J Korean Soc Echocardiogr.
1994 Dec;2(2):199-208. 10.4250/jkse.1994.2.2.199.
Electrocardiographic Characteristics of Hypertrophic Cardiomyopathy : Echocardiographic and Electrocardiographic Study
- Affiliations
-
- 1Cardiology Division, Yonsei Cardiovascular Center, College of Medicine, Yonsei University, Seoul, Korea.
- KMID: 2410449
- DOI: http://doi.org/10.4250/jkse.1994.2.2.199
Abstract
- BACKGROUND
Patients with hypertrophic cardiomyopathy(HCMP) may present a wide spectrum of electrocardiographic abnormalities. Although many ECG criteria for left ventricular hypertrophy were tried to diagnose HCMP, there is no single criterion which has acceptable sensitivity and specificity. Recently, Allen et al reported that 12 QRS summation criteria was superior to other conventional ECG criteria in HCMP. But the reported sensitivity was relatively low and further study may be warranted. This study examines the relations between the morphology of HCMP and various criteria of left ventricular hypertrophy.
METHODS
1) Study population : Among 18,183 patients who underwent echocardiography from june 1990 to Octover 1993 at Yonsei Cardiovascular Center echocardiography laboratory, 63 patients who were diagnosed as HCMP by two independent echocardiographers were enrolled to study population. All patients with HCMP have at least one segment of left ventricular wall measuring 17mm or more in thickness at end diastole. Each patient had no significant valvular disease and uncontrolled hypertension. We obtained all standard 12 leads ECGs in each 63 patients which was taken within 3 months of echocardiographic examination. 2) The summation of total QRS voltage and depth of T wave inversion in all 12 leads were measured by caliper and the R wave transitional zone in precordial leads was determined by visual estimation. To compare with otehr criteria of left ventricular hypertrophy such as Ramhilt-Estes point score, Sokolow-Lyon index, and RV6 : RV5 ratio, all available data were obtained in all ECGs.
RESULTS
1) Twelve leads QRS voltage summation criteria was the most sensitive to diagnose HCMP comparing with other criteria such as Sokolow-Lyon, RV6 : RV5, and Romhilt-Estes criteria. 2) Modified Romhilt-Estes criteria was equivalently sensitive compared with oter published results. Left atrial enlargement pattern and left axis deviation were more freqently observed in apex-sparing group than apical involved group with statistical significance. 3) The summation of depth of T wave inversion in 12 lead and transitional zone of R wave revealed statistically significant difference between apical involved and apex-sparing groups. 4) The giant T wave inversion was not observed in any patient with obstructive pattern. 5) While Sokolow-Lyon and Romhilt-Estes creteria were not affected by age, sex, and degree of obersity, twelve leads QRS voltage summation criteria and RV6 : RV5(Holt-Spodick) criteria were significantly affected by them.
CONCLUSION
In diagnosing HCMP using electrocardiographic data. 12 lead QRS voltage summation criteria is most sensitive. The depth of T inversion and transitional zone have statistically significant difference between apical involvement and apex sparing HCMP groups. Which may be warranted larger scale study. When diagnosing HCMP with more than moderate degree of hypertrophy, the sensitivities of Sokolow-Lyon criteria and Romhilt-Estes score index were not significantly affected by age, sex, and obesity but those of RV6 : RV5 and 12 lead QRS summation were significantly affected.
