Acetabular Cup Revision Arthroplasty Using Morselized Impaction Allograft
- Affiliations
-
- 1Department of Orthopaedic Surgery, CHA Bundang Medical Center, CHA University, Seongnam, Korea. drjmlee@naver.com
- KMID: 2412687
- DOI: http://doi.org/10.5371/hp.2018.30.2.65
Abstract
- The rate of acetabular cup revision arthroplasty is gradually rising along with an increased risk of osteolysis and prosthesis loosening over time and an increase in life expectancy. The goals of revision total hip arthroplasty are: i) implant stability through reconstruction of large bone defects, ii) restoration of range of motion and biomechanics of the hip joint, and iii) normalization of uneven limb lengths. In acetabular cup revision arthroplasty, stable fixation of acetabular components is difficult in the presence of severe bone loss (e.g., evidence suggests that it is challenging to achieve satisfactory results in cases of Paprosky type 3 or higher bone defects using conventional techniques). The author of this study performed acetabular revision to manage patients with large areas of defective bones by filling in with morselized impaction allografts. These allografts were irradiated frozen-stored femoral heads acquired from a tissue bank, and were applied to areas of an acetabular bone defect followed by insertion of a cementless cup. When this procedure was insufficient to obtain primary fixation, a tri-cortical or structural allograft using a femoral head was carried out. Structural stability and bone incorporation were confirmed via long-term follow-up. This study aims to review conventional surgical techniques and verify the utility of surgical procedures by analyzing the author's surgical methods and discussing case reports.
Keyword
MeSH Terms
Figure
-

