Bile Duct Patency Maintained after Intraductal Radiofrequency Ablation in a Case of Hepatocellular Cholangiocarcinoma with Bile Duct Invasion
- Affiliations
-
- 1Department of Internal Medicine, Pusan National University Hospital, Biomedical Research Institute, and Pusan National University School of Medicine, Busan, Korea. gasong@pusan.ac.kr
- KMID: 2410990
- DOI: http://doi.org/10.5946/ce.2017.097
Abstract
- Combined hepatocellular-cholangiocarcinoma (HCC-CC) with bile duct invasion (BDI) is rare. In unresectable cases, biliary stent placement and photodynamic therapy (PDT) are used for resolving obstructive jaundice. However, stent occlusion remains problematic, and PDT is expensive and time-consuming. Intraductal radiofrequency ablation (RFA) is an emerging procedure for palliation in these patients. It has potential benefits including less expense, lower rates of severe complication, longer maintenance of ductal patency, and easier technique compared with PDT or stenting alone. We report a 67-year-old man who underwent repeated intraductal RFA for HCC-CC and HCC with BDI, for whom bile duct patency was maintained without additional biliary procedures.
MeSH Terms
Figure
-

Fig. 1. Computed tomography (CT) image. (A) An initial CT revealed a 6.6-cm main mass at S2/3 and a 2-cm intraductal mass at the left proximal intrahepatic bile duct. (B) A follow-up CT after 5 months revealed the disappearance of the left intrahepatic ductal dilatation after the first intraductal radiofrequency ablation (RFA) procedure and the sixth cycle of chemotherapy. (C) The next follow-up CT after 7 months revealed a recurrent intraductal mass with dilatation of the left intrahepatic bile duct. (D) A follow-up CT after 9 months revealed that the left intrahepatic bile duct dilatation was improved after repeated intraductal RFA.
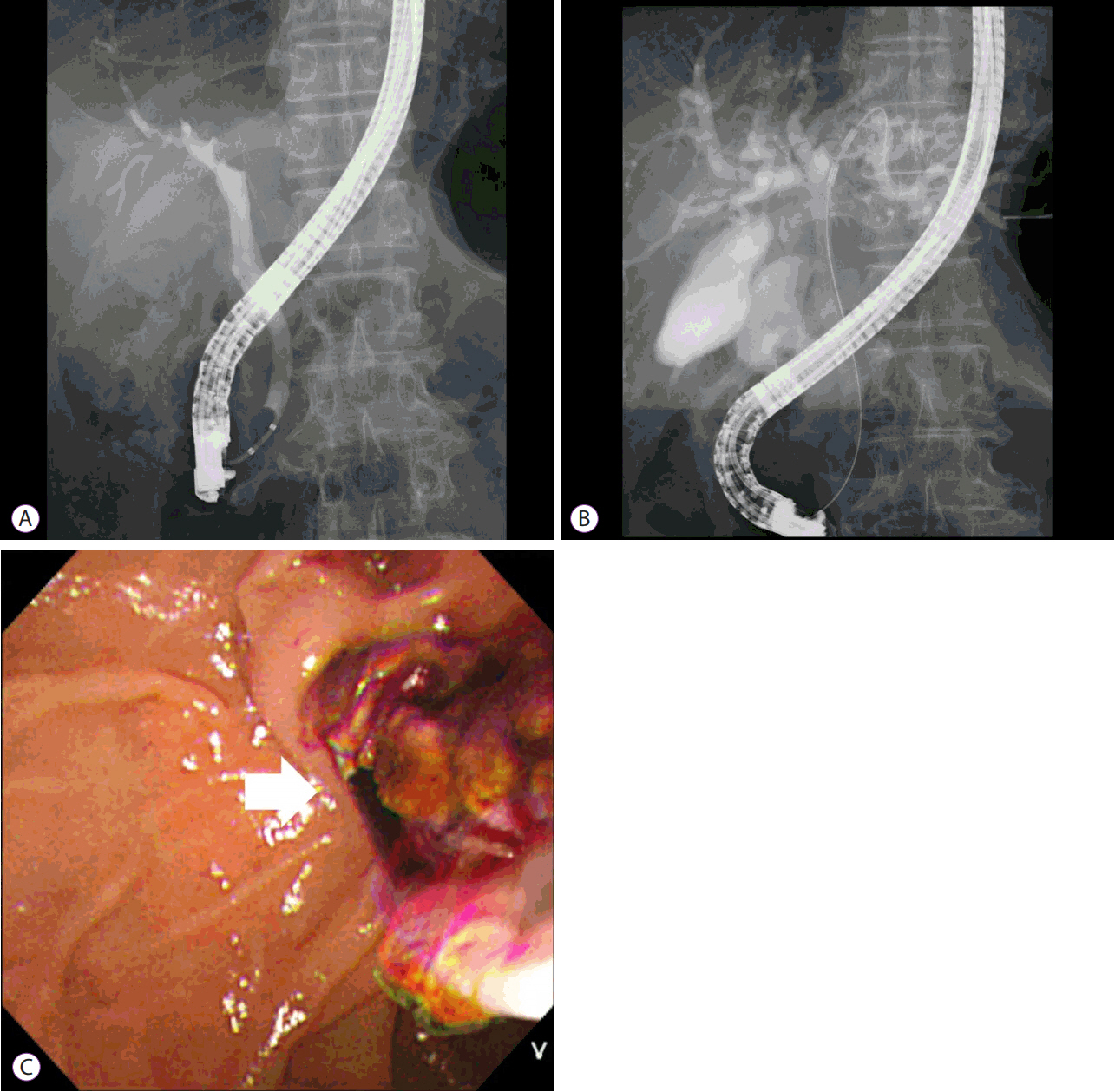
Fig. 2. Endoscopic retrograde cholangiopancreatography (ERCP). (A) ERCP demonstrated left intrahepatic duct obstruction due to the suspicion of an intraductal mass . (B) Intraductal radiofrequency ablation (RFA) was performed at the left proximal intrahepatic duct. (C) The necrotic tissue was removed after intraductal RFA (arrow: necrotic tissue).