MeSH Terms
Figure
-
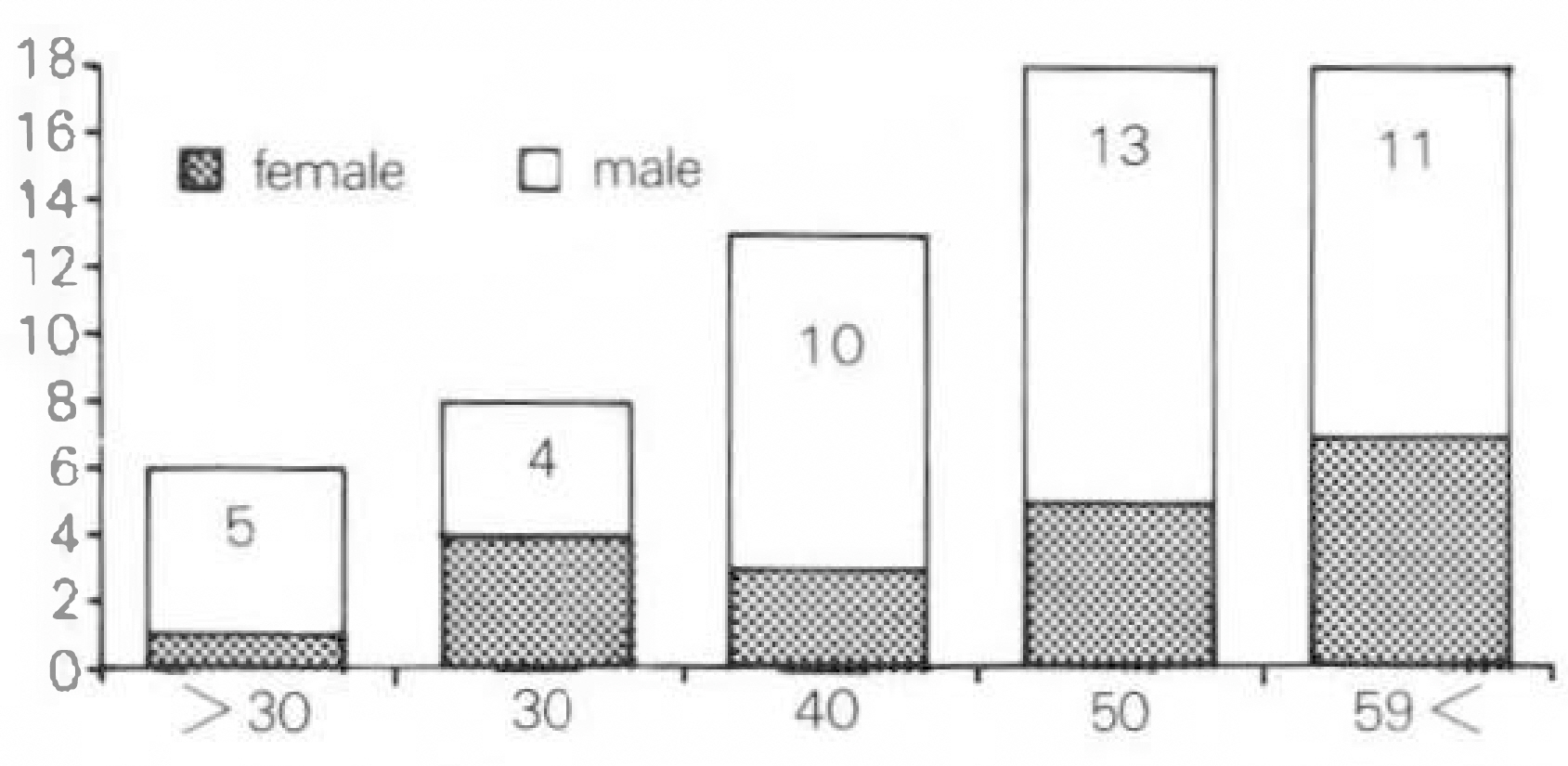
Fig. 1. Age and sex distribution of hypertrophic cardiomyopathy.
