Pulmonary Artery Intimal Sarcoma versus Pulmonary Artery Thromboembolism: CT and Clinical Findings
- Affiliations
-
- 1Department of Radiology and the Research Institute of Radiology, University of Ulsan College of Medicine, Asan Medical Center, Seoul 05505, Korea. mimowdr@amc.seoul.kr
- 2Department of Radiology, Korea University Ansan Hospital, Korea University College of Medicine, Ansan 15355, Korea.
- 3Department of Pathology, University of Ulsan College of Medicine, Asan Medical Center, Seoul 05505, Korea.
- 4Department of Healthcare Management, Cheongju University, Cheongju 28503, Korea.
- KMID: 2413709
- DOI: http://doi.org/10.3348/kjr.2018.19.4.792
Abstract
OBJECTIVE
To describe CT and clinical findings of pulmonary artery intimal sarcoma (PAIS) compared with those of pulmonary thromboembolism (PTE), to investigate MRI and positron emission tomography (PET)-CT findings of PAIS, and to evaluate the effect of delayed diagnosis of PAIS on survival outcomes.
MATERIALS AND METHODS
Twenty-six patients with PAIS were retrospectively identified and matched for sex, with patients with PTE at a ratio of 1:2. CT and clinical findings of the two groups were compared using Student's t test or chi-square test. The effect of delayed diagnosis on survival was investigated using Kaplan-Meier analysis.
RESULTS
The most common tumor pattern in PAIS was tumoral impaction. Heterogeneous attenuation, wall eclipse signs, intratumoral vessels, acute interphase angles, single location, presence of lung ischemia, and central location were significantly more common in PAIS than in PTE (all p < 0.01). Levels of D-dimers and brain natriuretic peptide were lower in PAIS than in PTE (p < 0.05). In three patients of PAIS, long inversion time sequence MRI showed intermingled dark signal intensity foci suggestive of intermingled thrombi. All nine patients who had undergone PET-CT displayed hypermetabolism. Diagnosis was delayed in 42.3% of the PAIS patients and those patients had a significantly shorter overall survival than patients whose diagnosis was not delayed (p < 0.05).
CONCLUSION
The characteristic CT and clinical findings of PAIS may help achieve early diagnosis of PAIS and make better survival outcomes of patients. MRI and PET-CT can be used as second-line imaging modalities and could help distinguish PAIS from PTE and to plan clinical management.
Keyword
MeSH Terms
Figure
-
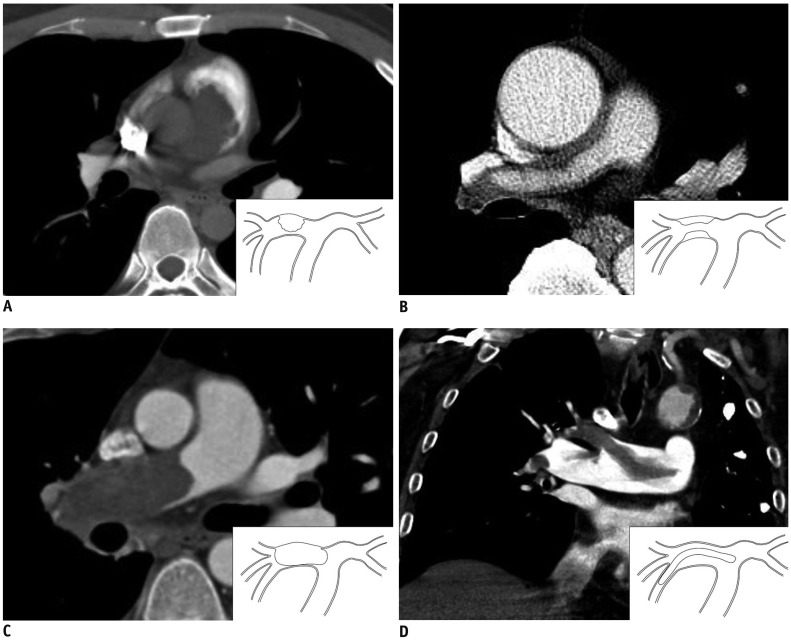
Fig. 1 Tumor extension patterns of CT in four patients (all 5-mm thick).A. Pattern I: cauliflower-like polypoid lesion. B. Pattern II: diffuse/focal wall thickening. C. Pattern III: tumoral impaction. D. Pattern IV: tubular-polypoid shape.