Fig. 1 (A) Morselized allografts are made by removing roughly 1 cm from the head of a femur with bone scissors following by cleansing (using pulsatile lavage) and drying. Dried morselized impaction allografts are next mixed with a patient's blood. (B) Preoperative anteroposterior view of a 58-year-old male patient with a bony defect (Paprosky type 2C) and aseptic loosening after total hip arthroplasty (THA). (C) Immediate postoperative anteroposterior view showing revision THA with a morselized impacted allograft. (D) Two years after operation, we performed greater trochanter reattachment and checked bone remodeling through medial bone absorption. (E) Eleven years after operation, acetabular components were well fixed and bony remodeling of the allograft was observed through changes in sclerotic lesions.
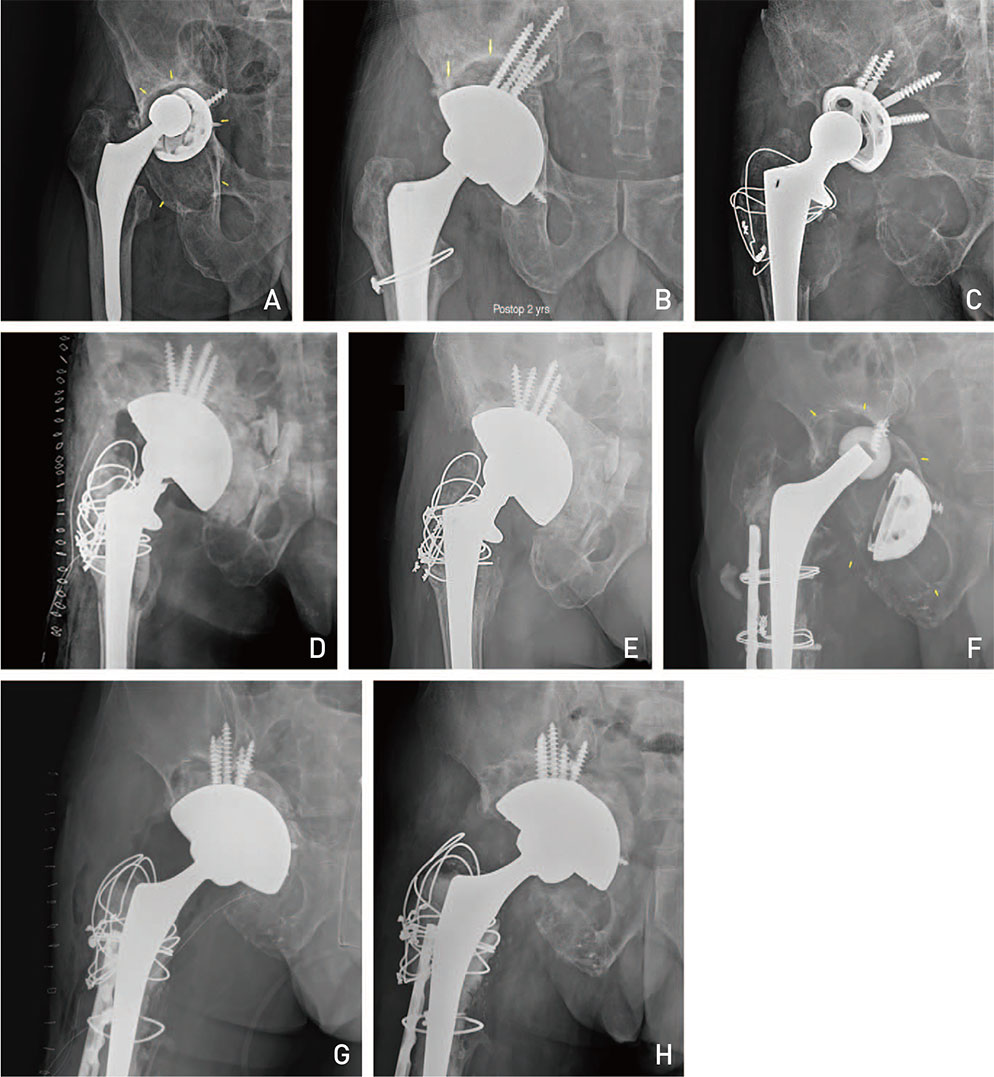
Fig. 2 (A) Preoperative anteroposterior view of a 63-year-old male patient with a bony defect and aseptic loosening requiring total hip arthroplasty (THA). (B) Revision THA with morselized impaction allograft was performed. Implants were well fixed after 2 years postoperatively. (C) Preoperative anteroposterior view of a 60-year-old male patient with bony defect and aseptic loosening requiring THA. (D) Immediate postoperative anteroposterior view showing revision THA with a morselized impacted allograft. (E) Implants were fixed after 3 years postoperatively. (F) Preoperative anteroposterior view of a 60-year-old male patient with a bony defect and aseptic loosening requiring THA. (G) Immediate postoperative anteroposterior view showing revision THA with a morselized impacted allograft. (H) Radiograph taken 2 years after revision showing bone resorption remodeling and allograft incorporation.
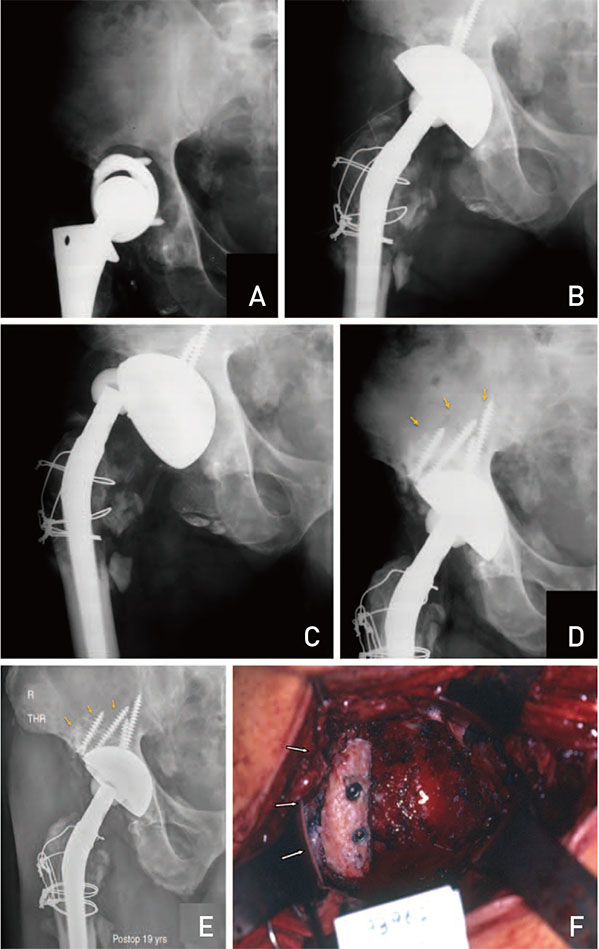
Fig. 3 (A) Preoperative anteroposterior view of a 58-year-old male patient with aseptic loosening requiring total hip arthroplasty (THA). (B) Immediate postoperative anteroposterior view showing revision THA with a morselized impacted allograft. (C) Following a traffic accident 6 weeks after surgery, fixation was lost. (D, F) Re-revision THA with morselized impaction allograft and tricortical iliac autograft was performed. Autograft was fixed with 2 screws. (E) Implants remained well fixed 19 years postoperatively. Bony union and remodeling were observed.
