Secondary Tumors of the Urinary System: An Imaging Conundrum
- Affiliations
-
- 1Department of Radiology, Hacettepe University, School of Medicine, Ankara 06230, Turkey. ruhionur@yahoo.com
- KMID: 2413703
- DOI: http://doi.org/10.3348/kjr.2018.19.4.742
Abstract
- Imaging features of metastases to the urinary system may closely mimic primary urinary tract tumors, and differential diagnosis by imaging alone may be problematic or even impossible in some cases. The main purpose of this article was to familiarize radiologists with imaging findings of metastasis to the urinary system on cross-sectional imaging, with an emphasis on abdominal and pelvic computed tomography and magnetic resonance imaging. In addition, we review the clinical importance and implications of metastases to the urinary tract and provide information on diagnostic work-ups.
Keyword
- Urinary system; Metastasis; Kidney; Ureter; Bladder; Urethra; CT; MRI
MeSH Terms
Figure
-

Fig. 1 75-year-old female patient with known breast cancer with recently detected pulmonary and bone metastases was referred for restaging after chemotherapy. A. Gray-scale US image demonstrates mildly hyperechoic mass (arrows) in lower pole of left kidney. Lesion is hardly discernible from background renal parenchyma on US image. B, C. Axial and coronal contrast-enhanced CT images reveal infiltrative-type hypodense solid mass (arrows) with relatively less enhancement as compared to background renal parenchyma. CT = computed tomography, US = ultrasonography
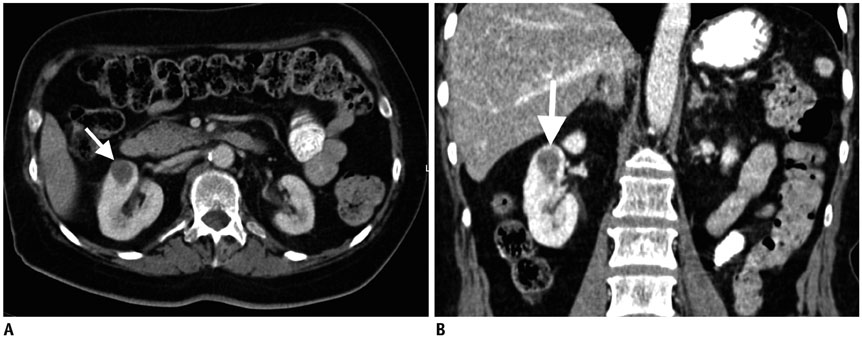
Fig. 2 65-year-old female with known lung cancer and brain metastasis. Post-contrast axial (A) and coronal (B) CT images show hypodense, endophytic solid lesion (arrows) in upper pole of right kidney. Biopsy confirmed metastatic nature of this mass.
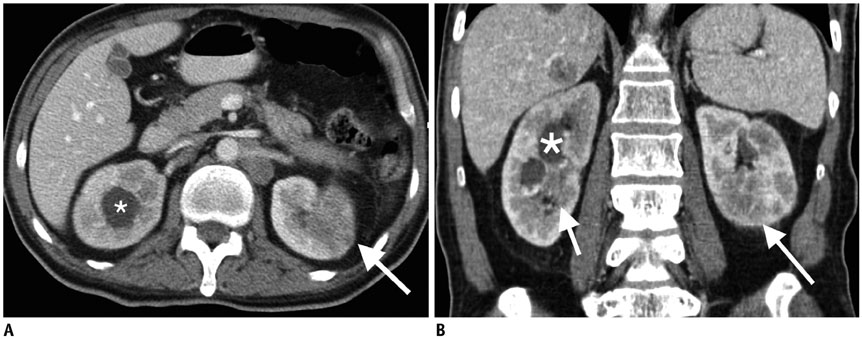
Fig. 3 53-year-old male patient with known stage 4 lung cancer. Brain and liver metastases were previously detected. Axial (A) and coronal (B) contrast-enhanced CT images demonstrate hydronephrosis (*) in right kidney due to centrally located hypovascular mass (short arrow). Also note diffusely infiltrative mass (long arrows) in lower pole of left kidney parenchyma. Biopsy confirmed metastatic nature of centrally located right kidney mass.