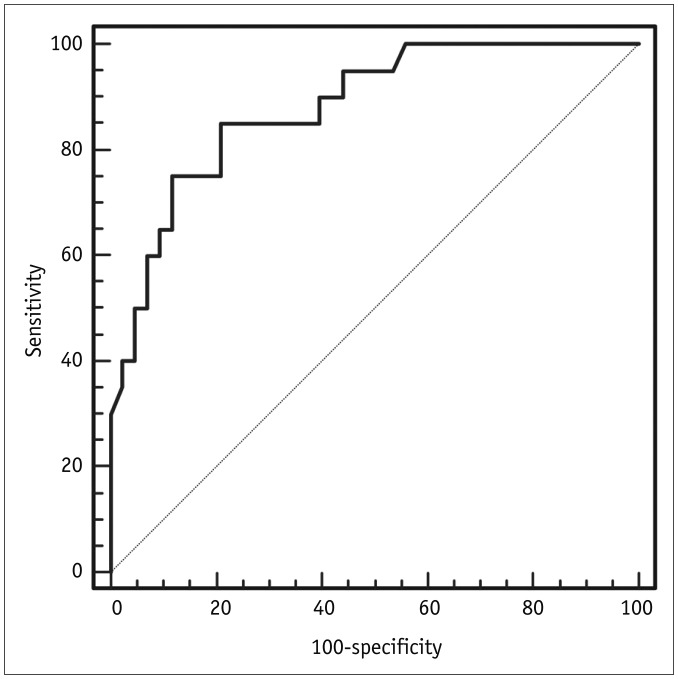
Fig. 2 ROC curve showing the D-dimer level predicting PAIS.Areas under ROC curve of D-dimers was 0.88 (95% confidence interval, 0.774–0.948). PAIS = pulmonary artery intimal sarcoma, ROC = receiver operating characteristic

Fig. 3 MR images obtained in 36-year-old male patient with PAIS (same patient as in Fig. 1A).A. T2-weighted axial image obtained at pulmonary trunk level. On MR image, index lesion has lobulated contour and high SI compared with pectoralis muscle. B. In late gadolinium enhancement image using inversion time of 600 msec (TI 600), lesion has intermingled dark SI, which reflects intermingled thrombosis (arrows). MR = magenetic resonance, SI = signal intensity

Fig. 4 FDG positron emission tomography-CT image obtained from 24-year-old patient with PAIS (same patient in Fig. 1C).Surgical resection was performed.A. Axial image shows high FDG uptake in right pulmonary artery (maxSUV: 12.9). B. Focal hemorrhage in mass of gross specimen (arrow); this is common in PAIS (arrow). High magnification elastic Van-Gieson-stained specimen (inset, × 100) shows mass of intimal origin detached from intimal layer (arrowheads). FDG = fluorodeoxyglucose
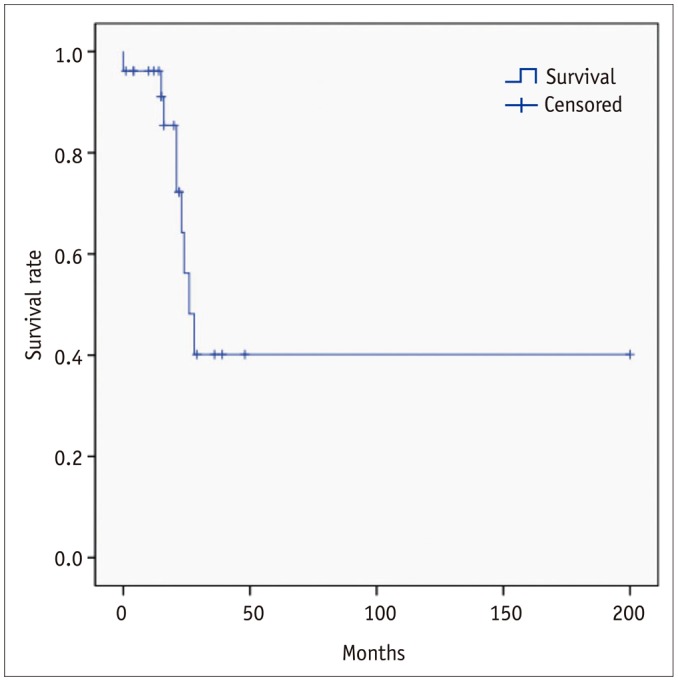
Fig. 5 Overall survival analyzed by Kaplan-Meier method.Median overall survival of patient with PAIS was 26 months (range, 0–200 months).
