Entirely Replaced Left Gastric Artery from the Left Hepatic Artery: A Case Report
- Affiliations
-
- 1Department of Radiology, Inje University Ilsan Paik Hospital, Goyang, Korea.
- 2Department of Radiology, Dongsan Medical Center, Keimyung University School of Medicine, Daegu, Korea. sheen@dsmc.or.kr
- KMID: 2410726
- DOI: http://doi.org/10.3348/jksr.2018.78.5.353
Abstract
- Arteries originating from the celiac axis have numerous anatomical variations. When performing interventional and surgical procedures, it is important to be aware of these variations to have better outcomes and to prevent iatrogenic complications. We report on a case of a 62-year-old man who came to our institution to receive transarterial chemoembolization for hepatocellular carcinoma. The computed tomography and angiography revealed a rare anatomic variation: the entire left gastric artery originated from the left hepatic artery with no other accessory feature of the left gastric artery from celiac axis or aorta was seen. To our knowledge, this is the first report on the entirely replaced left gastric artery from the left hepatic artery that was confirmed by utilizing both computed tomographic and angiographic images.
MeSH Terms
Figure
-
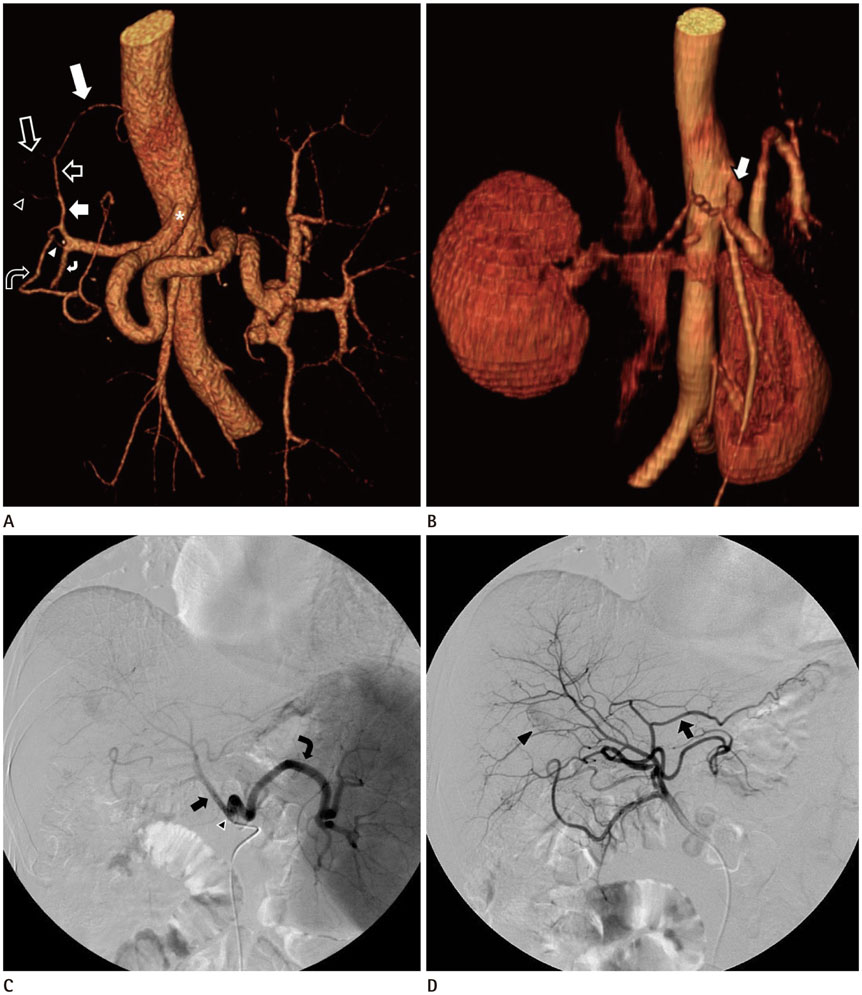
Fig. 1 A 62-year-old male patient with entirely replaced LGA from the LHA, confirmed on liver CT and conventional angiography. A. In a volume-rendering CT angiographic image, the celiac axis (*) bifurcates into the CHA and the splenic artery, and no other feature of the LGA from celiac axis or aorta is seen. After branching of the GDA (white curved arrow) and the RGA (empty curved arrow), the proper hepatic artery (white short arrow) bifurcates into the RHA (empty arrowhead) and LHA (empty short arrow). The LGA (white long arrow) is directly branching from the LHA, and the LHA is continuing its passage (empty long arrow). Note the unusual communication (white arrowhead) between the RGA and the GDA. B. In an initial volume-rendering CT image, the celiac axis (arrow) bifurcates into the CHA and the splenic artery, and no other feature of the LGA from the proximal portion of celiac axis or aorta is visible. C. During the initial TACE, a celiac angiogram shows the CHA (arrow) and splenic artery (curved arrow) are derived from the celiac axis (arrowhead), with no evidence of LGA. D. A subsequent CHA angiogram shows the LGA (arrow) branching from the LHA. A HCC, in segment 6/7 (arrowhead), is noted. CHA = common hepatic artery, CT = computed tomography, GDA = gastroduodenal artery, HCC = hepatocellular carcinoma, LGA = left gastric artery, LHA = left hepatic arter, RGA = right gastric artery, RHA = right hepatic artery, TACE = transarterial chemoembolization