Fig. 4 66-year-old male patient with known lung cancer and chest wall invasion. No distant metastasis was known at time of this CT scan. Axial (A) and coronal (B) contrast-enhanced CT images reveal low-attenuating, exophytic mass (arrows) that was histopathologically proven to be metastasis from lung carcinoma.

Fig. 5 74-year-old female patient with known lung cancer and metastatic involvement of left iliac bone. Patient was in clinical remission for two years after last treatment. A. Axial fat-saturated T2WI reveals hypointense, focal parenchymal mass (arrow) in subcortical part of right kidney. B. Corresponding DWI sequence image shows intense diffuse restriction at location of mass (arrow). Patient refused percutaneous biopsy at that point, and she was placed on close imaging surveillance. C. Axial fat-saturated T2WI obtained 3 months after first scan revealed interval enlargement of lesion (arrow). D. Corresponding DWI clearly demonstrates focally increased signal suggestive of diffusion restriction (arrow). Percutaneous biopsy confirmed metastatic nature of this lesion. E. Apparent diffusion coefficient map confirms true diffusion restriction by demonstrating significant hypointensity at site of lesion (arrow). DWI = diffusion-weighted imaging, T2WI = T2-weighted image
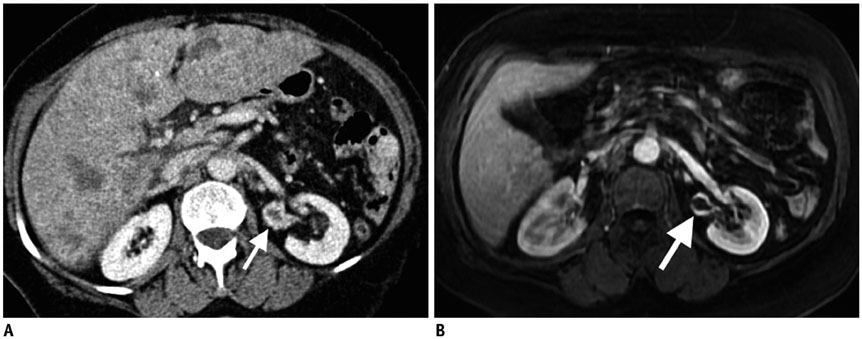
Fig. 6 64-year-old female with known breast cancer and multiple metastases in liver. A. Axial contrast-enhanced CT reveals nodular wall thickening in left renal pelvis (arrow) with intense contrast enhancement. Also note multiple metastases in liver. B. Axial post-contrast T1-weighted image also demonstrates abnormal irregular wall thickening (arrow) with associated brisk contrast enhancement. Urine cytology confirmed uroepithelial metastasis.
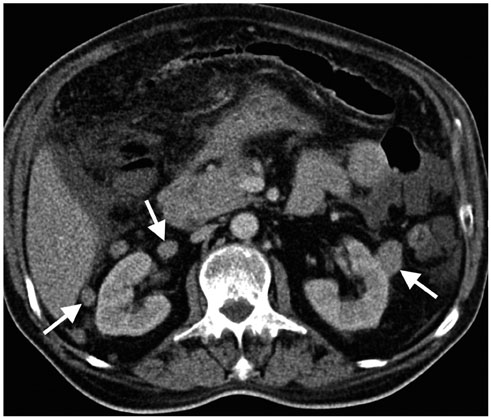
Fig. 7 65-year-old male with known lung cancer with widespread solid organ and peritoneal involvement in abdomen. Axial contrast-enhanced CT shows bilateral numerous perirenal solid masses (arrows), more prominent on right, consistent with metastases.
