Left Ventricular Blood Flow Pathways According to the Infarct Location
- Affiliations
-
- 1Department of Internal Medicine, Seoul National University, College of Medicine, Seoul, Korea.
- 2Department of Internal Medicine, Kang Nam General Hospital, Seoul, Korea.
- KMID: 2410455
- DOI: http://doi.org/10.4250/jkse.1994.2.1.13
Abstract
- BACKGROUND
Even after correction for infarct size, there are differences in the survival and the incidence of embolic complication according to infarct location. Blood flow pathway in the left ventricle changes with alteration of left ventricular geometry and this difference in the blood flow pathway might be one of the conceivable causes. Left ventricular blood flow pathway was evaluated using contrast echocardiography. METHOD: Eight Mongrel dogs weighing around 15kg were used. Contrast echocardiography was performed injecting agitated saline in the left atrium in the open chest dogs. Theree aspects were analysed at the baseline and after ligation of coronary arteries −4 in left anterior descending arteries and 4 in left circumflex arteries. 1) left ventricular blood flow pathway during early diastole, 2) persistence of mitral inflow reflected at the left ventricular outflow tract(RMI). 3) Presence of Mitral inflow not reaching the apex and diverted to the left ventricular outflow tract(DMI).
RESULTS
1) Left ventricular blood flow pathway during early diastole. At the baseline(8 cases)-6: centrally directed flow 2: inferiorly directed flow After the infarction(5 cases)-2 anterior infarction : anteriorly directed flow 2 inferior infarction : inferiorly directed flow 1 Iateral infarction : Iaterally directed flow 2) Persistence of RMI. RMI was present at the baseline in 6 cases : RMI was abolished in 2 cases where anterior infarction was induced, RMI persisted in 4 cases where inferior infarction was induced. 3) Presence of DMI. Presence of DMI according to the infarct location could not be evaluated because of the limited number of cases. But in overall cases. before and after the infarction, DMI was present in 7 cases and DMI was absent in 6 cases. DMI(+) group has significantly higher heart rate than DMI(−) group(158.3±17.2 vs 119.5±14.5)(p < 0.05).
CONCLUSION
Blood flow pathway differs according to the infarct location. Blood flow pathway was more similar to the narmal pathway in inferior infarction than anterior infarction. Increase in the heart rate accompanied by left ventricular dysfuction predispose to the diversion of mitral inflow to the left ventricular outflow tract without reaching the apex possibly causing blood stasis at the apex.
MeSH Terms
Figure
-

Fig. 1. A: Mitral inflow–E and A waves were merged (EA) because of the rapid heart rate. B: Mitral inflow wave turing around at the apex and going toward left ventricular outflow(EA').
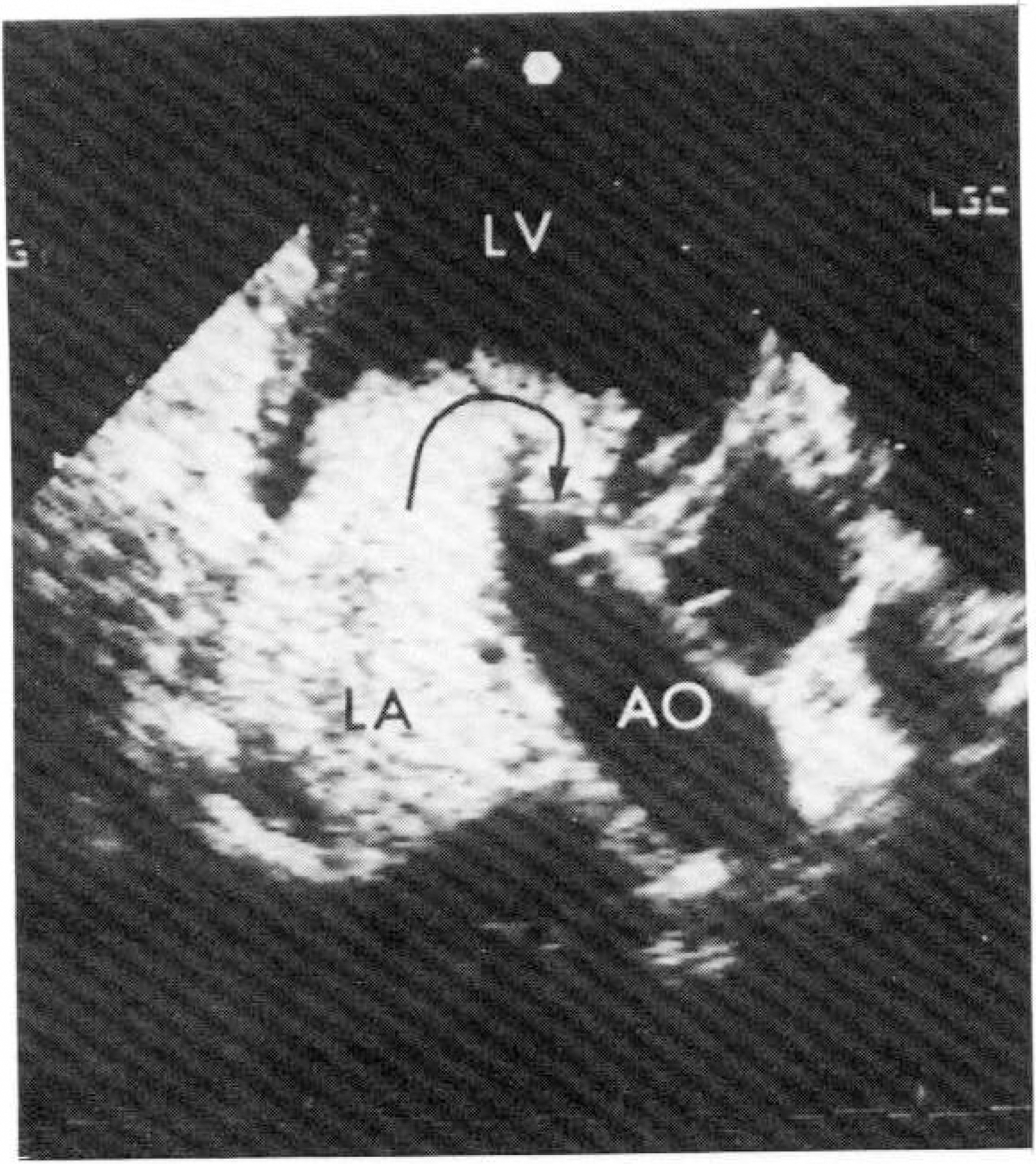
Fig. 2. Mitral inflow not reaching the apex and diverted to the left ventricular outflow.
