Minimally Invasive Horizontal Intercartilaginous Incision during Tracheostomy – A Cadaveric Study
- Affiliations
-
- 1Department of Otolaryngology-Head and Neck Surgery, Chonnam National University Hospital, Korea. blessed@jnu.ac.kr
- 2Department of Anatomy, Medical School, Chonnam National University, Korea. atlas@jnu.ac.kr
- KMID: 2415442
- DOI: http://doi.org/10.11637/kjpa.2018.31.2.57
Abstract
- The paper describes a minimally invasive tracheostomy technique that uses an intercartilaginous incision without resection of the tracheal cartilage and discusses its feasibility. A total of 20 adult cadavers (13 males and 7 females) were included in this study. The distance from the arch of the cricoid cartilage to the thyroid isthmus, maximal displacement of the thyroid isthmus, number of tracheal rings underneath the thyroid isthmus, and maximally opened distance resulting from an intercartilaginous incision were measured. The mean distance from the arch of the cricoid cartilage to the thyroid isthmus was 21.4±5.0 mm. The thyroid isthmus mainly overlaid the 3rd and 4th tracheal rings. The mean maximal displacement of the thyroid isthmus was 9.0±2.8 mm. Minimally invasive tracheostomy via an intercartilaginous incision is a feasible technique. A skin incision 2 cm below the cricoid cartilage enables exposure of the thyroid isthmus and anular ligament between the 2nd and 3rd tracheal rings. The intercartilaginous incision allows sufficient space for the tracheostomy tube. An intercartilaginous incision without resection of a tracheal ring can be a good alternative tracheostomy technique, especially for patients who require transient tracheostomy.
MeSH Terms
Figure
-
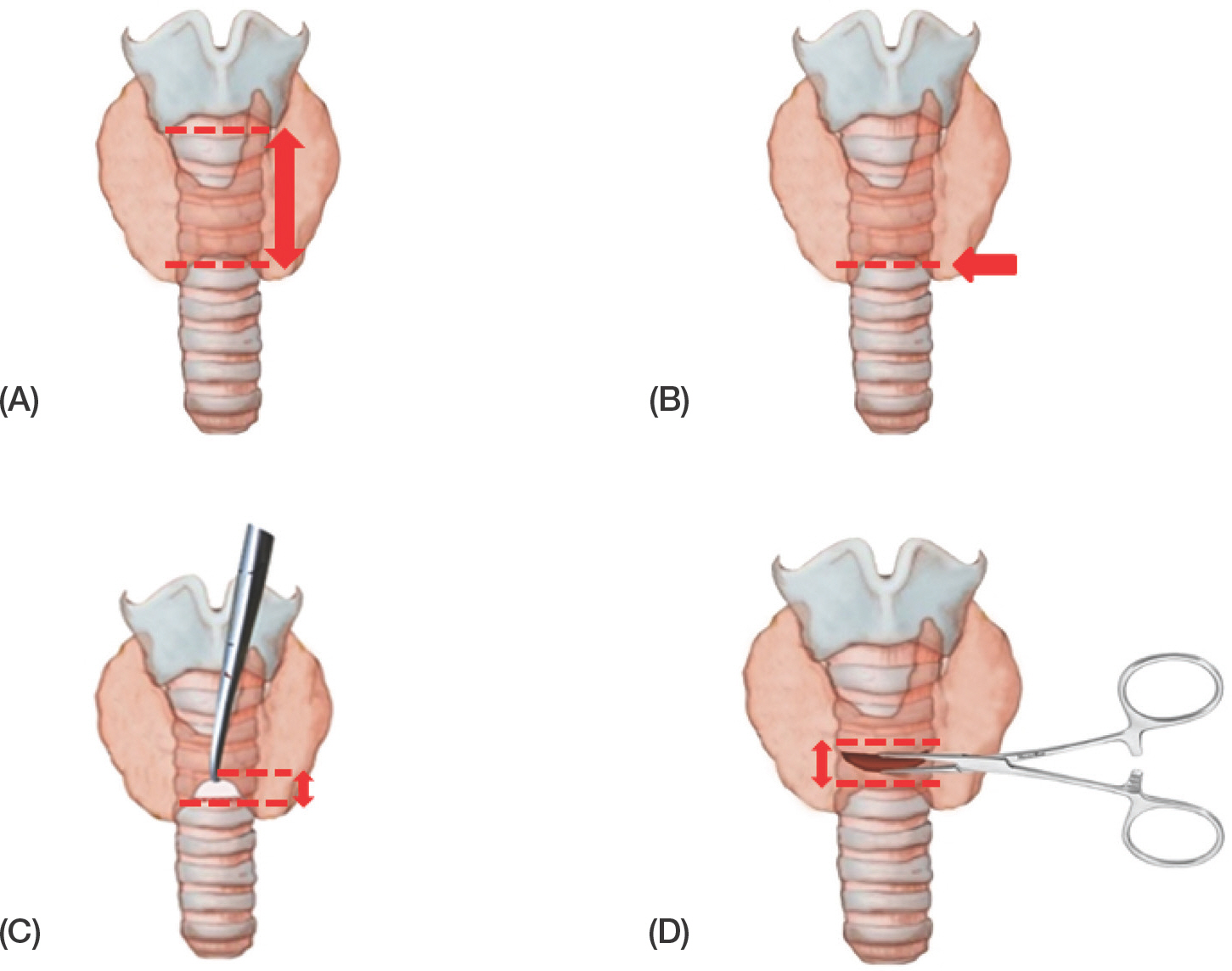
Fig. 1. Schematic illustration of variables used in this study. Figure shows distance between cricoid cartilage to the lower margin of thyroid isthmus (A), the level of thyroid isthmus lower margin compared with tracheal ring number (B, dotted line), movability of thyroid istchmus (C), maximal widened distance between the lower margin of upper tracheal cartilage and the upper margin of lower tracheal cartilage (D).