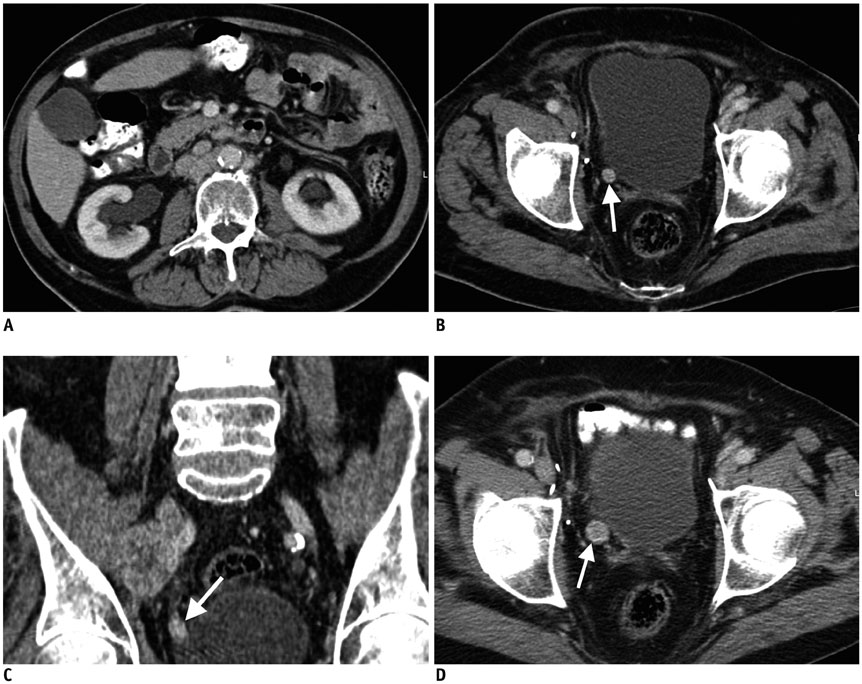
Fig. 8 55-year-old female patient with known gastric cancer and vertebral metastases presenting with right flank pain. A. Axial contrast-enhanced CT demonstrates newly developed pelvicalyceal dilatation in right kidney. Axial (B) and coronally reformatted (C) CT images demonstrate nodular contrast enhancement in lower third of right ureter (arrows). D. Axial contrast-enhanced CT image demonstrated interval enlargement of same lesion (arrow) 4 weeks after index CT and endo-urological biopsy confirmed gastric cancer as primary source.

Fig. 9 64-year-old female with known breast cancer who was in clinical remission for last 5 years. She was referred for annual follow-up CT and was asymptomatic at time of scan. A. Axial venous phase scan demonstrates moderate-severe hydroureteronephrosis (arrow), with significant loss of renal parenchyma, on left kidney. B. Axial venous phase scan demonstrates faint enhancement of lower left ureter (arrow). This was transition point of left dilated ureter. C. Enhancement becomes more pronounced on urographic phase image (arrow). Endo-urologic biopsy confirmed non-neoplastic cells but amyloid deposit.