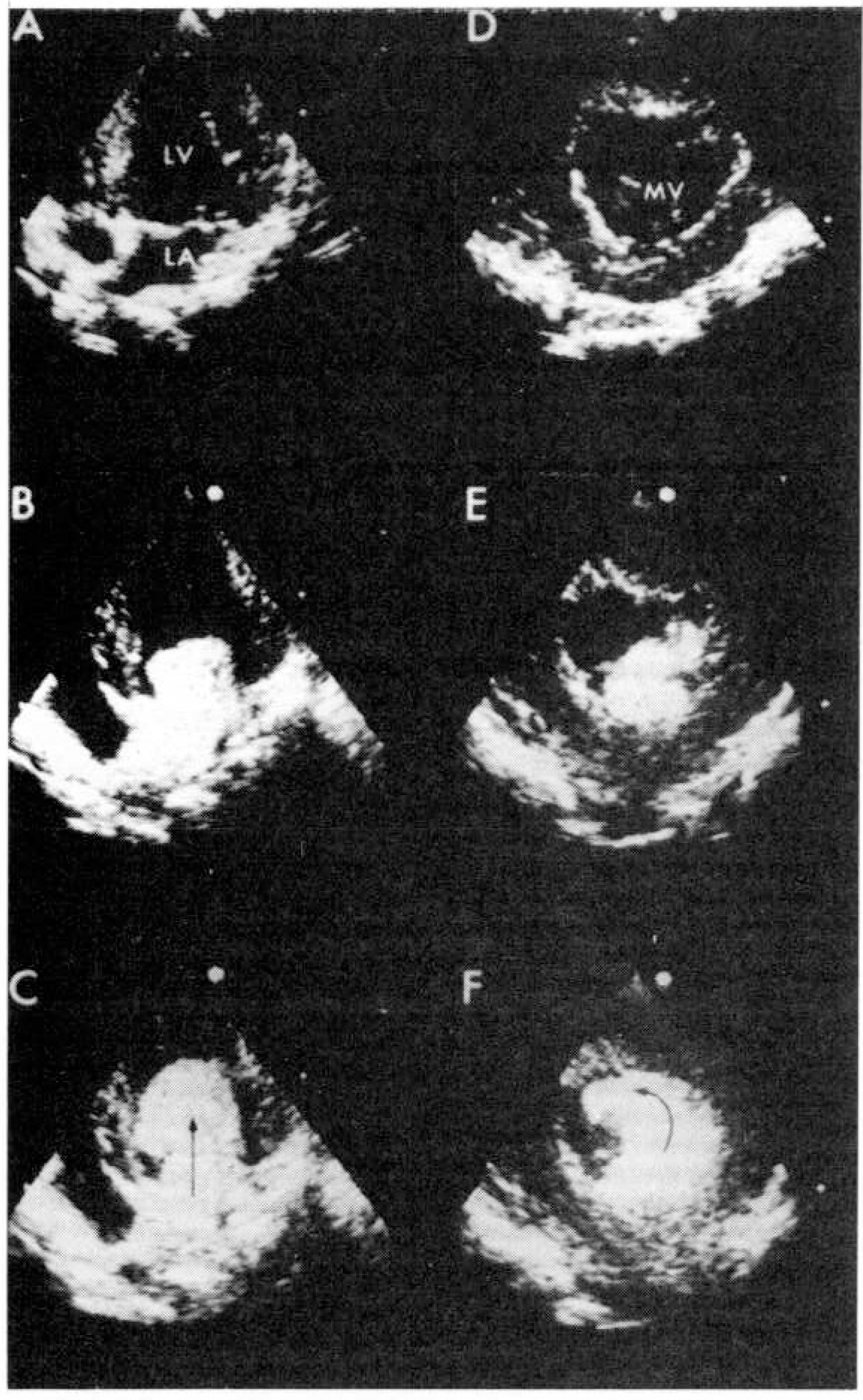
Fig. 3. Normal left ventricular blood flow pathways. A, B, C: Apical 4 chamber view showing centrally directed flow. D, E, F: Parasternal short axis view-In 2 cases initial mitral inflow directed interiorly and turned counterclockwise to the outflow tract.