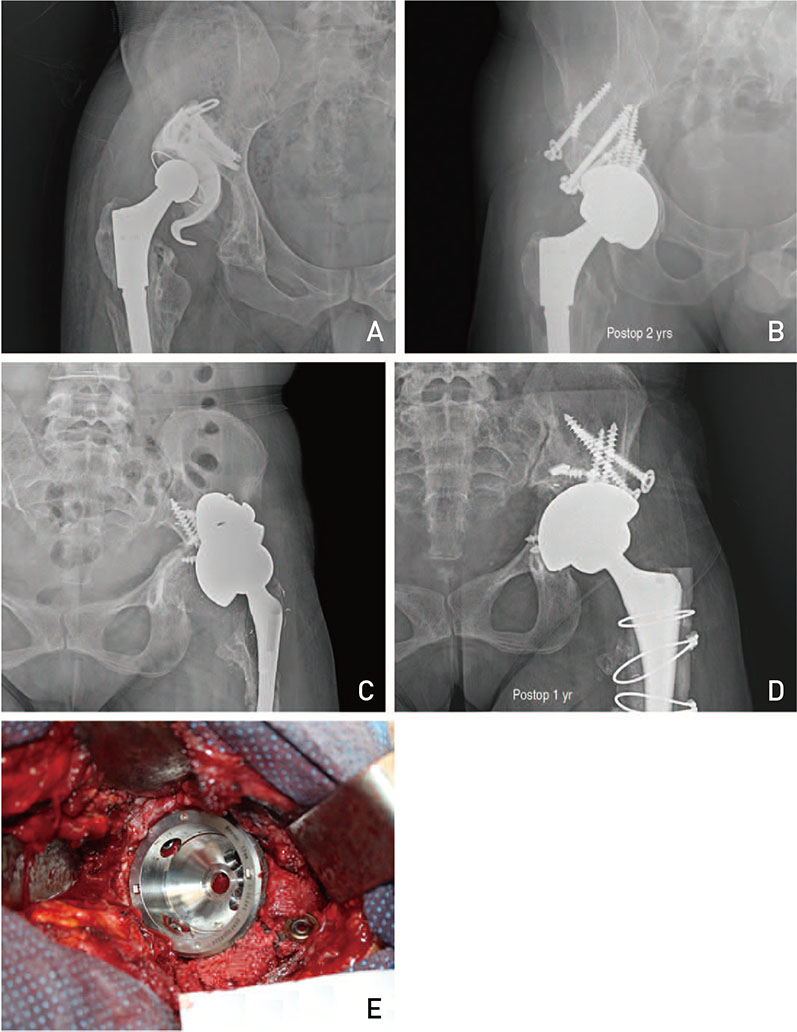
Fig. 4 (A) Preoperative anteroposterior view of a 40-year-old male patient with a severe bony defect and requiring aseptic total hip arthroplasty (THA). Immediate postoperative anteroposterior view showing revision THA with a morselized impaction allograft and 2 femoral head structural allografts was performed. (B) Radiograph taken 2 years after revision showing bone resorption remodeling and allograft incorporation. (C) Preoperative anteroposterior view of a 40-year-old female patient with a severe bony defect and requiring aseptic THA. (D) Implants were well fixed after 1 year postoperatively. (E) Immediate postoperative anteroposterior view showing revision THA with morselized impaction allograft and femoral head structural allograft.
Reference
-
1. Kurtz S, Mowat F, Ong K, Chan N, Lau E, Halpern M. Prevalence of primary and revision total hip and knee arthroplasty in the United States from 1990 through 2002. J Bone Joint Surg Am. 2005; 87:1487–1497.
