Diastolic Function Evaluation in Systemic Arterial Hypertension : A Color M-mode Doppler and Doppler Echocardiographic Analysis
- Affiliations
-
- 1Division of Cardiology, Depertment of Internal Medicine, School of Medicine, Keimyung University, Taegu, Korea.
- KMID: 2410405
- DOI: http://doi.org/10.4250/jkse.1996.4.1.47
Abstract
- BACKGROUND
Several recent studies have demonstrated that left ventricular diastolic dysfunction is major cause of congestive heart failure and may precede systolic dysfunction or without left ventricular hypertrophy in most patients with systemic arterial hypertension. The purpose of this study is to evaluate left ventricular diastolic function in patients with systemic arterial hypertension compared with normal control group using color M-mode Doppler and Doppler echocardiographic studies.
METHODS
From October 1994 to August 1995. 53 patients(18 men and 35 women, mean age : 56.1±12.6 years) with essential hypertension and 30 subjects age-matched nomal controls(13 men and 17 women, mean age 55.9±12.3 years) were included in this study. We measured the early propagation slope of LV inflow by color M-mode Doppler Echocadiography and the peak velocities of E and A wave, E/A tatio, deceleration time of E wave, isovolumic relaxation time by Doppler echocardiography. We also studied left ventricular diastolic function in patients with hypertension who were divided two group(Group I : hypertension with left ventricular hypertrophy, Group II : hypertension without left vetricular hypertrophy).
RESULTS
1) Early propagation slope of LV inflow was significantly decreased in patients with hypertension compared with normal control group(57.43±17.15m/secs vs 69.87±12.71m/secs, p < 0.05). 2) Peak velocity of A wave and isovolumic relaxation time were significantly increased in patients with hypertension compared with normal control group(0.79±0.2m/sec vs 0.69±0.17m/sec, 132.96±36.98m/secs vs 108.67±23.30m/secs, p < 0.05), whereas E/A ratio was significantly decreased in patients with hypertension compared with normal control group(0.96±0.42 vs 1.18±0.43, p < 0.05). Peak velocity of E wave and deceleration time of E wave were not significantly different between in patiens with hypertension and normal contral group, but peak velocity of E wave was showed decreasing tendency in patients with hypertension compared with normal contral group(0.75±0.38m/sec vs 0.77±0.17m/sec, p>0.05), whereas deceleration time of E wave was showed increasing tendency in patients with hypertension empared with normal control group(196.57±37.07m/secs vs 189.33±41.35m/secs, p>0.05). 3) Early propagation slope of LV inflow was not significantly different between Group I and Group II, but showing decreasing tendency in Group I compared with Group II(54.72±14.65m/sec vs 60.16±18.96m/sec, p>0.05). Peak velocity of E wave and peak velocity of A wave and E/A ratio and deceleration time were not significantly different between Group I and Group II but peak velocity of E wave and E/A ratio were showed decreasing tendency in Group I(0.65±0.19m/sec vs 0.73±0.22m/sec, 0.86±040 vs 1.04±0.44, p>0.05), whereas peak velocity of A wave and deceleration time of E wave were showed increasing tendency in Group I(0.80±0.20m/sec vs 0.74±0.18m/sec, 199.38±46.45m/secs vs 196.89±24.76m/secs, p>0.05). Only isovolumic relaxation time was significatly increased in Group I compared with Group II(150.63±44.75m/secs vs 120.34±19.77m/secs, p < 0.05).
CONCLUSION
Left ventricular diastolic dysfunction may precrede systolic or without left ventricular hypertrophy in patients with systemic arterial hypertension. An early diagnosis of left ventricular diastolic dysfunction, color M-mode Doppler echocardiography and Doppler echocardiography were useful diagnostic stools.
