Comparison of Postoperative Results of One Day Laser-assisted in-situ Keratomileusis, Laser-assisted Sub-epithelial Keratectomy Surgery, and Conventional Surgery
- Affiliations
-
- 1B&VIIt Eye Center, Seoul, Korea. kiki0306@hanmail.net
- KMID: 2411449
- DOI: http://doi.org/10.3341/jkos.2018.59.5.410
Abstract
- PURPOSE
To evaluate the postoperative results of one day laser-assisted in-situ keratomileusis (LASIK) or laser-assisted sub-epithelial keratectomy (LASEK) procedures, which were performed on the same day as preoperative examinations, including fundus examinations after dilating the pupil.
METHODS
This study included 226 LASIK patients (226 eyes) and 201 LASEK patients (201 eyes) who underwent surgery with Visumax and EX500 from January to December in 2016. We divided the patients into two groups. The one-day surgery group (one-day group) underwent surgery on the same day as preoperative examinations, including dilated fundus examinations. The scheduled surgery group (scheduled group) underwent surgery on the scheduled day after the preoperative examinations. In the one-day group, the surgery was usually performed 2-5 hours after instillation of the pupil dilating eye drops.
RESULTS
Among LASIK patients, the one-day group included 109 patients and the scheduled group included 117 patients. The postoperative myopic errors were 0.06 ± 0.37 diopters (D) and 0.07 ± 0.36 D, respectively (p = 0.91). The postoperative astigmatism was −0.38 ± 0.24 D and −0.37 ± 0.24 D, respectively (p = 0.77). The postoperative uncorrected visual acuity was −0.05 ± 0.03 logMAR and −0.06 ± 0.03 logMAR, respectively (p = 0.13). Among LASEK patients, the one-day group included 107 patients and the scheduled group included 94 patients. The postoperative myopic error was 0.18 ± 0.52 D and 0.22 ± 0.54 D, respectively (p = 0.95). The postoperative astigmatism was −0.48 ± 0.30 D and −0.46 ± 0.29 D, respectively (p = 0.14). The postoperative uncorrected visual acuity was −0.05 ± 0.03 logMAR and −0.06 ± 0.03 logMAR, respectively (p = 0.33).
CONCLUSIONS
The postoperative results of the one-day LASIK and LASEK patients, whose surgery was performed on the same day as the preoperative examinations, were not significantly different from those using the conventional method.
Keyword
MeSH Terms
Figure
-
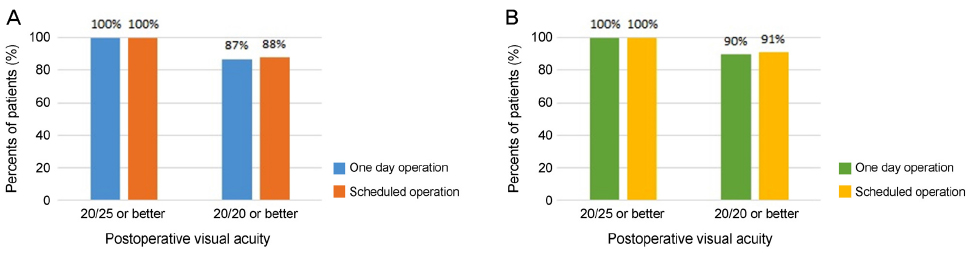
Figure 1 Comparison of postoperative uncorrected visual acuity between the same day operation group and scheduled operation group. Postoperative visual acuity after laser-assisted in-situ keratomileusis of 226 patients (A) and postoperative visual acuity after laser-assisted sub-epithelial keratectomy of 201 patients (B).
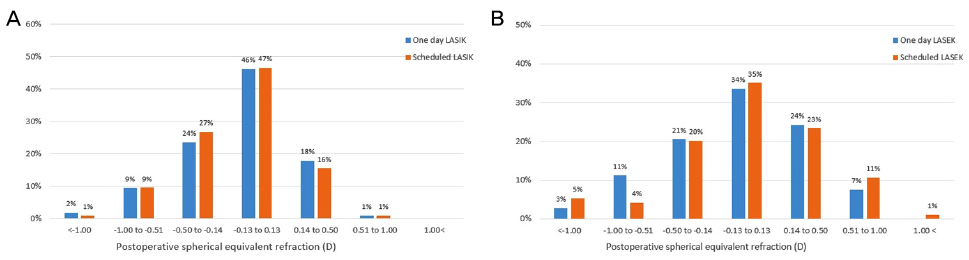
Figure 2 Refractive outcomes of the one day operation and scheduled operation group. The spherical equivalent refraction of one day laser-assisted in-situ keratomileusis (LASIK) group and scheduled LASIK group at postoperative 1 month (A). The spherical equivalent refraction of one day laser-assisted sub-epithelial keratectomy (LASEK) group and scheduled LASEK group at postoperative 6 months (B).