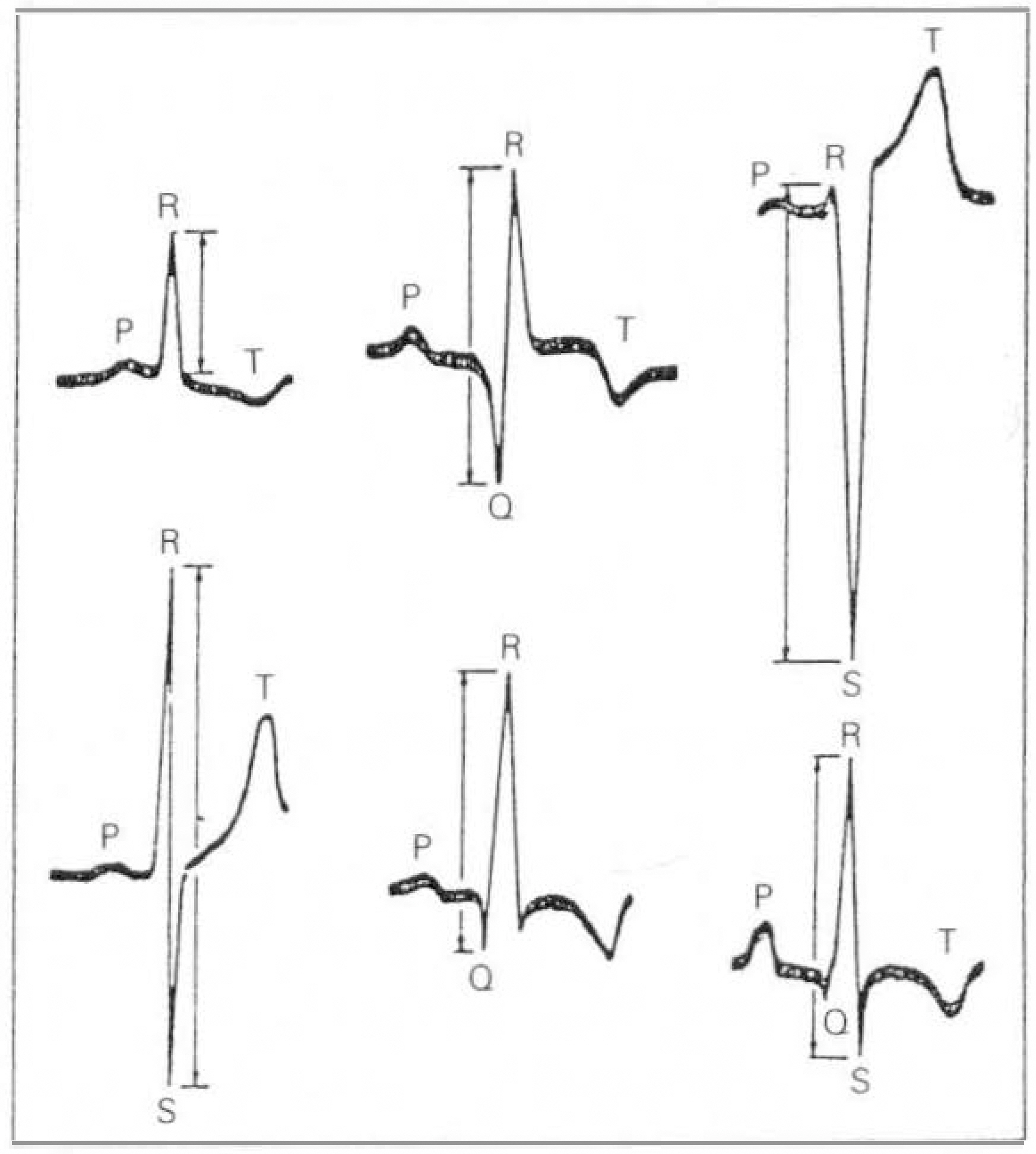
Fig. 2. Various electrocardiographic QRS complexes showing how the voltage(in mm) was measured.
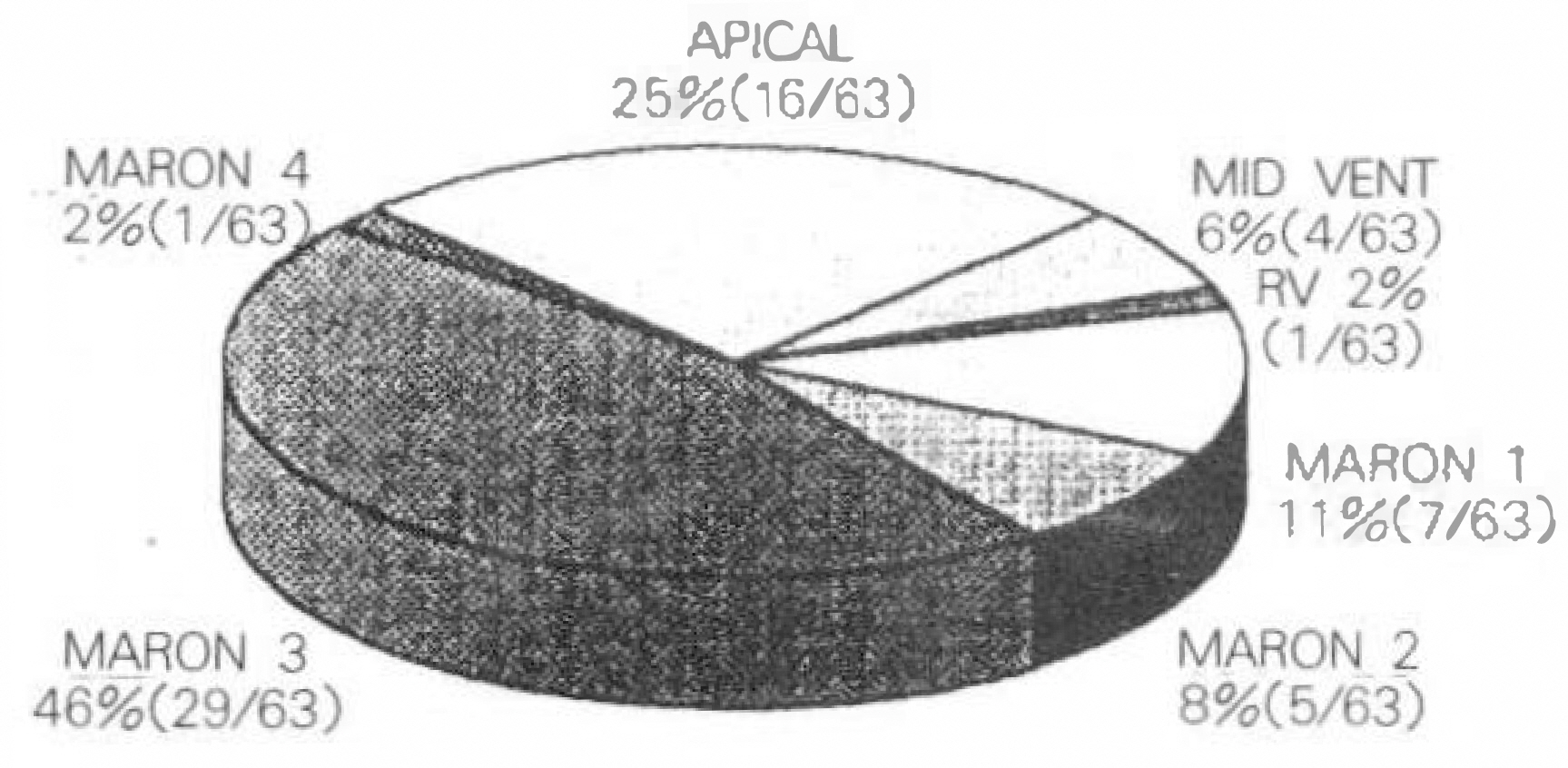
Fig. 3. Distributions of morphological types. APICAL; apical hcmp. MID VENT; mid ventricular hcmp RV; right ventricular hcmp
Reference
-
References
1). Dollar AL, Roberts WC. Usefulness of Total 12-lead QRS Voltage Compared with Other Criteria for Determining Left Ventricular Hypertrophy in Hypertrophic Cardiomyopathy: Analysis of 57 Patients Studied at Necropsy. Am J Med. 87:377. 1989.
Article2). 박창순 • 김유흥 · 박정대 · 장성국 · 박의현 · 이형 우· 채성철 · 전재은· 박회명. 폐쇄성 비후성 심근 증과 심설중격비후를 가진 고혈압성 심장병에서의 심전도학적 차이. 순환기. 18(4):635. 1988.3). Topol EJ, Traill T, Fortuin NJ. Hypertensive hypertrophic cardiomyopathy of the elderly. N Engl J Med. 312:277–283. 1985.
Article4). Sahn DJ, DeMaria A, Kisslo J, Weyman A. The Committee of M-mode standardization of the American Society of Echocardiography: Recommendations Regarding Quantitation in M-Mode Echocardiography: Results of a Survey of Echocardiographic Measurements. Circulation. 58(6):1072. 1978.5). Siegel RJ, Robert WC. Electrocardiographic observations in severe aortic stenosis: correlative necropsy study to clincal hemodynamic, and ECG variables demonstrating relation of 12-lead QRS amplitude to peak systolic transaortic pressure gradient. Am Heart J. 103:210. 1982.6). Maron BJ, Wolfson JK, Ciro E, Spirito P. Relation of electrocardiographic abnormalities and patterns of left ventricular hypertrophy identified by 2-Dimensional Echocardiography in patients with hypertrophic cardiomyopathy. Am J Cardiol. 51:189. 1983.