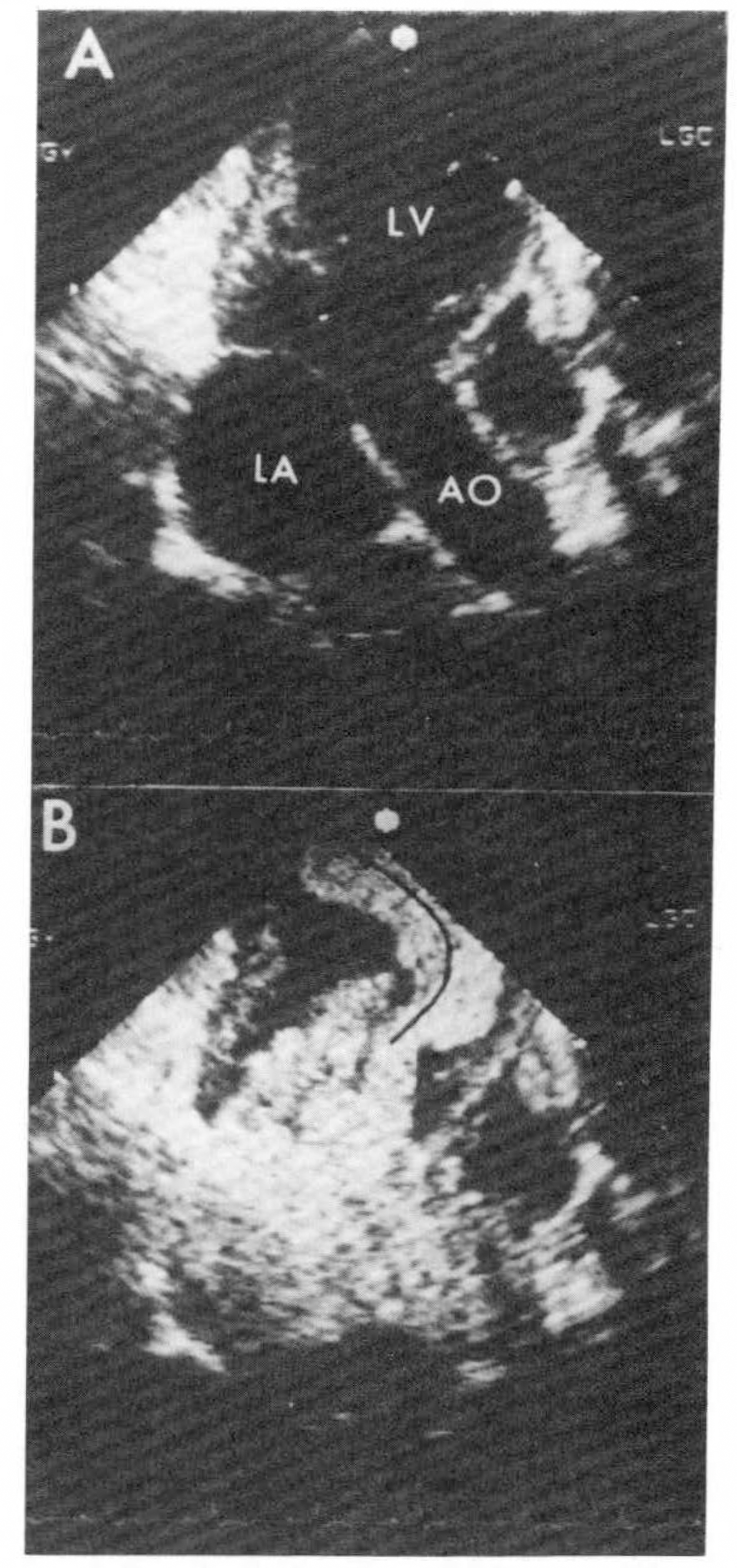
Fig. 4. In anterior infarction mitral inflow was deviated anteriorly and during the following systole turbulance was noted at the center of the cavity.
