Tracheal pleomorphic adenoma with coexisting pulmonary tuberculoma
- Affiliations
-
- 1Department of Pulmonary and Critical Care Medicine, Kosin University Gospel Hospital, Kosin University College of Medicine, Busan, Korea. oaks70@hanmail.net
- KMID: 2415744
- DOI: http://doi.org/10.12701/yujm.2018.35.1.114
Abstract
- Tracheal tumors are rare and difficult to diagnose. Moreover, delays in diagnosis are very common because the symptoms are nonspecific. As a result, tracheal tumors are commonly mistreated as chronic obstructive pulmonary disease or bronchial asthma. We report a case of a 49-year-old male who presented with a 3-month history of dyspnea and cough. Chest computed tomography scan showed a 1.5×1.3 cm homogenous tumor originating from the right lateral wall of the tracheobronchial angle into the tracheal lumen as well as a 0.5×0.4 cm round nodular lesion at the right upper lobe with multiple mediastinal lymph nodes enlargement. Bronchoscopic findings revealed a broad-based, polypoid lesion nearly obstructing the airway of the right main bronchus. The patient was diagnosed with pleomorphic adenoma which is the most common benign tumor of the salivary glands, but rarely appears in the trachea. Upon surgery, tracheal pleomorphic adenoma and co-existing active pulmonary tuberculoma that had been mistreated as bronchial asthma over 3 months was revealed. Following surgery, the patient underwent anti-tuberculosis treatment. No recurrence has been detected in the 3 years since treatment and the patient is now asymptomatic.
MeSH Terms
Figure
-

Fig. 1. (A) Chest x-ray shows a round mass shadow in the lower tracheal level (black arrows). (B) Three-dimensional airway CT shows a round mass in lower trachea level (white arrows). (C) Lung setting of CT scan of the chest shows a 1.5×1.3 cm homogenous mass in the right lateral inner wall of the trachea (black arrows). (D) A 0.5×0.4 cm round shaped nodule in the posterior zone of right upper lobe seen on the CT (arrowhead). CT, computed tomography.

Fig. 2. (A) Bronchoscopic shows a polypoid and broad mass originated from right side of lower trachea have rich engorged blood vessels on the tumor surface. (B) The mass nearly occludes the orifice of right main bronchus.

Fig. 3. The excised tumor. (A) Macroscopic appearance of the pleomorphic adenoma; there is a well-circumscribed grey colored measuring 1.5×1.3×1.3 cm mass; cut surface shows a well-defined ovoid mass without necrosis or invasion into the paratracheal tissues. (B, C) Microscopic appearance of the pleomorphic adenoma; ductal and myxoid components in the chondromyxoid stroma consisted of eosinophilic cuboidal epithelium and myoepithelium (H&E stain, B, ×12.5; C, ×400).