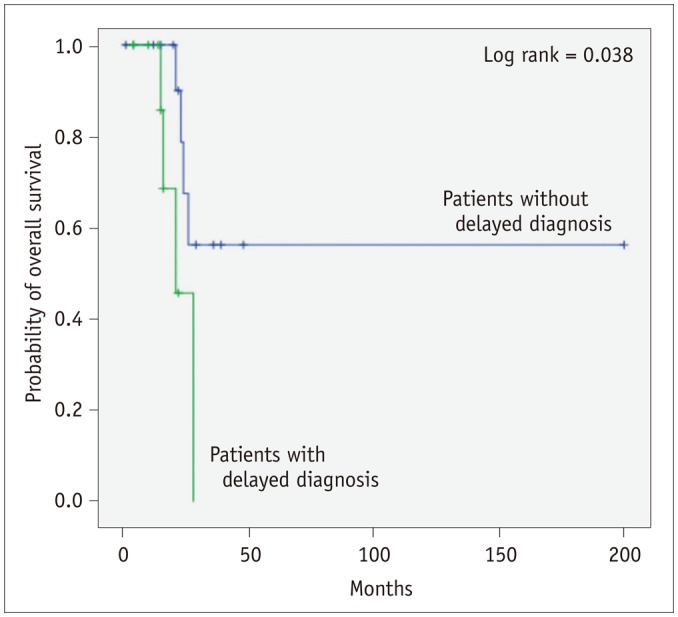
Fig. 6 Kaplan-Meier survival curve showing overall survival of patients with and without delayed diagnosis.Overall survival of patients with delayed diagnosis was shorter than that of patients with timely diagnosis, if initial patients who died due to immediate post-operative complication (< 7 days) were excluded (mean survival, 22.5 ± 2.6 vs. 122.0 ± 29.1 months, p = 0.038).
Reference
-
1. Travis WD, Brambilla E, Burke AP, Marx A, Nicholson AG. WHO classification of tumours of the lung, pleura, thymus and heart. 4th ed. Lyon: World Health Organization;2015. p. 128–129.2. Anderson MB, Kriett JM, Kapelanski DP, Tarazi R, Jamieson SW. Primary pulmonary artery sarcoma: a report of six cases. Ann Thorac Surg. 1995; 59:1487–1490. PMID: 7771829.
Article3. Bernard J, Yi ES. Pulmonary thromboendarterectomy: a clinicopathologic study of 200 consecutive pulmonary thromboendarterectomy cases in one institution. Hum Pathol. 2007; 38:871–877. PMID: 17350667.
Article4. Mussot S, Ghigna MR, Mercier O, Fabre D, Fadel E, Le Cesne A, et al. Retrospective institutional study of 31 patients treated for pulmonary artery sarcoma. Eur J Cardiothorac Surg. 2013; 43:787–793. PMID: 22843511.
Article5. Yi CA, Lee KS, Choe YH, Han D, Kwon OJ, Kim S. Computed tomography in pulmonary artery sarcoma: distinguishing features from pulmonary embolic disease. J Comput Assist Tomogr. 2004; 28:34–39. PMID: 14716229.6. Gan HL, Zhang JQ, Huang XY, Yu W. The wall eclipsing sign on pulmonary artery computed tomography angiography is pathognomonic for pulmonary artery sarcoma. PLoS One. 2013; 8:e83200. PMID: 24391746.
Article7. Chang S, Hur J, Im DJ, Suh YJ, Hong YJ, Lee HJ, et al. Dual-energy CT-based iodine quantification for differentiating pulmonary artery sarcoma from pulmonary thromboembolism: a pilot study. Eur Radiol. 2016; 26:3162–3170. PMID: 26638163.
Article8. Blackmon SH, Rice DC, Correa AM, Mehran R, Putnam JB, Smythe WR, et al. Management of primary pulmonary artery sarcomas. Ann Thorac Surg. 2009; 87:977–984. PMID: 19231448.
Article9. Weinsaft JW, Kim HW, Crowley AL, Klem I, Shenoy C, Van Assche L, et al. LV thrombus detection by routine echocardiography: insights into performance characteristics using delayed enhancement CMR. JACC Cardiovasc Imaging. 2011; 4:702–712. PMID: 21757159.10. Weinsaft JW, Kim HW, Shah DJ, Klem I, Crowley AL, Brosnan R, et al. Detection of left ventricular thrombus by delayed-enhancement cardiovascular magnetic resonance prevalence and markers in patients with systolic dysfunction. J Am Coll Cardiol. 2008; 52:148–157. PMID: 18598895.11. Mollet NR, Dymarkowski S, Volders W, Wathiong J, Herbots L, Rademakers FE, et al. Visualization of ventricular thrombi with contrast-enhanced magnetic resonance imaging in patients with ischemic heart disease. Circulation. 2002; 106:2873–2876. PMID: 12460863.