Reference
-
1. Varotti G, Gondolesi GE, Goldman J, Wayne M, Florman SS, Schwartz ME, et al. Anatomic variations in right liver living donors. J Am Coll Surg. 2004; 198:577–582.2. Adachi B. Das Arteriensystem der Japaner. 2nd ed. Tokyo: Kenkyusha Press;1928. p. 11–68.3. Nakamura H, Uchida H, Kuroda C, Yoshioka H, Tokunaga K, Kitatani T, et al. Accessory left gastric artery arising from left hepatic artery: angiographic study. AJR Am J Roentgenol. 1980; 134:529–532.
Article4. Gruttadauria S, Foglieni CS, Doria C, Luca A, Lauro A, Marino IR. The hepatic artery in liver transplantation and surgery: vascular anomalies in 701 cases. Clin Transplant. 2001; 15:359–363.
Article5. Michels NA. Newer anatomy of the liver and its variant blood supply and collateral circulation. Am J Surg. 1966; 112:337–347.
Article6. Naidich JB, Naidich TP, Sprayregen S, Hyman RA, Pudlowski RM, Stein HL. The origin of the left gastric artery. Radiology. 1978; 126:623–626.
Article7. Ishigami K, Yoshimitsu K, Irie H, Tajima T, Asayama Y, Hirakawa M, et al. Accessory left gastric artery from left hepatic artery shown on MDCT and conventional angiography: correlation with CT hepatic arteriography. AJR Am J Roentgenol. 2006; 187:1002–1009.
Article8. Marelli L, Stigliano R, Triantos C, Senzolo M, Cholongitas E, Davies N, et al. Transarterial therapy for hepatocellular carcinoma: which technique is more effective? a systematic review of cohort and randomized studies. Cardiovasc Intervent Radiol. 2007; 30:6–2.
Article9. Kelemouridis V, Athanasoulis CA, Waltman AC. Gastric bleeding sites: an angiographic study. Radiology. 1983; 149:643–648.
Article10. Lang EV, Picus D, Marx MV, Hicks ME, Friedland GW. Massive upper gastrointestinal hemorrhage with normal findings on arteriography: value of prophylactic embolization of the left gastric artery. AJR Am J Roentgenol. 1992; 158:547–549.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Analysis of branching patterns of middle hepatic artery using A-P and oblique view hepatic angiography
- Left Bronchial Artery Arising from a Replaced Left Hepatic Artery in a Patient with Massive Hemoptysis
- Common Hepatic Artery Originating from Left Gastric Artery: A Rare Variant Encountered in Gastric Cancer Surgery
- Normal Variation of Hepatic Artery
- A portal quadrad with triple hepatic arteries