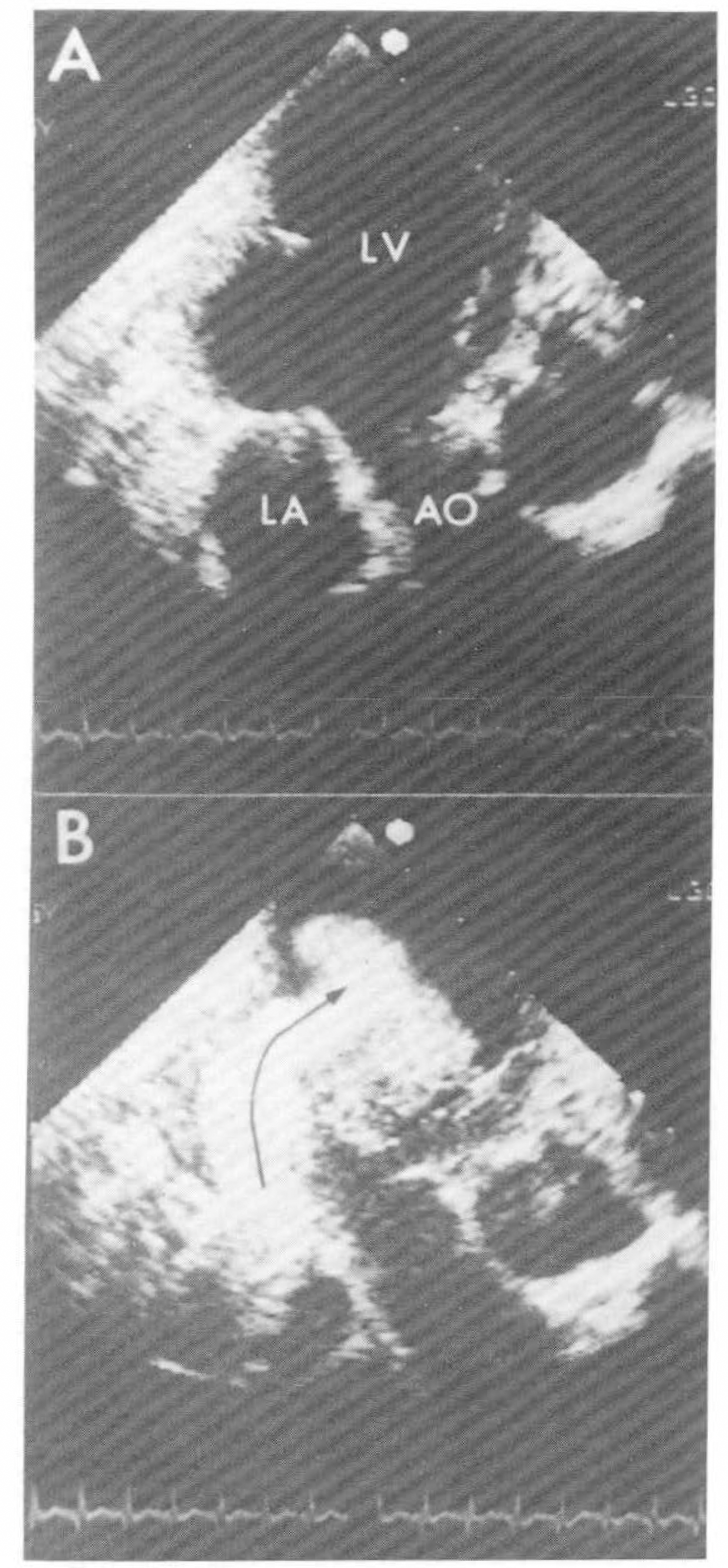
Fig. 5. In inferior infarction. Note the inferiorly deviated mitral inflow.