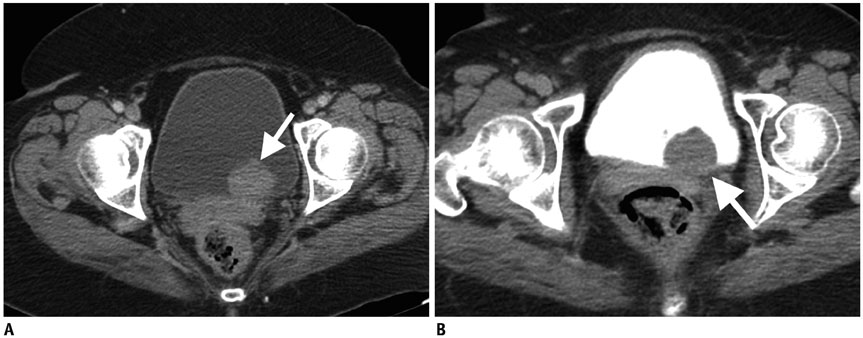
Fig. 10 61-year-old female with known RCC and retroperitoneal lymph node metastases presenting with hematuria. A. Axial contrast-enhanced CT image demonstrates polypoid lesion located close to left ureteral orifice (arrow). There was no evidence of hydronephrosis in left kidney on upper level images (not shown). B. Axial urographic phase image clearly shows filling defect (arrow) created by same polypoid lesion. Cystoscopic biopsy confirmed metastatic RCC. RCC = renal cell cancer
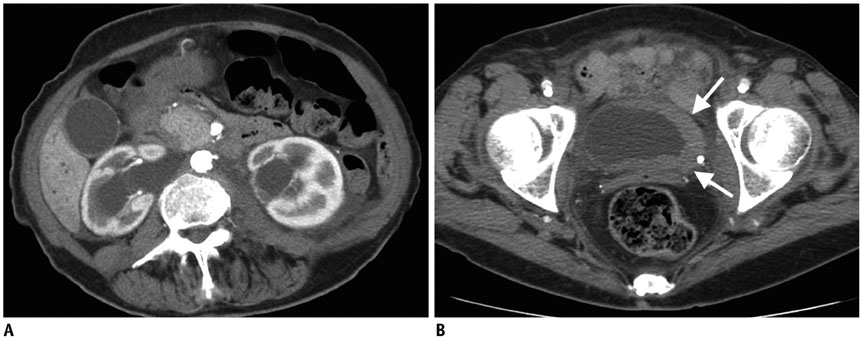
Fig. 11 Bladder metastasis in 74-year-old female with known breast cancer, which was last treated 10 years ago; she was in clinical and imaging remission since then. She recently presented with polyuria and gross hematuria. A. Bilateral dilatation of renal collecting system is seen on axial contrast-enhanced CT image. B. Axial contrast-enhanced CT image demonstrates asymmetric thickening (arrows) in left lateral wall of bladder. Chest CT was also negative. Cystoscopic biopsy confirmed metastatic breast cancer.

Fig. 12 Urethral metastasis in 57-year-old male with known neuroendocrine tumor of bladder and no known metastasis elsewhere. A. Axial urographic phase CT image shows asymmetric wall thickening (arrows) in anterior bladder wall. Cystoscopic biopsy revealed neuroendocrine tumor of bladder. B. Axial post-contrast CT image of same patient, who presented with difficult urination. CT image demonstrates extensive tumor infiltration (arrow) in penile shaft and ureter (also note urinary drainage catheter-*). Endo-urologic biopsy confirmed metastatic neuroendocrine tumor.
Reference
-
1. Arvind NK, Singh O, Gupta S, Ali Q. Ureteral metastasis as the presenting manifestation of pancreatic carcinoma. Rev Urol. 2013; 15:124–130.2. Doo SW, Kim WB, Kim BK, Yang WJ, Yoon JH, Jin SY, et al. Metastasis of renal cell carcinoma to the bladder. Korean J Urol. 2013; 54:69–72.
Article3. Zhou C, Urbauer DL, Fellman BM, Tamboli P, Zhang M, Matin SF, et al. Metastases to the kidney: a comprehensive analysis of 151 patients from a tertiary referral centre. BJU Int. 2016; 117:775–782.
Article4. Abrams HL, Spiro R, Goldstein N. Metastases in carcinoma; analysis of 1000 autopsied cases. Cancer. 1950; 3:74–85.5. Bracken RB, Chica G, Johnson DE, Luna M. Secondary renal neoplasms: an autopsy study. South Med J. 1979; 72:806–807.6. Bates AW, Baithun SI. The significance of secondary neoplasms of the urinary and male genital tract. Virchows Arch. 2002; 440:640–647.
Article7. Patel U, Ramachandran N, Halls J, Parthipun A, Slide C. Synchronous renal masses in patients with a nonrenal malignancy: incidence of metastasis to the kidney versus primary renal neoplasia and differentiating features on CT. AJR Am J Roentgenol. 2011; 197:W680–W686.