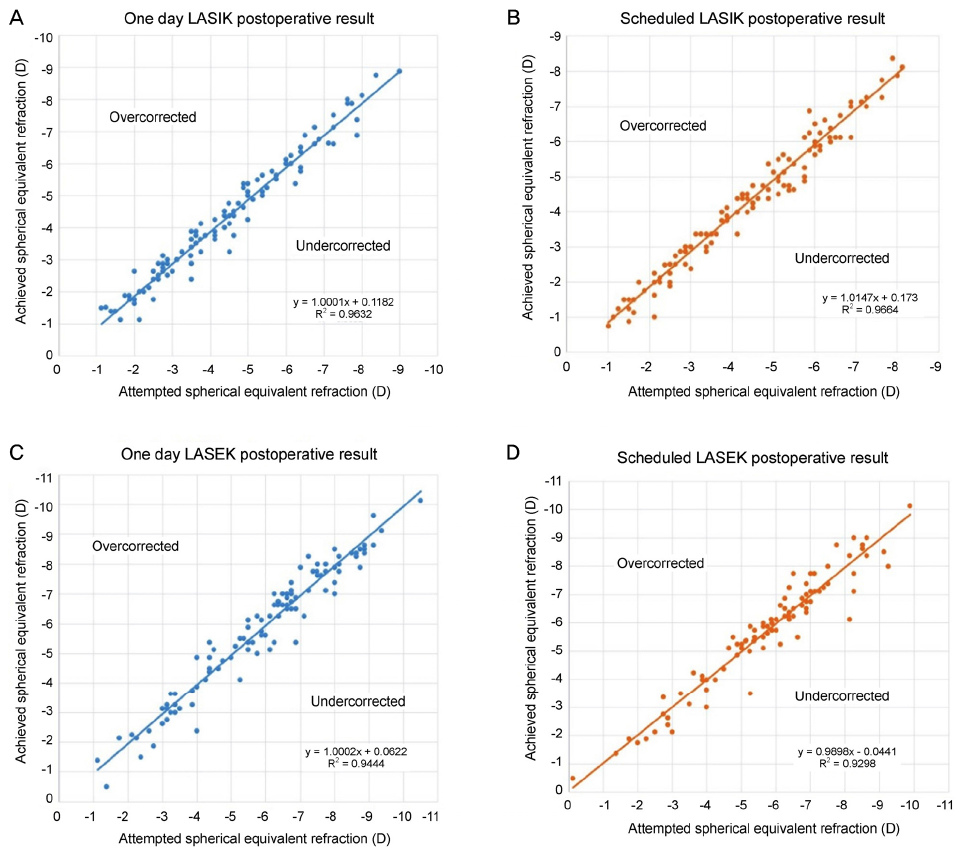
Figure 3 Predictability of spherical equivalent correction of the one day operation and scheduled operation group. The results of the one day laser-assisted in-situ keratomileusis (LASIK) group (A) and scheduled LASIK group (B) at postoperative 1 month. The results of one day laser-assisted sub-epithelial keratectomy (LASEK) group (C) and scheduled LASEK group (D) at postoperative 6 months.