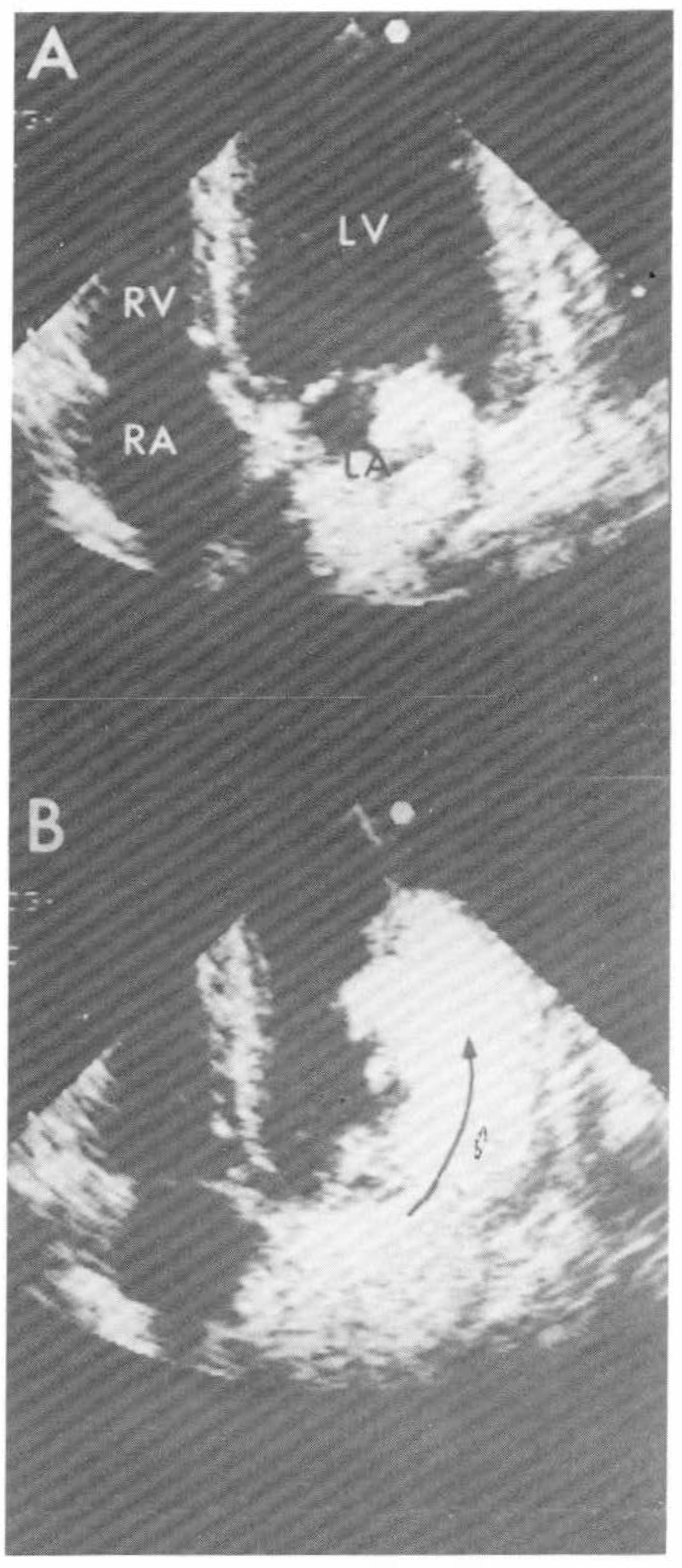
Fig. 6. In lateral infarction. Mitral inflow was deviated laterally.

Fig. 7. Upper panel: In anterior infarction, reflected mitral inflow shown before infarction was abolished after the infarction. Lower panel: Reflected mitral infarction was preserved after the infarction.