Fig. 2. Schematic illustration of Minimally invasive horizontal intercartilaginous incision technique. The skin incision is made 2 cm below the center of the cricoid cartilage to exposure the inferior border of thyroid isthmus (A). The inferior border of thyroid isthmus is identified and retracted upward to expose the 2nd and the 3rd tracheal ring or the 3rd and the 4th tracheal ring (B). The annular ligament between the 2nd and the 3rd tracheal ring or the the 3rd and the 4th tracheal ring is identified, and an intercartilaginous incision was made.
Reference
-
References
1. Walts PA, Murthy SC, DeCamp MM. Techniques of surgical tracheostomy. Clin Chest Med. 2003; 24:413–22.
Article2. Cheung NH, Napolitano LM. Tracheostomy: Epidemiology, Indications, Timing, Technique, and Outcomes Discussion. Respir Care. 2014; 59:895–919.3. Heffner JE, Miller KS, Sahn SA. Tracheostomy in the intensive care unit. Part 2: Complications. Chest. 1986; 90:430–6.4. Scurry WC, McGinn JD. Operative tracheotomy. Oper Tech Otolaryngol. 2007; 18:85–9.
Article5. Mendez-Picon G, Ehrlich FE, Salzberg AM. The effect of tracheostomy incisions on tracheal growth. J Pediatr Surg. 1976; 11:681–5.
Article6. Lulenski GC, Batsakis JG. Tracheal incision as a contributing factor to tracheal stenosis: an experimental study. Ann Otol Rhinol Laryngol. 1975; 84:781–6.
Article7. Probst G, Dubiel S, Deitmer T. The cartilage conserving concept of surgical tracheostomy. Laryngorhinootologie. 2004; 83:461–5.8. Song JJ, Choi IJ, Chang H, Kim DW, Chang HW, Park GH, et al. Pediatric tracheostomy revisited: A nine-year experience using horizontal intercartilaginous incision. Laryngoscope. 2015; 125:485–92.
Article9. Kato I, Uesugi K, Kikuchihara M, Iwasawa H, Iida J, Tsutsumi K, et al. Tracheostomy –The horizontal tracheal incision. J Laryngol Otol. 1990; 104:322–5.10. Kamel KS, Lau G, Stringer MD. In vivo and in vitro morphometry of the human trachea. Clin Anat. 2009; 22:571–9.
Article11. WON HS, HAN CS, Oh CS, Chung IH, Won HJ, Kim JH. The location and morphometry of the thyroid isthmus in adult Korean cadavers. Anatomical science international. 2013; 88:212–6.
Article12. Kim IS, Lim JM, Chai OH, Han EH, Kim HT, Song CH. Morphometric Study of the Trachea in Korean. Korean J Phys Anthrop. 2015; 28:185–95.
Article13. Moore KL, Dalley AF, Agur AMR. Clinically oriented anatomy. 7th ed.Lippincott Williams & Wilkins;Philadel-phia: 2014.14. Anson BJ. Morris'human anatomy. 12th edn.McGraw-Hill book Co, New York;1996.15. Clemente CD. Anatomy of the human body. 30th edn.Lea & Febiger, Philadelphia;1985.16. Gardner E, Gray DJ, O'Rahilly R. Anatomy, a regional study of human structure. W.B. Saunders Company, Philadelphia;1960.17. Moore KL, Dalley AF, Agur AMR. Clinically oriented anatomy. 7th ed.Lippincott Williams & Wilkins, Philadel-phia;2014. p. 1018. p.18. Moore KL, Dalley AF, Agur AMR. Clinically oriented anatomy. 7th ed.Lippincott Williams & Wilkins, Philadel-phia;2014. p. 1045. p.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Percutaneous Dilatational Tracheostomy
- Mitral Valve Replacement by Minimally Invasive Right Parasternal Incision: A Case Report
- A New Beginning for the Journal of Minimally Invasive Surgery for the International Recognition and Contribution of Scientific Development of Minimally Invasive Surgery
- Minimally Invasive Aortic Valve Surgery: A Report of Two Cases
- Minimal Invasive Translaryngeal Tracheostomy after Open Heart Surgery
