Porous Femoral Fixation in Total Hip Arthroplasty with Short Anatomical Stem: Radiographic Evaluation
- Affiliations
-
- 1Department of Orthopedic Surgery, University of Chicago at Weiss Memorial Hospital, Chicago, IL, USA. dsspatil@gmail.com
- 2Clinch Valley Medical Center, Richlands, VA, USA.
- 3Department of Orthopedic Surgery, Mount Sinai Hospital, Chicago, IL, USA.
- KMID: 2412260
- DOI: http://doi.org/10.4055/cios.2017.9.3.255
Abstract
- BACKGROUND
Hip prostheses with short anatomical stems were designed for metaphyseal fixation and to spare bone stock. We present a study of a short anatomical femoral stem used in all age groups of patients with Dorr A and B type of femora.
METHODS
We reviewed radiographs of 85 hips in 74 patients who had a cementless total hip arthroplasty with a short anatomical 80 mm femoral stem designed to achieve pure metaphyseal fixation. A ream-only technique was used for femoral canal preparation in all patients. At each follow-up, radiological evaluation was performed for stem alignment, proximal metaphyseal fill, subsidence, status of biological fixation of the femoral stem, heterotrophic ossification, radiolucency, osteolysis, and limb length discrepancy of the stem. Acetabular components were evaluated for positioning, acetabular bone coverage, and radiolucent and osteolytic lesions.
RESULTS
The final mean alignment of femoral stem was 2° valgus. The average intramedullary fill by the stem at the proximal level of the lesser trochanter was 93% in the coronal plane and 88% in the sagittal plane. No components were considered to be undersized. Thirteen hips (15.2%) presented radiolucent lines (10 hips < 1 mm in width and 3 hips [3.5%] 2 mm in width) and 100% of them were not progressive with respect to the last follow-up radiograph. All of the stems had excellent fixation by demonstrating bone ingrowth at the latest follow-up. At the last follow-up, heterotopic ossification was noted in 5 hips. The mean preoperative limb length discrepancy was 9.3 mm and the mean postoperative discrepancy was 3.8 mm. The mean acetabular component angle of the 85 components was 41.2° with a mean anteversion of 22.1°. At the last follow-up, there were no revisions of the femoral component. One patient, 25 months after the index operation, required an acetabular component revision because of recurrent hip dislocation. There were no radiological signs of loosening in any of the short-stem prostheses at the last examination.
CONCLUSIONS
The short, metaphyseal-fitting anatomic cementless femoral stem provided stable fixation without relying on diaphyseal fixation.
Keyword
MeSH Terms
Figure
-
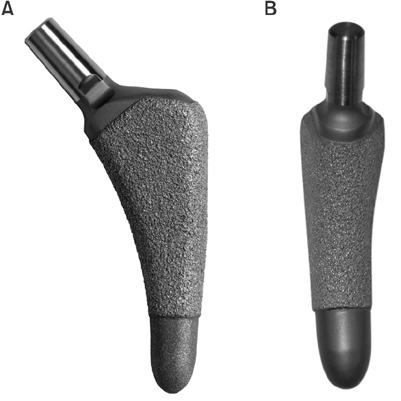
Fig. 1 Sagittal (A) and coronal (B) views of a cementless Balance Microplasty Stem (Biomet) that has a modified 3-degree bi-planar taper geometry. The proximal 80% portion of the stem is circumferentially coated with porous plasma spray.

Fig. 2 Schematic of a ream-only technique. (A) Removal of the calcar metaphyseal cancellous bone using a 3-degree conical reamer. (B) Removal of the cancellous bone in the greater trochanter, avoiding varus positioning of the femoral component.