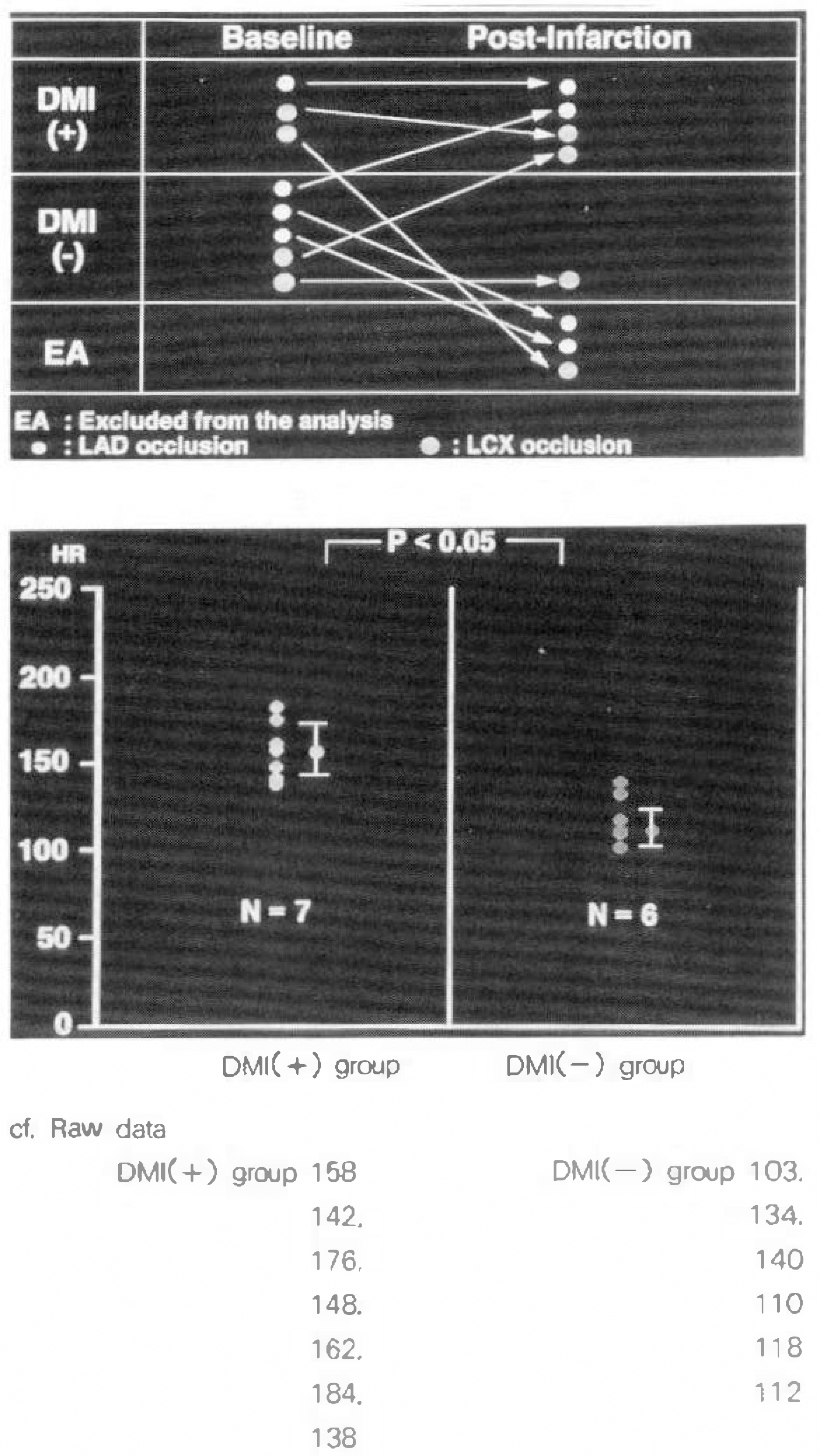
Fig. 8. DMI(+) group showed significantly higher heart rate than DMI(–) group.
Reference
-
References
1). Gruppo Italiano Per Lo Studio Della Streptochinasi Nell'infarcto Miocardico(GISSI). Effectiveness of intravenous thrombolytic treatment in acute myocardial infarction. Lancet. 1:397. 1986.2). TIMI Study Group. Comparison on invasive and conservative strategies following tissue plasminogen activator in acute myocardial infarction: Results of the thrombolysis in myocardial infarction (TIMI-II) trial. N Engl J Med. 320:618. 1989.3). European Cooperative Study Group for Streptokinase Treatment in Acute Myocardial Infarction. Streptokinase in acute myocardial infarction. N Engl J Med. 301:797. 1989.4). Maisel AS, Gilpin E, Holt B, et al. Survival after hospital discharge in matched populations with inferior or anterior myocardial infarction. J Am Coll Cardiol. 6:731. 1985.
