); no anemia & high N/L (n=1,134); anemia & low N/L (n=1,034); and anemia & high N/L (n=819). MACE; major adverse cardiac event, Hb; hemoglobin, N/L; neutrophil to lymphocyte ratio.

Fig. 4 The 180-day mortality according to (A) TIMI risk score and (B) GRACE score for non-STEMI in all patients (n=6,157). TIMI; thrombolysis in myocardial infarction, GRACE; Global Registry of Acute Coronary Events, STEMI; ST-elevation myocardial infarction.

Fig. 5 The 180-day MACEs according to (A) TIMI risk score and (B) GRACE score for non-STEMI in all patients (n=6,157). MACE; major adverse cardiac event, TIMI; thrombolysis in myocardial infarction, GRACE; Global Registry of Acute Coronary Events, STEMI; ST-elevation myocardial infarction.
Reference
-
1. Maseri A, Rebuzzi AG, Cianflone D. Need for a composite risk stratification of patients with unstable coronary syndromes tailored to clinical practice. Circulation. 1997; 96:4141–4142.2. Amsterdam EA, Wenger NK, Brindis RG, Casey DE Jr, Ganiats TG, Holmes DR Jr, et al. 2014 AHA/ACC guideline for the management of patients with non-ST-elevation acute coronary syndromes: executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2014; 130:2354–2394.
Article3. Becker RC, Burns M, Gore JM, Spencer FA, Ball SP, French W, et al. Early assessment and in-hospital management of patients with acute myocardial infarction at increased risk for adverse outcomes: a nationwide perspective of current clinical practice. Am Heart J. 1998; 135:786–796.
Article4. Horne BD, Anderson JL, John JM, Weaver A, Bair TL, Jensen KR, et al. Which white blood cell subtypes predict increased cardiovascular risk? J Am Coll Cardiol. 2005; 45:1638–1643.
Article5. Núñez J, Núñez E, Bodí V, Sanchis J, Miñana G, Mainar L, et al. Usefulness of the neutrophil to lymphocyte ratio in predicting long-term mortality in ST segment elevation myocardial infarction. Am J Cardiol. 2008; 101:747–752.
Article6. Lee PC, Kini AS, Ahsan C, Fisher E, Sharma SK. Anemia is an independent predictor of mortality after percutaneous coronary intervention. J Am Coll Cardiol. 2004; 44:541–546.
Article7. Nikolsky E, Aymong ED, Halkin A, Grines CL, Cox DA, Garcia E, et al. Impact of anemia in patients with acute myocardial infarction undergoing primary percutaneous coronary intervention: analysis from the Controlled Abciximab and Device Investigation to Lower Late Angioplasty Complications (CADILLAC) Trial. J Am Coll Cardiol. 2004; 44:547–553.
Article8. Cho KH, Jeong MH, Ahmed K, Hachinohe D, Choi HS, Chang SY, et al. Value of early risk stratification using hemoglobin level and neutrophil-to-lymphocyte ratio in patients with ST-elevation myocardial infarction undergoing primary percutaneous coronary intervention. Am J Cardiol. 2011; 107:849–856.
Article9. Nutritional anaemias. Report of a WHO scientific group. World Health Organ Tech Rep Ser. 1968; 405:5–37.10. Gibson CM, Schömig A. Coronary and myocardial angiography: angiographic assessment of both epicardial and myocardial perfusion. Circulation. 2004; 109:3096–3105.11. Eagle KA, Lim MJ, Dabbous OH, Pieper KS, Goldberg RJ, Van de Werf F, et al. A validated prediction model for all forms of acute coronary syndrome: estimating the risk of 6-month postdischarge death in an international registry. JAMA. 2004; 291:2727–2733.
Article12. Antman EM, Cohen M, Bernink PJ, McCabe CH, Horacek T, Papuchis G, et al. The TIMI risk score for unstable angina/non-ST elevation MI: a method for prognostication and therapeutic decision making. JAMA. 2000; 284:835–842.