Fig. 4. Wedge resected nodule in the right upper lobe. (A) Macroscopic appearance of the lesion; surrounded by grey capsule, 0.5×0.4× 0.4 cm ovoid nodule, the cut surface of the nodule is homogenously solid and white with yellow spot. (B) Chronic granulomatous inflammation with caseous necrosis (H&E stain, ×200). (C) Acid-fast stain-positive bacilli are identified (×1,000).
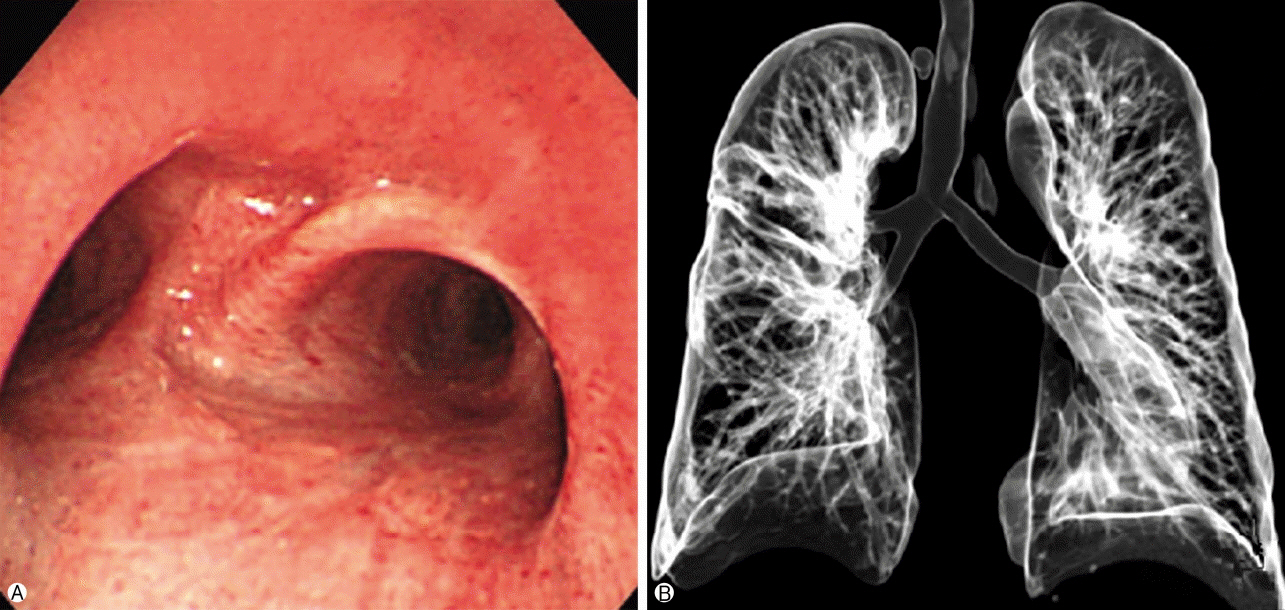
Fig. 5. The post-operative bronchoscopy and 3D airway CT at 2 years after operation (A, B) shows no recurrence of the tracheal lesion compared to pre-operative bronchoscopy and 3D airway CT. 3D, three-dimensional; CT, computed tomography.
Reference
-
1. Park KS, Sung WJ. Pleomorphic adenoma of the trachea: a case report. Korean J Pathol. 2013; 47:399–401.
Article2. Ashwaq AM, Sani A. Pleomorphic adenoma of the trachea. Med J Malaysia. 2007; 62:162–3.3. Chowdhury Q, Rahman MA, Sultana L, Islam MA, Chowdhury GM. Tracheal adenocarcinoma treated with adjuvant radiation: a case report and literature review. Case Rep Oncol. 2013; 6:280–4.
Article4. Pinkston JA, Cole P. Incidence rates of salivary gland tumors: results from a population-based study. Otolaryngol Head Neck Surg. 1999; 120:834–40.
Article5. Spencer H. Bronchial mucous gland tumours. Virchows Arch A Pathol Anat Histol. 1979; 383:101–15.
Article6. Moran CA, Suster S, Askin FB, Koss MN. Benign and malignant salivary gland-type mixed tumors of the lung. Clinicopathologic and immunohistochemical study of eight cases. Cancer. 1994; 73:2481–90.
Article7. Ang KL, Dhannapuneni VR, Morgan WE, Soomro IN. Primary pulmonary pleomorphic adenoma. An immunohistochemical study and review of the literature. Arch Pathol Lab Med. 2003; 127:621–2.8. Payne WS, Schier J, Woolner LB. Mixed tumors of the bronchus (salivary gland type). J Thorac Cardiovasc Surg. 1965; 49:663–8.
Article9. Matsubara M, Yasuo M, Tanabe T, Tsushima K, Urushihata K, Yamamoto H, et al. Pleomorphic adenoma with an endobronchial resection. Intern Med. 2008; 47:1117–20.
Article10. Tanigaki T, Shoyama Y, Iwasaki M, Abe Y, Nakamura M, Inoue H. Pleomorphic adenoma in the lung. Monaldi Arch Chest Dis. 2002; 57:30–2.11. Fitchett J, Luckraz H, Gibbs A, O'Keefe P. A rare case of primary pleomorphic adenoma in main bronchus. Ann Thorac Surg. 2008; 86:1025–6.
Article12. Aribas OK, Kanat F, Avunduk MC. Pleomorphic adenoma of the trachea mimicking bronchial asthma: report of a case. Surg Today. 2007; 37:493–5.
Article13. Schneider P, Schirren J, Muley T, Vogt-Moykopf I. Primary tracheal tumors: experience with 14 resected patients. Eur J Cardiothorac Surg. 2001; 20:12–8.
Article14. Goto T, Maeshima A, Akanabe K, Hamaguchi R, Wakaki M, Oyamada Y, et al. Bronchial pleomorphic adenoma coexisting with lung cancer. Ann Thorac Cardiovasc Surg. 2011; 17:174–7.
Article15. Demirağ F, Topçu S, Kurul C, Memiş L, Altinok T. Malignant pleomorphic adenoma (malignant mixed tumor) of the trachea: a case report and review of the literature. Eur Arch Otorhinolaryngol. 2003; 260:96–9.
Article16. Shim TS. Diagnosis and treatment of latent tuberculosis infection. Korean J Med. 2012; 82:284–90. Korean.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Pleomorphic adenoma of the trachea
- Pulmonary Pleomorphic Adenoma: Report of a Rare Case
- A Case of Pleomorphic Adenoma Occurred on Philtrum
- Multimodality Imaging of Metastasizing Pleomorphic Adenoma Presenting as a Solitary Pulmonary Nodule without Local Tumor Recurrence: A Case Report
- A Case of Pleomorphic Adenoma Manifested as a Subcutaneous Nodule