Article2. Issack PS, Nousiainen M, Beksac B, Helfet DL, Sculco TP, Buly RL. Acetabular component revision in total hip arthroplasty. Part I: cementless shells. Am J Orthop (Belle Mead NJ). 2009; 38:509–514.3. Issack PS, Nousiainen M, Beksac B, Helfet DL, Sculco TP, Buly RL. Acetabular component revision in total hip arthroplasty. Part II: management of major bone loss and pelvic discontinuity. Am J Orthop (Belle Mead NJ). 2009; 38:550–556.4. Pulido L, Rachala SR, Cabanela ME. Cementless acetabular revision: past, present, and future. Revision total hip arthroplasty: the acetabular side using cementless implants. Int Orthop. 2011; 35:289–298.5. Blumenfeld TJ. Implant choices, technique, and results in revision acetabular surgery: a review. Hip Int. 2012; 22:235–247.
Article6. Jiranek WA. Acetabular liner fixation by cement. Clin Orthop Relat Res. 2003; (417):217–223.7. D'Antonio JA, Capello WN, Borden LS, et al. Classification and management of acetabular abnormalities in total hip arthroplasty. Clin Orthop Relat Res. 1989; (243):126–137.8. Paprosky WG, Perona PG, Lawrence JM. Acetabular defect classification and surgical reconstruction in revision arthroplasty. A 6-year follow-up evaluation. J Arthroplasty. 1994; 9:33–44.
Article9. Saleh KJ, Holtzman J, Gafni A, et al. Development, test reliability and validation of a classification for revision hip arthroplasty. J Orthop Res. 2001; 19:50–56.
Article10. Gustilo RB, Pasternak HS. Revision total hip arthroplasty with titanium ingrowth prosthesis and bone grafting for failed cemented femoral component loosening. Clin Orthop Relat Res. 1988; (235):111–119.
Article11. Gross AE, Allan DG, Catre M, Garbuz DS, Stockley I. Bone grafts in hip replacement surgery. The pelvic side. Orthop Clin North Am. 1993; 24:679–695.12. Parry MC, Whitehouse MR, Mehendale SA, et al. A comparison of the validity and reliability of established bone stock loss classification systems and the proposal of a novel classification system. Hip Int. 2010; 20:50–55.
Article13. Aaron AD, Wiedel JD. Allograft use in orthopedic surgery. Orthopedics. 1994; 17:41–48.
Article14. Strong DM, Friedlaender GE, Tomford WW, et al. Immunologic responses in human recipients of osseous and osteochondral allografts. Clin Orthop Relat Res. 1996; (326):107–114.
Article15. Lee JM, Roh JY, Lee JH, Wang WJ, Kim HM. Fate of morselized impaction allograft used for the defect of acetabulum in revision total hip arthroplasty. J Korean Musculoskelet Transplant Soc. 2004; 4:104–111.16. Goldberg VM, Stevenson S, Schaffer JW. Bone and cartilage allografts. In : Friedlaender GE, Goldberg VM, editors. American Academy of Orthopaedic Surgeons Symposium. vol. 1. Park Ridge, IL: American Academy of Orthopaedic Surgeons;1991. p. 3–12.17. Dearborn JT, Harris WH. High placement of an acetabular component inserted without cement in a revision total hip arthroplasty. Results after a mean of ten years. J Bone Joint Surg Am. 1999; 81:469–480.
Article18. Doehring TC, Rubash HE, Shelley FJ, Schwendeman LJ, Donaldson TK, Navalgund YA. Effect of superior and superolateral relocations of the hip center on hip joint forces. An experimental and analytical analysis. J Arthroplasty. 1996; 11:693–703.
Article19. Murayama T, Ohnishi H, Okabe S, et al. 15-year comparison of cementless total hip arthroplasty with anatomical or high cup placement for Crowe I to III hip dysplasia. Orthopedics. 2012; 35:e313–e318.
Article20. Hendricks KJ, Harris WH. High placement of noncemented acetabular components in revision total hip arthroplasty. A concise follow-up, at a minimum of fifteen years, of a previous report. J Bone Joint Surg Am. 2006; 88:2231–2236.