Article7). Romhilt DW, Estes EH. A point-score system for ECG diagnosis of left ventricular hypertrophy. Am Heart J. 75:752. 1968.8). Koito H, Spodick D. Accuracy of RV6: RV5 voltage ratio for increased left ventricular mass. Am J Cardiol. 62:985. 1988.9). Reichek N, Devereux RB. Left ventricular hypertrophy: relationship of anatomic, echocardiogrphic and electrocardiographic findings. Circulation. 63(6):1391. 1981.10). Devereux RB, Phillips MC, Casale PN, Eisenberg RR, Kligfield P. Geometric determinants of electrocardiographic left ventricular hypertrophy. Circulation. 67(4):907. 1983.
Article11). Woythaler JN, Singer SL, Kwan OL, Meltzer RS, Reubner B, Bommer W, DeMaria A. Accuracy of echocardiography versus electrocardiography in detecting left ventricular hypertrophy: Comparison with postmortem mass measurements. J Am Coll Cardiol. 2(2):305. 1983.
Article12). Levy D, Savage D, Garrison RJ, Anderson KM, Kannel WB, Castelli WP. Echocardiographic criteria for left ventricular hypertrophy: The Framingham heart study. Am J Cardiol. 59:956–960. 1987.
Article13). Casale PN, Devereux RB, Alonso DR, Campo E, Kligfield P. Improved sex-specific criteria of left ventricular hypertrophy for clinical and computer interpretation of electrocardiograms: validation with autopsy findings. Circulation. 75(3):565–572. 1987.
Article14). Levy D, Labib SB, Anderson KM, Christiansen JC, Kannel WB, Castelli WP. Determinants of sensitivity and specificity of electrocardiographic criteria for left ventricular hypertrophy. Circulation. 81:815–820. 1990.
Article15). Padial LR. Usefulness of total 12-lead QRS voltage for determining the presence of left ventricular hypertrophy in systemic hypertension. Am J Cardiol. 68(15):261. 1991.
Article16). Usui M, Inoue H, Suzuki J, Watanabe F, Sugimoto T, Nishikawa J. Relationship between distribution of hypertrophy and electrocardiographic changes in hypertrophic cardiomyopathy. Am Heart J. 126:177–183. 1993.
Article17). Suwa M, Kirota Y, Nakayama Y, Yoenda Y, Kusukawa J, Nakayama A, Kawamura K. Prevalence and clinical significance of development of conduction disturbances in patients with hypertrophic cardiomyopathy. J Cardiol. 19:147–153. 1989; (in Japanese).18). Sugishita Y, Iida K, Matsuda M, Ajisaka R, Ogawa T, Matsumoto R, Fujita T, Ito I, Yamaguchi T. Apical hypertrophy and catecholamines. J Cardiol. 15(supple VI):75. 83, 1985 (in Japanese).19). Nishiyama S, Shiratori K, Nishimura S, Araki R, Takeda K, Nagasaki S, Yamaguchi H, Kuwashima M. Correlation between left ventricular wall thickness and the depth of negative T waves in apical hypertrophic cardiomyopathy. J cardiol. 14:281–288. 1984; (in Japanese).20). Koga Y, Itaya K, Toshima H. Prognosis in hypertrophic cardiomyopathy. Am Heart J. 108:351. 1984.
Article21). Fananapazir L, Chang AC, Epstein SE, McAreavey D. Prognostic Determinants in Hypertrophic Cardiomyopathy: Prospective Evaluation of a Therapeutic Strategy Based on Clinical, Holter, Hemodynamic, and Electrophysiological Findings. Circulation. 86:730–740. 1992.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Left Atrial Enlargement: Echocardiographic Assessment of Electrocardiographic Criteria
- Comparison of ECG Findings between Hypertrophic Obstructive Cardiomyopathy and Hypertension with Disproportionate Septal Thickening
- The Echocardiographic Study on the 13 Patients with the Hypertrophic Cardiomyopathy
- A Case of Normalized Hypertrophic Cardiomyopathy after Removal of Pheochromocytoma
- A Case of Dexamethasone induced Hypertrophic Cardiomyopathy in Neonate with Bronchopulmonary Dysplasia
