J Korean Assoc Pediatr Surg.
2018 Jun;24(1):20-25. 10.13029/jkaps.2018.24.1.20.
Santulli Enterostomy: A Considerable Method for Patients Who Require Proximal Enterostomy
- Affiliations
-
- 1Department of Pediatric Surgery, Severance Children's Hospital, Yonsei University College of Medicine, Seoul, Korea. jtoh@yuhs.ac
- KMID: 2415882
- DOI: http://doi.org/10.13029/jkaps.2018.24.1.20
Abstract
- PURPOSE
Santulli enterostomy has been used for various surgical abdominal conditions that require temporary diversion of bowel during a neonatal period. The aim of this study was to report clinical outcomes of Santulli enterostomy and to evaluate its usefulness.
METHODS
Between January 2000 and December 2016, 40 neonates who underwent Santulli enterostomy were enrolled; Santulli enterostomies were performed for 25 patients without previous laparotomy (primary Santulli group) and 15 patients with previous laparotomy (secondary Santulli group).
RESULTS
Small bowel atresia is the first common indication of Santulli enterostomy (22/40, 55.0%), and luminal discrepancy between proximal and distal bowel was the most common determinant factor of Santulli enterostomy (17/40, 42.5%). The median age at surgery and mean birth weight were 2 days and 2,480 g respectively in the primary group, and 71 days, 2,340 g respectively in the secondary group. Operation time was significantly longer in the secondary group than the primary group (156±48 minutes vs. 224±95 minutes, p=0.019), and there was no difference in the time taken to initiation of oral feeding between the two groups. Santulli enterostomy closure was performed at median 65 days after Santulli enterostomy for primary group and 70 days for secondary group. Six complications (15.0%) were found after Santulli enterostomy, and nine complications (24.3%) after Santulli enterostomy closure (p=0.302). The incidence of complications was significantly higher in secondary group than in primary group (4.5% vs. 53.3%, p=0.001), and the reoperation rate was also significantly higher in the secondary group (4.5% vs. 46.7%, p=0.004).
CONCLUSION
Santulli enterostomy could be applied as a temporary enterostomy in neonatal patients with various surgical abdominal diseases. Considering the high complication rate after secondary Santulli enterostomy closure, decision making on the timing of enterostomy closure should be done with caution.
MeSH Terms
Figure
-
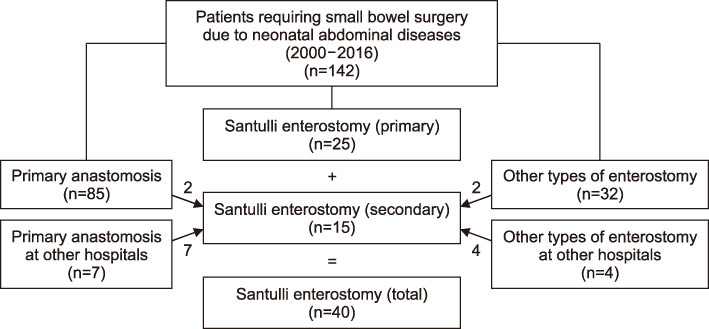
Fig. 1. Flowchart showing the study design including 40 patients enrolled in this study.
Reference
-
1. van Zoonen AG, Schurink M, Bos AF, Heineman E, Hulscher JB. Ostomy creation in neonates with acute abdominal disease: friend or foe? Eur J Pediatr Surg. 2012; 22:295–299.
Article2. Santulli TV, Blanc WA. Congenital atresia of the intestine: pathogenesis and treatment. Ann Surg. 1961; 154:939–948.3. Sapin E, Carricaburu E, De Boissieu D, Goutail-Flaud MF, Benammar S, Helardot PG. Conservative intestinal surgery to avoid short-bowel syndrome in multiple intestinal atresias and necrotizing enterocolitis: 6 cases treated by multiple anastomoses and Santulli-type enterostomy. Eur J Pediatr Surg. 1999; 9:24–28.4. Yeung F, Tam YH, Wong YS, Tsui SY, Wong HY, Pang KK, et al. Early reoperations after primary repair of Jejunoileal atresia in newborns. J Neonatal Surg. 2016; 5:42.
Article5. Rees CM, Eaton S, Khoo AK, Kiely EM. Members of NET Trial Group. Pierro A. Peritoneal drainage does not stabilize extremely low birth weight infants with perforated bowel: data from the NET Trial. J Pediatr Surg. 2010; 45:324–328. discussion 328–9.6. Vanamo K, Rintala R, Lindahl H. The Santulli enterostomy in necrotising enterocolitis. Pediatr Surg Int. 2004; 20:692–694.
Article7. Zani A, Lauriti G, Li Q, Pierro A. The timing of stoma closure in infants with necrotizing enterocolitis: a systematic review and meta-analysis. Eur J Pediatr Surg. 2017; 27:7–11.
Article8. Ahlgren LS. Apple peel jejunal atresia. J Pediatr Surg. 1987; 22:451–453.
Article9. Tepetes K, Liakou P, Balogiannis I. The use of the Santulli enterostomy. World J Surg. 2007; 31:1343–1344.10. Steinau G, Ruhl KM, Hörnchen H, Schumpelick V. Enterostomy complications in infancy and childhood. Langenbecks Arch Surg. 2001; 386:346–349.
Article11. Lee J, Kang MJ, Kim HS, Shin SH, Kim HY, Kim EK, et al. Enterostomy closure timing for minimizing postoperative complications in premature infants. Pediatr Neonatol. 2014; 55:363–368.
Article12. Struijs MC, Sloots CE, Hop WC, Tibboel D, Wijnen RM. The timing of ostomy closure in infants with necrotizing enterocolitis: a systematic review. Pediatr Surg Int. 2012; 28:667–672.
Article13. Waldhausen JH, Sawin RS. Improved long-term outcome for patients with jejunoileal apple peel atresia. J Pediatr Surg. 1997; 32:1307–1309.
Article14. Wit J, Sellin S, Degenhardt P, Scholz M, Mau H. Is the Bishop-Koop anastomosis in treatment of neonatal ileus still current? Chirurg. 2000; 71:307–310.15. Gause CD, Hayashi M, Haney C, Rhee D, Karim O, Weir BW, et al. Mucous fistula refeeding decreases parenteral nutrition exposure in postsurgical premature neonates. J Pediatr Surg. 2016; 51:1759–1765.
Article16. Aguayo P, Fraser JD, Sharp S, St Peter SD, Ostlie DJ. Stomal complications in the newborn with necrotizing enterocolitis. J Surg Res. 2009; 157:275–278.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Determining the Timing for the Enterostomy Repair using Age-based Analysis
- Experience with Enterostomy Closure in Very Low Birth Weight Infants
- Clinical characteristics of ovarian cancer patients who underwent enterostomy
- The Use of Palliative Endoscopic Ultrasound-guided Enterostomy to Treat Small Bowel Obstruction in Two Patients with Advanced Malignancies
- Enterocolitis In Hirschsprung's Disease