Article21. Namba R, Scott RD. Acetabular revision with the bipolar prosthesis and particulate bone grafting. Semin Arthroplasty. 1993; 4:87–91.22. Oakeshott RD, Morgan DA, Zukor DJ, Rudan JF, Brooks PJ, Gross AE. Revision total hip arthroplasty with osseous allograft reconstruction. A clinical and roentgenographic analysis. Clin Orthop Relat Res. 1987; (225):37–61.23. Papagelopoulos PJ, Lewallen DG, Cabanela ME, McFarland EG, Wallrichs SL. Acetabular reconstruction using bipolar endoprosthesis and bone grafting in patients with severe bone deficiency. Clin Orthop Relat Res. 1995; (314):170–184.
Article24. McFarland EG, Lewallen DG, Cabanela ME. Use of bipolar endoprosthesis and bone grafting for acetabular reconstruction. Clin Orthop Relat Res. 1991; (268):128–139.25. Takatori Y, Ninomiya S, Umeyama T, Yamamoto M, Moro T, Nakamura K. Bipolar revision arthroplasty for failed threaded acetabular components: radiographic evaluation of cup migration. J Orthop Sci. 2002; 7:467–471.
Article26. Leopold SS, Jacobs JJ, Rosenberg AG. Cancellous allograft in revision total hip arthroplasty. A clinical review. Clin Orthop Relat Res. 2000; (371):86–97.27. Paprosky WG, Magnus RE. Principles of bone grafting in revision total hip arthroplasty. Acetabular technique. Clin Orthop Relat Res. 1994; (298):147–155.28. Yoo MC. [Revision total hip arthroplasty using acetabular reinforcement ring]. J Korean Hip Soc. 2004; 16:183–190. Korean.29. Berry DJ, Müller ME. Revision arthroplasty using an anti-protrusio cage for massive acetabular bone deficiency. J Bone Joint Surg Br. 1992; 74:711–715.
Article30. Zehntner MK, Ganz R. Midterm results (5.5–10 years) of acetabular allograft reconstruction with the acetabular reinforcement ring during total hip revision. J Arthroplasty. 1994; 9:469–479.
Article31. Slooff TJ, Huiskes R, van Horn J, Lemmens AJ. Bone grafting in total hip replacement for acetabular protrusion. Acta Orthop Scand. 1984; 55:593–596.
Article32. Hwang KT, Kim YH. Revision total hip arthroplasty of an acetabular cup with acetabular bone defects. J Korean Hip Soc. 2011; 23:237–247.
Article33. Trumm BN, Callaghan JJ, George CA, Liu SS, Goetz DD, Johnston RC. Minimum 20-year follow-up results of revision total hip arthroplasty with improved cementing technique. J Arthroplasty. 2014; 29:236–241.
Article34. Highcock A, Siney P, Wroblewski BM, Wynne Jones H, Raut VV. Severe femoral osteolysis treated with a cemented Charnley revision arthroplasty. Clinical and radiological follow-up to 27 years. Orth Proc. 2015; 97-B:51.35. Slooff TJ, Buma P, Schreurs BW, Schimmel JW, Huiskes R, Gardeniers J. Acetabular and femoral reconstruction with impacted graft and cement. Clin Orthop Relat Res. 1996; (324):108–115.
Article36. Buttaro MA, Comba F, Pusso R, Piccaluga F. Acetabular revision with metal mesh, impaction bone grafting, and a cemented cup. Clin Orthop Relat Res. 2008; 466:2482–2490.
Article37. Comba F, Buttaro M, Pusso R, Piccaluga F. Acetabular revision surgery with impacted bone allografts and cemented cups in patients younger than 55 years. Int Orthop. 2009; 33:611–616.
Article38. Schreurs BW, Luttjeboer J, Thien TM, et al. Acetabular revision with impacted morselized cancellous bone graft and a cemented cup in patients with rheumatoid arthritis. A concise follow-up, at eight to nineteen years, of a previous report. J Bone Joint Surg Am. 2009; 91:646–651.
Article39. Jasty M, Harris WH. Total hip reconstruction using frozen femoral head allografts in patients with acetabular bone loss. Orthop Clin North Am. 1987; 18:291–299.
Article40. Pellicci PM, Wilson PD Jr, Sledge CB, et al. Long-term results of revision total hip replacement. A follow-up report. J Bone Joint Surg Am. 1985; 67:513–516.
Article41. Kavanagh BF, Ilstrup DM, Fitzgerald RH Jr. Revision total hip arthroplasty. J Bone Joint Surg Am. 1985; 67:517–526.