Article8. Choyke PL, White EM, Zeman RK, Jaffe MH, Clark LR. Renal metastases: clinicopathologic and radiologic correlation. Radiology. 1987; 162:359–363.
Article9. Prasad SR, Dalrymple NC, Surabhi VR. Cross-sectional imaging evaluation of renal masses. Radiol Clin North Am. 2008; 46:95–111. vi–vii.
Article10. Sánchez-Ortiz RF, Madsen LT, Bermejo CE, Wen S, Shen Y, Swanson DA, et al. A renal mass in the setting of a nonrenal malignancy: when is a renal tumor biopsy appropriate? Cancer. 2004; 101:2195–2201.11. Adamy A, Von Bodman C, Ghoneim T, Favaretto RL, Bernstein M, Russo P. Solitary, isolated metastatic disease to the kidney: Memorial Sloan-Kettering Cancer Center experience. BJU Int. 2011; 108:338–342.
Article12. Olsson CA, Moyer JD, Laferte RO. Pulmonary cancer metastatic to the kidney--a common renal neoplasm. J Urol. 1971; 105:492–496.
Article13. Klinger ME. Secondary tumors of the genito-urinary tract. J Urol. 1951; 65:144–153.
Article14. Mitnick JS, Bosniak MA, Rothberg M, Megibow AJ, Raghavendra BN, Subramanyam BR. Metastatic neoplasm to the kidney studied by computed tomography and sonography. J Comput Assist Tomogr. 1985; 9:43–49.
Article15. Bailey JE, Roubidoux MA, Dunnick NR. Secondary renal neoplasms. Abdom Imaging. 1998; 23:266–274.
Article16. Bhatt GM, Bernardino ME, Graham SD Jr. CT diagnosis of renal metastases. J Comput Assist Tomogr. 1983; 7:1032–1034.
Article17. Vikram R, Beland MD, Blaufox MD, Moreno CC, Gore JL, Harvin HJ, et al. ACR appropriateness criteria renal cell carcinoma staging. J Am Coll Radiol. 2016; 13:518–525.
Article18. Sun MR, Pedrosa I. Magnetic resonance imaging of renal masses. Semin Ultrasound CT MR. 2009; 30:326–351.
Article19. Ferrozzi F, Bova D, Campodonico F. Computed tomography of renal metastases. Semin Ultrasound CT MR. 1997; 18:115–121.
Article20. Maurer MH, Härmä KH, Thoeny H. Diffusion-weighted genitourinary imaging. Radiol Clin North Am. 2017; 55:393–411.
Article21. Thoeny HC, De Keyzer F, Oyen RH, Peeters RR. Diffusion-weighted MR imaging of kidneys in healthy volunteers and patients with parenchymal diseases: initial experience. Radiology. 2005; 235:911–917.
Article22. Heller MT, Haarer KA, Thomas E, Thaete FL. Neoplastic and proliferative disorders of the perinephric space. Clin Radiol. 2012; 67:e31–e41.
Article23. Surabhi VR, Menias C, Prasad SR, Patel AH, Nagar A, Dalrymple NC. Neoplastic and non-neoplastic proliferative disorders of the perirenal space: cross-sectional imaging findings. Radiographics. 2008; 28:1005–1017.
Article24. Grützner G, Jungblut RM. [Perirenal metastasis of a malignant melanoma in a young child]. Aktuelle Radiol. 1993; 3:372–374.25. Wilbur AC, Turk JN, Capek V. Perirenal metastases from lung cancer: CT diagnosis. J Comput Assist Tomogr. 1992; 16:589–591.26. Gore RM, Balfe DM, Aizenstein RI, Silverman PM. The great escape: interfascial decompression planes of the retroperitoneum. AJR Am J Roentgenol. 2000; 175:363–370.27. Koutani A, Lechevallier E, André M, de Fromont M, Coulange C. [Contralateral perirenal metastasis of renal adenocarcinoma]. Prog Urol. 1997; 7:1002–1003.28. Nikolaos F, Panagiotis A, Konstantinos B, Vassilios S, Iraklis P. Distant ureteral metastasis from colon adenocarcinoma: report of a case and review of the literature. Case Rep Urol. 2014; 2014:196425.