Article13. Wu WC, Rathore SS, Wang Y, Radford MJ, Krumholz HM. Blood transfusion in elderly patients with acute myocardial infarction. N Engl J Med. 2001; 345:1230–1236.
Article14. Al Falluji N, Lawrence-Nelson J, Kostis JB, Lacy CR, Ranjan R, Wilson AC, et al. Effect of anemia on 1-year mortality in patients with acute myocardial infarction. Am Heart J. 2002; 144:636–641.
Article15. Anderson RD, White HD, Ohman EM, Wagner GS, Krucoff MW, Armstrong PW, et al. Predicting outcome after thrombolysis in acute myocardial infarction according to ST-segment resolution at 90 minutes: a substudy of the GUSTO-III trial. Am Heart J. 2002; 144:81–88.
Article16. Best PJ, Lennon R, Ting HH, Bell MR, Rihal CS, Holmes DR Jr, et al. The impact of renal insufficiency on clinical outcomes in patients undergoing percutaneous coronary interventions. J Am Coll Cardiol. 2002; 39:1113–1119.
Article17. Gottlieb SS, McCarter RJ, Vogel RA. Effect of beta-blockade on mortality among high-risk and low-risk patients after myocardial infarction. N Engl J Med. 1998; 339:489–497.
Article18. Wahr JA. Myocardial ischaemia in anaemic patients. Br J Anaesth. 1998; 81:Suppl 1. 10–15.19. Most AS, Ruocco NA Jr, Gewirtz H. Effect of a reduction in blood viscosity on maximal myocardial oxygen delivery distal to a moderate coronary stenosis. Circulation. 1986; 74:1085–1092.
Article20. Kaiafa G, Kanellos I, Savopoulos C, Kakaletsis N, Giannakoulas G, Hatzitolios AI. Is anemia a new cardiovascular risk factor? Int J Cardiol. 2015; 186:117–124.
Article21. Yoshikawa H, Powell WJ Jr, Bland JH, Lowenstein E. Effect of acute anemia on experimental myocardial ischemia. Am J Cardiol. 1973; 32:670–678.
Article22. Hoffman M, Blum A, Baruch R, Kaplan E, Benjamin M. Leukocytes and coronary heart disease. Atherosclerosis. 2004; 172:1–6.
Article23. Barron HV, Cannon CP, Murphy SA, Braunwald E, Gibson CM. Association between white blood cell count, epicardial blood flow, myocardial perfusion, and clinical outcomes in the setting of acute myocardial infarction: a thrombolysis in myocardial infarction 10 substudy. Circulation. 2000; 102:2329–2334.
Article24. Duffy BK, Gurm HS, Rajagopal V, Gupta R, Ellis SG, Bhatt DL. Usefulness of an elevated neutrophil to lymphocyte ratio in predicting long-term mortality after percutaneous coronary intervention. Am J Cardiol. 2006; 97:993–996.
Article25. Ricevuti G, Mazzone A, De Servi S, Specchia G, Fratino P. New trends in coronary artery disease: the role of granulocyte activation. Atherosclerosis. 1989; 78:261–265.
Article26. Madjid M, Awan I, Willerson JT, Casscells SW. Leukocyte count and coronary heart disease: implications for risk assessment. J Am Coll Cardiol. 2004; 44:1945–1956.27. Onsrud M, Thorsby E. Influence of in vivo hydrocortisone on some human blood lymphocyte subpopulations. I. Effect on natural killer cell activity. Scand J Immunol. 1981; 13:573–579.
Article28. Thomson SP, Gibbons RJ, Smars PA, Suman VJ, Pierre RV, Santrach PJ, et al. Incremental value of the leukocyte differential and the rapid creatine kinase-MB isoenzyme for the early diagnosis of myocardial infarction. Ann Intern Med. 1995; 122:335–341.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Risk Stratification of Acute Coronary Syndrome
- Updates in the management of patients with acute coronary syndrome
- Influence of the Timing of Percutaneous Coronary Intervention on Clinical Outcomes in Non-ST-Elevation Myocardial Infarction
- Diagnosis and management of acute coronary syndrome
- Serum Myoglobin in the Early Phase of Acute Myocardial Infarction