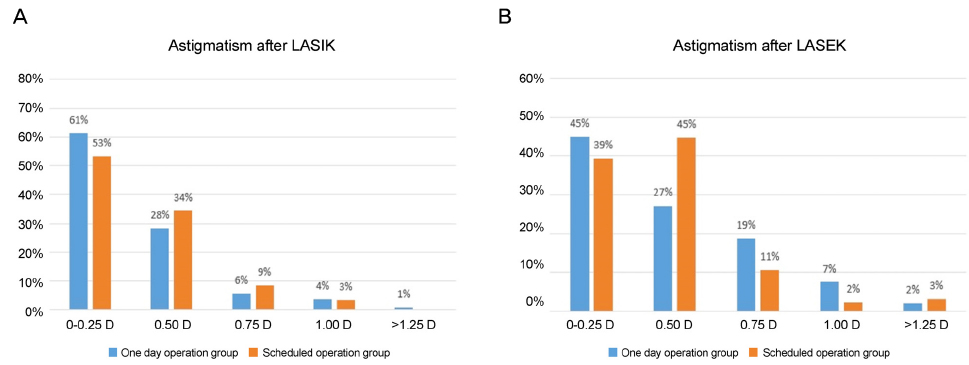
Figure 4 Postoperative refractive astigmatism distribution. Astigmatism after the one day laser-assisted in-situ keratomileusis (LASIK) group and scheduled LASIK group at postoperative 1 month (A), and astigmatism after the one day laser-assisted sub-epithelial keratectomy (LASEK) group and scheduled LASEK group at postoperative 6 months (B).
Reference
-
1. O'Brart DP, Shalchi Z, Mcdonald RJ, et al. Twenty-year follow-up of a randomized prospective clinical trial of excimer laser photorefractive keratectomy. Am J Ophthalmol. 2014; 158:651–663.2. Sandoval HP, Donnenfeld ED, Kohnen T, et al. Modern laser in situ keratomileusis outcomes. J Cataract Refract Surg. 2016; 42:1224–1234.
Article3. Lam DS, Fan DS, Chan WM, et al. Prevalence and characteristics of peripheral retinal degeneration in Chinese adults with high myopia: a cross-sectional prevalence survey. Optom Vis Sci. 2005; 82:235–238.
Article4. Arevalo JF. Retinal complications after laser-assisted in situ keratomileusis (LASIK). Curr Opin Ophthalmol. 2004; 15:184–191.
Article5. Lewis H. Peripheral retinal degenerations and the risk of retinal detachment. Am J Ophthalmol. 2003; 136:155–160.
Article6. Lin SC, Tseng SH. Prophylactic laser photocoagulation for retinal breaks before laser in situ keratomileusis. J Refract Surg. 2003; 19:661–665.
Article7. Lin J, Xie X, Du X, et al. Incidence of vitreoretinal pathologic conditions in myopic eyes after laser in situ keratomileusis. Zhonghua Yan Ke Za Zhi. 2002; 38:546–549.8. Wright KW, Strube YNJ. 3rd ed. New York: Oxford University Press;2012. p. 92.9. Lee YC. Active eye-tracking improves LASIK results. J Refract Surg. 2007; 23:581–585.
Article10. Mosquera SA, Arbelaez MC. Use of a six-dimensional eye-tracker in corneal laser refractive surgery with the Schwind Amaris Maris TotalTech laser. J Refract Surg. 2011; 27:582–590.11. Meidani A, Tzavara C. Comparison of efficacy, safety, and predictability of laser in situ keratomileusis using two laser suites. Clin Ophthalmol. 2016; 10:1639–1646.12. Waring GO 3rd. One-kilohertz eye tracker and active intraoperative torsion detection in the NIDEK CXIII and Quest excimer lasers. J Refract Surg. 2009; 25:10 Suppl. S931–S933.
Article13. Pajic B, Cvejic Z, Mijatovic Z, et al. Excimer laser surgery: biometrical iris eye recognition with cyclorotational control eye tracker system. Sensors (Basel). 2017; 17:pii: E1211.
Article14. Ciccio AE, Durrie DS, Stahl JE, Schwendeman F. Ocular cyclotorsion during customized laser ablation. J Refract Surg. 2005; 21:S772–S774.
Article15. Chang J. Cyclotorsion during laser in situ keratomileusis. J Cataract Refract Surg. 2008; 34:1720–1726.
Article16. Reinstein DZ, Gobbe M, Gobbe L, et al. Optical zone centration accuracy using corneal fixation-based SMILE compared to eye tracker-based femtosecond laser-assisted LASIK for myopia. J Refract Surg. 2015; 31:586–592.