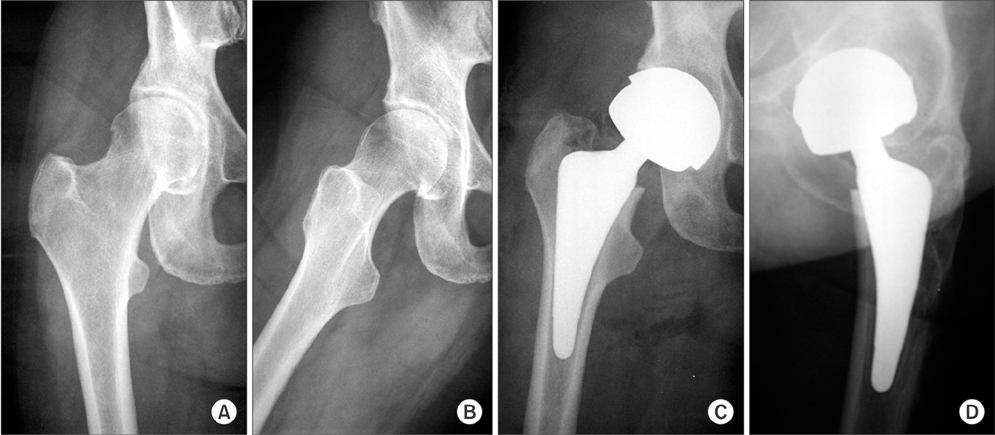
Fig. 3 Preoperative and postoperative radiographs of the right hip of a female who was 65 years old at the time of the right primary total hip replacement. (A and B) Preoperative anteroposterior and lateral radiographs demonstrating osteoarthritis of the hip with partial loss of the joint space and formation of osteophytes. (C and D) Anteroposterior and lateral radiographs at 2 years after total hip replacement with use of a cementless hip Balance Microplasty Stem (Biomet) and a M2A-Magnum (Biomet) metal-on-metal acetabular component. Note the excellent osseointegration and absence of radiolucent lines at the implant-bone interface.
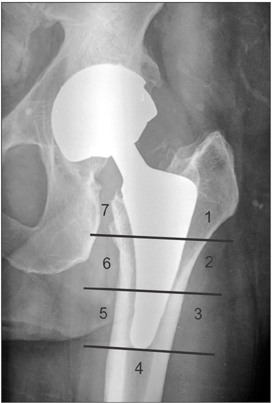
Fig. 4 Gruen's zones. Zones 1 and 2 were divided by a line through 50% of the lateral porous-coated area of the stem. Zones 6 and 7 represented the same areas on the medial side. Zones 3, 4, and 5 included the lateral smooth portion, the distal smooth portion, and the medial smooth portion of the stem, respectively.
Reference
-
1. Ahnfelt L, Herberts P, Malchau H, Andersson GB. Prognosis of total hip replacement: a Swedish multicenter study of 4,664 revisions. Acta Orthop Scand Suppl. 1990; 238:1–26.2. Callaghan JJ, Dysart SH, Savory CG. The uncemented porous-coated anatomic total hip prosthesis: two-year results of a prospective consecutive series. J Bone Joint Surg Am. 1988; 70(3):337–346.
Article3. Cameron HU. The results of early clinical trials with a microporus coated metal hip prosthesis. Clin Orthop Relat Res. 1982; (165):188–190.4. Lord G, Bancel P. The madreporic cementless total hip arthroplasty: new experimental data and a seven-year clinical follow-up study. Clin Orthop Relat Res. 1983; (176):67–76.5. Archibeck MJ, Berger RA, Jacobs JJ, et al. Second-generation cementless total hip arthroplasty: eight to eleven-year results. J Bone Joint Surg Am. 2001; 83(11):1666–1673.6. Bobyn JD, Mortimer ES, Glassman AH, Engh CA, Miller JE, Brooks CE. Producing and avoiding stress shielding: laboratory and clinical observations of noncemented total hip arthroplasty. Clin Orthop Relat Res. 1992; (274):79–96.7. Burt CF, Garvin KL, Otterberg ET, Jardon OM. A femoral component inserted without cement in total hip arthroplasty: a study of the Tri-Lock component with an average ten-year duration of follow-up. J Bone Joint Surg Am. 1998; 80(7):952–960.
Article8. Whiteside LA, Arima J, White SE, Branam L, McCarthy DS. Fixation of the modular total hip femoral component in cementless total hip arthroplasty. Clin Orthop Relat Res. 1994; (298):184–190.9. Mallory TH, Head WC, Lombardi AV Jr. Tapered design for the cementless total hip arthroplasty femoral component. Clin Orthop Relat Res. 1997; (344):172–178.
Article10. Taunt CJ Jr, Finn H, Baumann P. Immediate weight bearing after cementless total hip arthroplasty. Orthopedics. 2008; 31(3):223.
Article11. Hodgkinson JP, Shelley P, Wroblewski BM. The correlation between the roentgenographic appearance and operative findings at the bone-cement junction of the socket in Charnley low friction arthroplasties. Clin Orthop Relat Res. 1988; (228):105–109.