Reference
-
1. Garancini M, Goffredo P, Pagni F, et al. Combined hepatocellular-cholangiocarcinoma: a population-level analysis of an uncommon primary liver tumor. Liver Transpl. 2014; 20:952–959.
Article2. Meng KW, Dong M, Zhang WG, Huang QX. Clinical characteristics and surgical prognosis of hepatocellular carcinoma with bile duct invasion. Gastroenterol Res Pract. 2014; 2014:604971.
Article3. Yu XH, Xu LB, Liu C, Zhang R, Wang J. Clinicopathological characteristics of 20 cases of hepatocellular carcinoma with bile duct tumor thrombi. Dig Dis Sci. 2011; 56:252–259.
Article4. Qin LX, Tang ZY. Hepatocellular carcinoma with obstructive jaundice: diagnosis, treatment and prognosis. World J Gastroenterol. 2003; 9:385–391.
Article5. Rustagi T, Jamidar PA. Intraductal radiofrequency ablation for management of malignant biliary obstruction. Dig Dis Sci. 2014; 59:2635–2641.
Article6. Steel AW, Postgate AJ, Khorsandi S, et al. Endoscopically applied radiofrequency ablation appears to be safe in the treatment of malignant biliary obstruction. Gastrointest Endosc. 2011; 73:149–153.
Article7. Dolak W, Schreiber F, Schwaighofer H, et al. Endoscopic radiofrequency ablation for malignant biliary obstruction: a nationwide retrospective study of 84 consecutive applications. Surg Endosc. 2014; 28:854–860.
Article8. Chi M, Mikhitarian K, Shi C, Goff LW. Management of combined hepatocellular-cholangiocarcinoma: a case report and literature review. Gastrointest Cancer Res. 2012; 5:199–202.9. Fujii H, Zhu XG, Matsumoto T, et al. Genetic classification of combined hepatocellular-cholangiocarcinoma. Hum Pathol. 2000; 31:1011–1017.
Article10. Wang J, Wang F, Kessinger A. Outcome of combined hepatocellular and cholangiocarcinoma of the liver. J Oncol. 2010; 2010.
Article11. Kassahun WT, Hauss J. Management of combined hepatocellular and cholangiocarcinoma. Int J Clin Pract. 2008; 62:1271–1278.
Article12. Ortner ME, Caca K, Berr F, et al. Successful photodynamic therapy for nonresectable cholangiocarcinoma: a randomized prospective study. Gastroenterology. 2003; 125:1355–1363.
Article13. Zoepf T, Jakobs R, Arnold JC, Apel D, Riemann JF. Palliation of nonresectable bile duct cancer: improved survival after photodynamic therapy. Am J Gastroenterol. 2005; 100:2426–2430.
Article14. Pereira SP, Aithal GP, Ragunath K, Devlin J, Owen F, Meadows H. Safety and long term efficacy of porfimer sodium photodynamic therapy in locally advanced biliary tract carcinoma. Photodiagnosis Photodyn Ther. 2012; 9:287–292.
Article15. Tal AO, Vermehren J, Friedrich-Rust M, et al. Intraductal endoscopic radiofrequency ablation for the treatment of hilar non-resectable malignant bile duct obstruction. World J Gastrointest Endosc. 2014; 6:13–19.
Article16. Cho JH, Lee KH, Kim JM, Kim YS, Lee DH, Jeong S. Safety and effectiveness of endobiliary radiofrequency ablation according to the different power and target temperature in a swine model. J Gastroenterol Hepatol. 2017; 32:521–526.
Article17. Künzli BM, Abitabile P, Maurer CA. Radiofrequency ablation of liver tumors: actual limitations and potential solutions in the future. World J Hepatol. 2011; 3:8–14.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Comparing palliative treatment options for cholangiocarcinoma: photodynamic therapy vs. radiofrequency ablation
- Extrahepatic Bile Duct Duplication with Intraductal Papillary Neoplasm: A Case Report
- CT feature of bile duct invasion in hepatocellular carcinoma
- A Case of Direct Peroral Cholangioscopy-Guided Intraductal Radiofrequency Ablation for Malignancy Biliary Obstruction via Choledochoduodenostomy Orifice
- Bile Duct Invasion of Hepatocellular Carcinoma