Article29. Katsuno G, Kagawa S, Kokudo Y, Muraoka A, Tatemoto A, Sone Y, et al. Ureteral metastasis from appendiceal cancer: report of a case. Surg Today. 2005; 35:168–171.
Article30. Roy S, Baijal SS. Pancreatic adenocarcinoma presenting with ureteric metastases. Case report and review of literature. Clin Imaging. 1993; 17:99–103.
Article31. Haddad FS. Metastases to the ureter. Review of the world literature, and three new case reports. J Med Liban. 1999; 47:265–271.32. Stow B. IX. Fibrolymphosarcomata of both ureters metastatic to a primary lymphosarcomata of the anterior mediastinum of thymus origin. Ann Surg. 1909; 50:901–906.33. Maclean JT, Fowler VB. Pathology of tumors of the renal pelvis and ureter. J Urol. 1956; 75:384–415.
Article34. Presman D, Ehrlich L. Metastatic tumors of the ureter. J Urol. 1948; 59:312–325.
Article35. Cohen WM, Freed SZ, Hasson J. Metastatic cancer to the ureter: a review of the literature and case presentations. J Urol. 1974; 112:188–189.
Article36. Winalski CS, Lipman JC, Tumeh SS. Ureteral neoplasms. Radiographics. 1990; 10:271–283.
Article37. Fitch WP, Robinson JR, Radwin HW. Metastatic carcinoma of the ureter. Arch Surg. 1976; 111:874–876.
Article38. Marincek B, Scheidegger JR, Studer UE, Kraft R. Metastatic disease of the ureter: patterns of tumoral spread and radiologic findings. Abdom Imaging. 1993; 18:88–94.
Article39. Gelister JS, Falzon M, Crawford R, Chapple CR, Hendry WF. Urinary tract metastasis from renal carcinoma. Br J Urol. 1992; 69:250–252.
Article40. Morichetti D, Mazzucchelli R, Lopez-Beltran A, Cheng L, Scarpelli M, Kirkali Z, et al. Secondary neoplasms of the urinary system and male genital organs. BJU Int. 2009; 104:770–776.
Article41. Ramsey J, Beckman EN, Winters JC. Breast cancer metastatic to the urinary bladder. Ochsner J. 2008; 8:208–212.42. Kazama S, Kitayama J, Sunami E, Niimi A, Nomiya A, Homma Y, et al. Urethral metastasis from a sigmoid colon carcinoma: a quite rare case report and review of the literature. BMC Surg. 2014; 14:31.
Article43. Cheng CW, Wong WS, Chan LW, Lai FM. A rare cause of acute urinary retention: urethral metastasis from renal cell carcinoma. Int Urol Nephrol. 2004; 36:145–147.
Article44. Bhagavatula SK, Shyn PB. Image-guided renal interventions. Radiol Clin North Am. 2017; 55:359–371.
Article45. Rybicki FJ, Shu KM, Cibas ES, Fielding JR, vanSonnenberg E, Silverman SG. Percutaneous biopsy of renal masses: sensitivity and negative predictive value stratified by clinical setting and size of masses. AJR Am J Roentgenol. 2003; 180:1281–1287.
Article46. Butros SR, McCarthy CJ, Karaosmanoğlu AD, Shenoy-Bhangle AS, Arellano RS. Feasibility and effectiveness of image-guided percutaneous biopsy of the urinary bladder. Abdom Imaging. 2015; 40:1838–1842.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Characteristics of Multiple Primary Malignant Neoplasms Associated with the Urinary Tract Malignancy
- Radionuclide Imaging on Urinary Tract Obstruction
- The A.B.O. Blood Groups in Tumors of the Genitourinary Tract Among Korean
- Diagnostic Conundrum: Fever and Pyuria Preceding Diagnosis of Kawasaki Disease in Children
- Clinical Observation on Tumors of the Genito-urinary Tract