Article12. Kim YH. Cementless total hip arthroplasty with a close proximal fit and short tapered distal stem (third-generation) prosthesis. J Arthroplasty. 2002; 17(7):841–850.
Article13. Morrey BF, Adams RA, Kessler M. A conservative femoral replacement for total hip arthroplasty: a prospective study. J Bone Joint Surg Br. 2000; 82(7):952–958.14. Santori FS, Manili M, Fredella N, Tonci Ottieri M, Santori N. Ultra-short stems with proximal load transfer: clinical and radiographic results at five-year follow-up. Hip Int. 2006; 16:Suppl 3. 31–39.
Article15. Dorr LD, Faugere MC, Mackel AM, Gruen TA, Bognar B, Malluche HH. Structural and cellular assessment of bone quality of proximal femur. Bone. 1993; 14(3):231–242.
Article16. Charnley J. The long-term results of low-friction arthroplasty of the hip performed as a primary intervention. J Bone Joint Surg Br. 1972; 54(1):61–76.
Article17. Martell JM, Pierson RH 3rd, Jacobs JJ, Rosenberg AG, Maley M, Galante JO. Primary total hip reconstruction with a titanium fiber-coated prosthesis inserted without cement. J Bone Joint Surg Am. 1993; 75(4):554–571.
Article18. Kim YH, Kim VE. Uncemented porous-coated anatomic total hip replacement: results at six years in a consecutive series. J Bone Joint Surg Br. 1993; 75(1):6–13.
Article19. Brooker AF, Bowerman JW, Robinson RA, Riley LH Jr. Ectopic ossification following total hip replacement: incidence and a method of classification. J Bone Joint Surg Am. 1973; 55(8):1629–1632.20. Gruen TA, McNeice GM, Amstutz HC. “Modes of failure” of cemented stem-type femoral components: a radiographic analysis of loosening. Clin Orthop Relat Res. 1979; (141):17–27.21. Johnston RC, Crowninshield RD. Roentgenologic results of total hip arthroplasty: a ten-year follow-up study. Clin Orthop Relat Res. 1983; (181):92–98.22. Zicat B, Engh CA, Gokcen E. Patterns of osteolysis around total hip components inserted with and without cement. J Bone Joint Surg Am. 1995; 77(3):432–439.
Article23. Engh CA, Massin P, Suthers KE. Roentgenographic assessment of the biologic fixation of porous-surfaced femoral components. Clin Orthop Relat Res. 1990; (257):107–128.
Article24. Engh CA, Bobyn JD, Glassman AH. Porous-coated hip replacement: the factors governing bone ingrowth, stress shielding, and clinical results. J Bone Joint Surg Br. 1987; 69(1):45–55.
Article25. Engh CA, O'Connor D, Jasty M, McGovern TF, Bobyn JD, Harris WH. Quantification of implant micromotion, strain shielding, and bone resorption with porous-coated anatomic medullary locking femoral prostheses. Clin Orthop Relat Res. 1992; (285):13–29.
Article26. DeLee JG, Charnley J. Radiological demarcation of cemented sockets in total hip replacement. Clin Orthop Relat Res. 1976; (121):20–32.
Article27. Hube R, Zaage M, Hein W, Reichel H. Early functional results with the Mayo-hip, a short stem system with metaphyseal-intertrochanteric fixation. Orthopade. 2004; 33(11):1249–1258.28. Hallan G, Lie SA, Furnes O, Engesaeter LB, Vollset SE, Havelin LI. Medium- and long-term performance of 11,516 uncemented primary femoral stems from the Norwegian arthroplasty register. J Bone Joint Surg Br. 2007; 89(12):1574–1580.29. Khalily C, Whiteside LA. Predictive value of early radiographic findings in cementless total hip arthroplasty femoral components: an 8- to 12-year follow-up. J Arthroplasty. 1998; 13(7):768–773.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Short Term Results of Cementless Total Hip Arthroplasty With a Tapered Femoral Component
- Revision of Total Hip Arthroplasty Using Extensively Porous-Coated Femoral Stem
- Femoral Osteolysis in Total Hip Arthroplasty with Circumferentially Porous Coated Multilock(R) Femoral Stem
- Short-term Results after Cementless Total Hip Arthroplasty Using a Fully Hydroxyapatite-coated Femoral Stem
- Revision Total Hip Arthroplasty with a Strut Allograft and an Extensively Porous-Coated Femoral Stem