Article12. Grosse C, Grosse A. CT findings in diseases associated with pulmonary hypertension: a current review. Radiographics. 2010; 30:1753–1777. PMID: 21057119.
Article13. Blackmon SH, Reardon MJ. Pulmonary artery sarcoma. Methodist Debakey Cardiovasc J. 2010; 6:38–43.
Article14. Cox JE, Chiles C, Aquino SL, Savage P, Oaks T. Pulmonary artery sarcomas: a review of clinical and radiologic features. J Comput Assist Tomogr. 1997; 21:750–755. PMID: 9294569.
Article15. Rafal RB, Nichols JN, Markisz JA. Pulmonary artery sarcoma: diagnosis and postoperative follow-up with gadolinium-diethylenetriamine pentaacetic acid-enhanced magnetic resonance imaging. Mayo Clin Proc. 1995; 70:173–176. PMID: 7845042.
Article16. Weinreb JC, Davis SD, Berkmen YM, Isom W, Naidich DP. Pulmonary artery sarcoma: evaluation using Gd-DTPA. J Comput Assist Tomogr. 1990; 14:647–649. PMID: 2370363.17. Smith WS, Lesar MS, Travis WD, Lubbers P, Sen RP, Ginsberg AM, et al. MR and CT findings in pulmonary artery sarcoma. J Comput Assist Tomogr. 1989; 13:906–909. PMID: 2778152.
Article18. Kanjanauthai S, Kanluen T, Ray C. Pulmonary artery sarcoma masquerading as saddle pulmonary embolism. Heart Lung Circ. 2008; 17:417–419. PMID: 17913581.
Article19. Liu M, Luo C, Wang Y, Guo X, Ma Z, Yang Y, et al. Multiparametric MRI in differentiating pulmonary artery sarcoma and pulmonary thromboembolism: a preliminary experience. Diagn Interv Radiol. 2017; 23:15–21. PMID: 27919861.
Article20. Nijjar PS, Iqbal FM, Alraies MC, Valeti US, Tadavarthy SM. Primary pulmonary artery sarcoma masquerading as pulmonary embolism: role of cardiac MRI. Eur Heart J. 2016; 37:1479. PMID: 26787435.
Article21. Sun J, Tang H, Lu C, Chen Y. Syncope caused by pulmonary artery intima sarcoma: a cardiac magnetic resonance imaging-based differentiating diagnosis. Eur J Cardiothorac Surg. 2014; 46:503. PMID: 24477742.
Article22. Renilla A, Fernández-Vega I, Martín M, Weinsaft JW. Pulmonary artery sarcoma mimicking a pulmonary embolism. Eur Heart J Cardiovasc Imaging. 2013; 14:1025. PMID: 23604911.
Article23. Kriz JP, Munfakh NA, King GS, Carden JO. Pulmonary srtery intimal sarcoma: a case report. Case Rep Oncol. 2016; 9:267–272. PMID: 27239183.24. Attinà D, Niro F, Tchouanté P, Mineo G, Russo V, Palazzini M, et al. Pulmonary artery intimal sarcoma. Problems in the differential diagnosis. Radiol Med. 2013; 118:1259–1268. PMID: 23801391.
Article25. Lee DH, Jung TE, Lee JH, Shin DG, Park WJ, Choi JH. Pulmonary artery intimal sarcoma: poor 18F-fluorodeoxyglucose uptake in positron emission computed tomography. J Cardiothorac Surg. 2013; 8:40. PMID: 23497592.
Article26. Watanabe K, Shinkai M, Kaneko T. Autopsy case of pulmonary artery sarcoma forming aneurysm without FDG uptake. Arch Bronconeumol. 2016; 52:535–536. PMID: 27242246.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Pulmonary Artery Intimal Sarcoma Involving the Peripheral Pulmonary Artery, Initially Misdiagnosed as Pulmonary Artery Thromboembolism and Vasculitis: A Case Report
- Differential Imaging Features of Pulmonary Artery Dissection from Other Intraluminal Diseases of Pulmonary Artery: Two Cases Report
- A Case of Pulmonary Artery Intimal Sarcoma Diagnosed with Multislice CT Scan with 3D Reconstruction
- Primary Intimal Sarcoma Originating from Pulmonary Valve
- Surgical Treatment of Pulmonary Artery Sarcoma: One case report