Article17. Piñero DP, Teus MA. Clinical outcomes of small-incision lenticule extraction and femtosecond laser-assisted wavefront-guided laser-in situ keratomileusis. J Cataract Refract Surg. 2016; 42:1078–1093.18. Chan C, Lawless M, Sutton G, et al. Small incision lenticule extraction (SMILE) in 2015. Clin Exp Optom. 2016; 99:204–212.
Article19. Nagiel A, Lalane RA, Sadda SR, Schwartz SD. Ultra-widefield fundus imaging: A review of clinical applications and future trends. Retina. 2016; 36:660–678.20. Wilkes SR, Beard CN, Kurland LT, et al. The incidence of retinal detachment in Rochester, Minnesota, 1970-1978. Am J Ophthalmol. 1982; 94:670–673.
Article21. Ghosh S, Couper TA, Lamoureux E, et al. Evaluation of iris recognition system for wavefront-guided laser in situ keratomileusis for myopic astigmatism. J Cataract Refract Surg. 2008; 34:215–221.
Article22. Motwani M. The use of WaveLight(R) Contoura to create a uniform cornea: the LYRA Protocol. Part 2: the consequences of treating astigmatism on an incorrect axis via excimer laser. Clin Ophthalmol. 2017; 11:907–913.23. Kanellopoulos AJ. Topography-modified refraction (TMR): adjustment of treated cylinder amount and axis to the topography versus standard clinical refraction in myopic topography-guided LASIK. Clin Ophthalmol. 2016; 10:2213–2221.
Article24. Utine CA, Altunsoy M, Basar D. Visante anterior segment OCT in a patient with ga sbubbles in the anterior chamber after femtosecond laser corneal flap formation. Int Ophthalmol. 2010; 30:81–84.25. Gimeno FL, Chan CM, Li L, et al. Comparison of eye-tracking success in laser in situ keratomileusis after flap creation with 2 femtosecond laser models. J Cataract Refract Surg. 2011; 37:538–543.
Article26. de Ortueta D, Arba-Mosquera S. Laser in situ keratomileusis for high hyperopia with corneal vertex centration and asymmetric offset. Eur J Ophthalmol. 2017; 27:141–152.
Article27. Narváez J, Brucks M, Zimmerman G, et al. Intraoperative cyclorotation and pupil centroid shift during LASIK and PRK. J Refract Surg. 2012; 28:353–357.
Article28. Motwani M, Pei R. Treatment of moderate-to-high hyperopia with the WaveLight Allegretto 400 and EX500 excimer laser systems. Clin Ophthalmol. 2017; 11:999–1007.
Article29. Kanellopoulos AJ, Asimellis G. LASIK ablation centration: an objective digitized assessment and comparison between two generations of an excimer laser. J Refract Surg. 2015; 31:164–169.
Article30. Kim WK, Cho EY, Kim HS, Kim JK. The incidence of increased intraocular pressure when using 01% fluorometholone after photorefractive keratectomy. J Korean Ophthalmol Soc. 2015; 56:985–991.
Article31. Chen X, Stojanovic A, Stojanovic F, et al. Effect of limbal marking prior to laser ablation on the magnitude of cyclotorsional error. J Refract Surg. 2012; 28:358–362.
Article32. Shajari M, Bühren J, Kohnen T. Dynamic torsional misalignment of eyes during laser in-situ keratomileusis. Graefes Arch Clin Exp Ophthalmol. 2016; 254:911–916.
Article33. Febbraro JL, Koch DD, Khan HN, et al. Detection of static cyclotorsion and compensation for dynamic cyclotorsion in laser in situ keratomileusis. J Cataract Refract Surg. 2010; 36:1718–1723.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Comparison in Pain between Photorefractive Keratectomy and Laser In Situ Epithelial Keratomileusis during Intraoperative and Postoperative Period
- Comparison of Laser Epithelial Keratomileusis Versus Epipolis-Laser in Situ Keratomileusis for Moderate to High Myopia
- Development of EKC after Eximer Laser Photorefractive Surgery and Subsequent Recurrence of EKC-like Keratitis
- Comparison of Photorefractive Keratectomy and Laser Epithelial Keratomileusis for Low to Moderate Myopia
- Short Term Clinical Results of Laser Epithelial Keratomileusis and Epi-Laser in Situ Keratomileusis for Moderate and High Myopia