Article5). Hans ME, Lloyd BL, Robinson JS, et al. Prognostic significance of electrocardiographic site of infarction after correction for enzymatic size and infarction. Circulation. 73:885. 1986.6). Spirito P, Bellotti P, Chiarella F, et al. Prognostic significance and natural history, of left ventricular thrombi in patients with acute anterior myocardial infarction: A two-dimensional echocardiographic study. Circulation. 72:774. 1985.
Article7). Nihoyannopoulos P, Smith GC, Maseri A, et al. The natural history of left ventricular thrombus in myocardial infarction: A rationale in support of masterly inactivity. J Am Coll Cardiol. 14:903. 1989.
Article8). Jugdutt BI, Sivaram CA. Prospective two-dimensional echocardiographic evaluation of left vetricular thrombus and embolism after acute myocardial infarction. J Am Coll Cardiol. 13:554. 1989.9). Funke Kupper AJ, Verheugt FWA, Peels CH, et al. Left ventricular thrombus incidence and behavior studied by serial two-dimensional echocardiography in acute anterior myocardial infarction: left ventricular wall motion, systemic wall motion, systemic embolism and oral anticoagulation. J Am Coll Cardiol. 13:1514. 1989.10). Keren A, Goldberg S, Gottlieb S, et al. Natural history of left ventricular thrombi: Their appearance and resolution in the posthospitalization period of ac%ute myocardial infarction. J Am Coll Cardiol. 15:790. 1990.
Article11). Wieting DW, Stripling TE. Dynamics and fluid dynamics of the mitral valve. Duran C, Angel WW, Johnson AD, Oury JH, editors. Recent Advances in Mitral Valve Disease. London: Butterworth;p. 13–46. 1984.
Article12). Bellhouse BJ. Fluid mechinics of a model mitral valve. J Physiol. 207:72. 1970.13). Bellhouse BJ. Fluid mechanics of a model mitral valve and left ventricle. Cardiovasc Res. 6:199. 1972.
Article14). Panayiotou H, Byrd BF III. Origin and significance of diastolic doppler flow signals in the left ventricular outflow tract. J Am Coll Cardiol. 16:1625. 1990.
Article15). Beppu S, Izumi S, Miyatake K, et al. Abnormal blood pathways in left ventricular cavity in acute myocardial infarction: experimental observations with special reference to regional wall motion abnormality and hemostasis. Circulation. 78:157. 1988.
Article16). Delemarre BJ, Visser CA, Bot H, et al. Prediction of apical thrombus formation in acute myocardial infarction based on left ventricular spatial flow pattern. J Am Coll Cardiol. 15:355. 1990.
Article17). Marwick TH, Nemec JJ, Pashkow FJ, et al. Accuracy and limitation of exercise chocardiography in a routine clinical setting. J Am Coll Cardiol. 19:74. 1992.18). Feinstein SB, Cheirif J, Ten Cate FJ, et al. Safety and efficacy of a new transpulmonary ultrasound contrast agent: Initial multicenter clinical results. J Am Coll Cardiol. 16:316. 1990.
Article19). Smith MK, Elion JL, McClure RR, et al. Left heart opacification with peripheral venous injection of a new saccharide echo contrast agent in dogs. J Am Coll Cardiol. 13:1622. 1989.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Study for Diastolic Functions in Patients with Early Acute Myocardial Infarction
- The Effect of Sufentanil on Myocardial Function and Coronary Flow in an Isolated-Heart Rat Model
- The Effects of Handgrip and Cold Pressor Test on Mitral Flow in Patients with Left Ventricular Hypertrophy
- Differences in Left and Right Ventricular Function between Different Infarct Sites: An ECG-Gated Blood Pool Study
- Angiographic Findings of Infarct-Related Artery in the Time Course of Myocardial Infarction