Article42. Bal BS, Maurer T, Harris WH. Revision of the acetabular component without cement after a previous acetabular reconstruction with use of a bulk femoral head graft in patients who had congenital dislocation or dysplasia. A follow-up note. J Bone Joint Surg Am. 1999; 81:1703–1706.
Article43. Gross AE. Revision arthroplasty of the acetabulum with restoration of bone stock. Clin Orthop Relat Res. 1999; (369):198–207.
Article44. Silverton CD, Rosenberg AG, Sheinkop MB, Kull LR, Galante JO. Revision total hip arthroplasty using a cementless acetabular component. Technique and results. Clin Orthop Relat Res. 1995; (319):201–208.45. Sun C, Lian YY, Jin YH, Zhao CB, Pan SQ, Liu XF. Clinical and radiographic assessment of cementless acetabular revision with morsellised allografts. Int Orthop. 2009; 33:1525–1530.
Article46. Leopold SS, Rosenberg AG, Bhatt RD, Sheinkop MB, Quigley LR, Galante JO. Cementless acetabular revision. Evaluation at an average of 10.5 years. Clin Orthop Relat Res. 1999; (369):179–186.47. Rosenberg AG. Cementless acetabular components: the gold standard for socket revision. J Arthroplasty. 2003; 18(3):Suppl 1. 118–120.
Article48. Levine B, Della Valle CJ, Jacobs JJ. Applications of porous tantalum in total hip arthroplasty. J Am Acad Orthop Surg. 2006; 14:646–655.
Article49. Siegmeth A, Duncan CP, Masri BA, Kim WY, Garbuz DS. Modular tantalum augments for acetabular defects in revision hip arthroplasty. Clin Orthop Relat Res. 2009; 467:199–205.
Article50. Weeden SH, Schmidt RH. The use of tantalum porous metal implants for Paprosky 3A and 3B defects. J Arthroplasty. 2007; 22(6):Suppl 2. 151–155.
Article51. Nehme A, Lewallen DG, Hanssen AD. Modular porous metal augments for treatment of severe acetabular bone loss during revision hip arthroplasty. Clin Orthop Relat Res. 2004; (429):201–208.
Article52. Boscainos PJ, Kellett CF, Maury AC, Backstein D, Gross AE. Management of periacetabular bone loss in revision hip arthroplasty. Clin Orthop Relat Res. 2007; 465:159–165.
Article53. Ballester Alfaro JJ, Sueiro Fernández J. Trabecular Metal buttress augment and the Trabecular Metal cup-cage construct in revision hip arthroplasty for severe acetabular bone loss and pelvic discontinuity. Hip Int. 2010; 20:Suppl 7. S119–S127.
Article54. Staheli LT. Slotted acetabular augmentation. J Pediatr Orthop. 1981; 1:321–327.
Article55. Lee JM, Cho KH, Cha YS. A morselized impaction allograft used for the defect of acetabulum in revision total hip arthroplasty: minimum 10-year follow-up. J Korean Musculoskelet Transplant Soc. 2012; 12:76–84.56. Lee JM, Nam HT. Acetabular revision total hip arthroplasty using an impacted morselized allograft and a cementless cup: minimum 10-year follow-up. J Arthroplasty. 2011; 26:1057–1060.
Article57. Lee JM, Sun MY, Jeon JB. Acetabular revision total hip arthroplasty using morselized impaction allograft for acetabular bone defect above Paprosky type III. J Korean Musculoskelet Transplant Soc. 2013; 13:58–64.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Acetabular Revision Total Hip Arthroplasty Using Uncemented Cup and Morselized Impacted Allograft
- Acetabular Reconstruction with Impacted Morselized Allograft, Wire Mesh and Cemented Acetabular Cup in Severe Acetabular Bone Defect
- Revision Total Hip Arthroplasty of an Acetabular Cup with Acetabular Bone Defects
- Revision Total Hip Arthroplasty using Morselized Femoral Head Allograft and Cementless Cup in Acetabular Bone Deficiency
- Reconstruction of the Acetabular Bone Defect with Morselized Bone Grafts in Acetabular Cup Revision Screw fixed Hemispherical Cup vs. Bipolar Cup