MeSH Terms
Figure
-
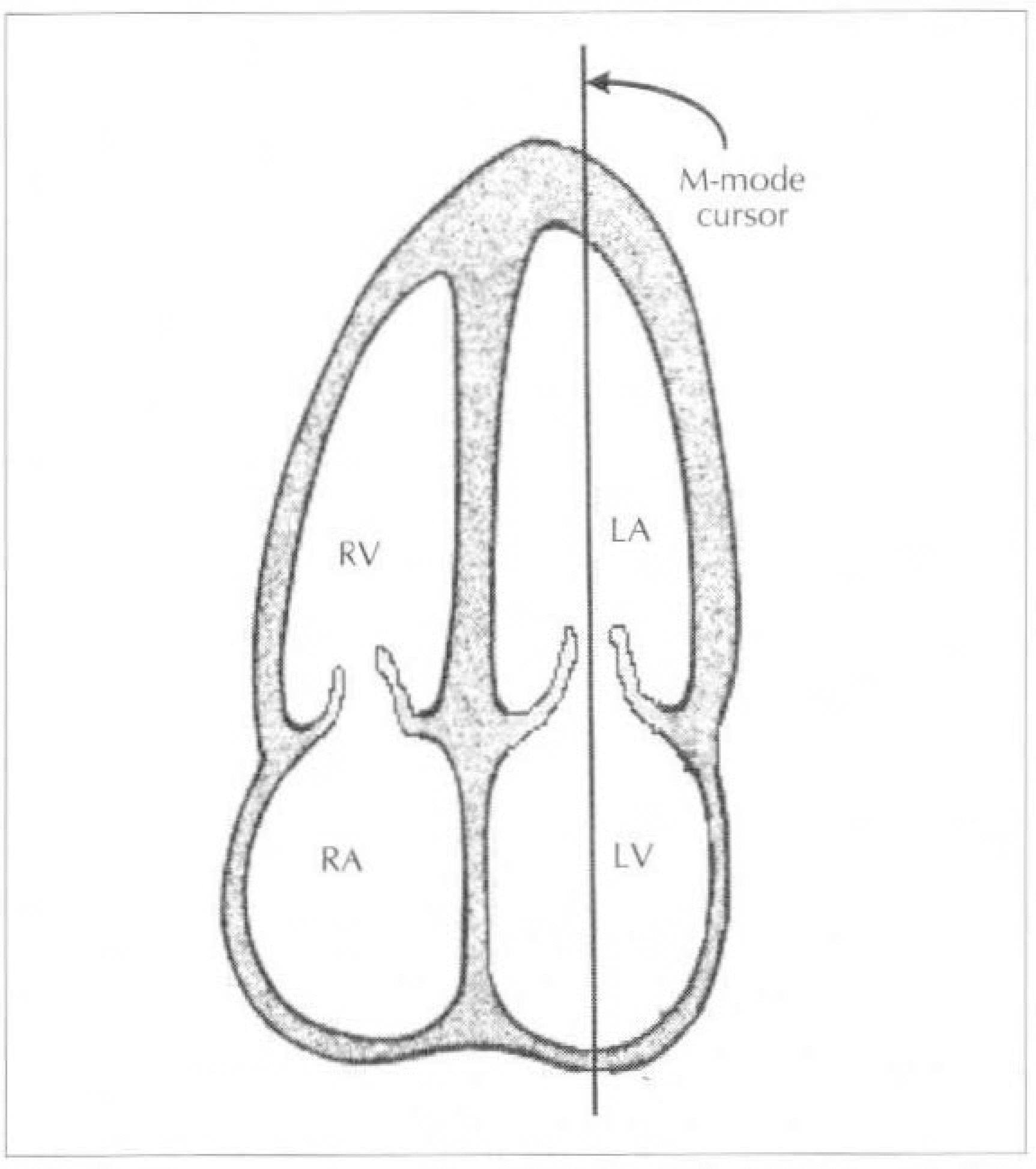
Fig. 1. Shematic illustration of the levels used for analysis of left ventricular filling. The heart was shown in the apical 4-chamber view.
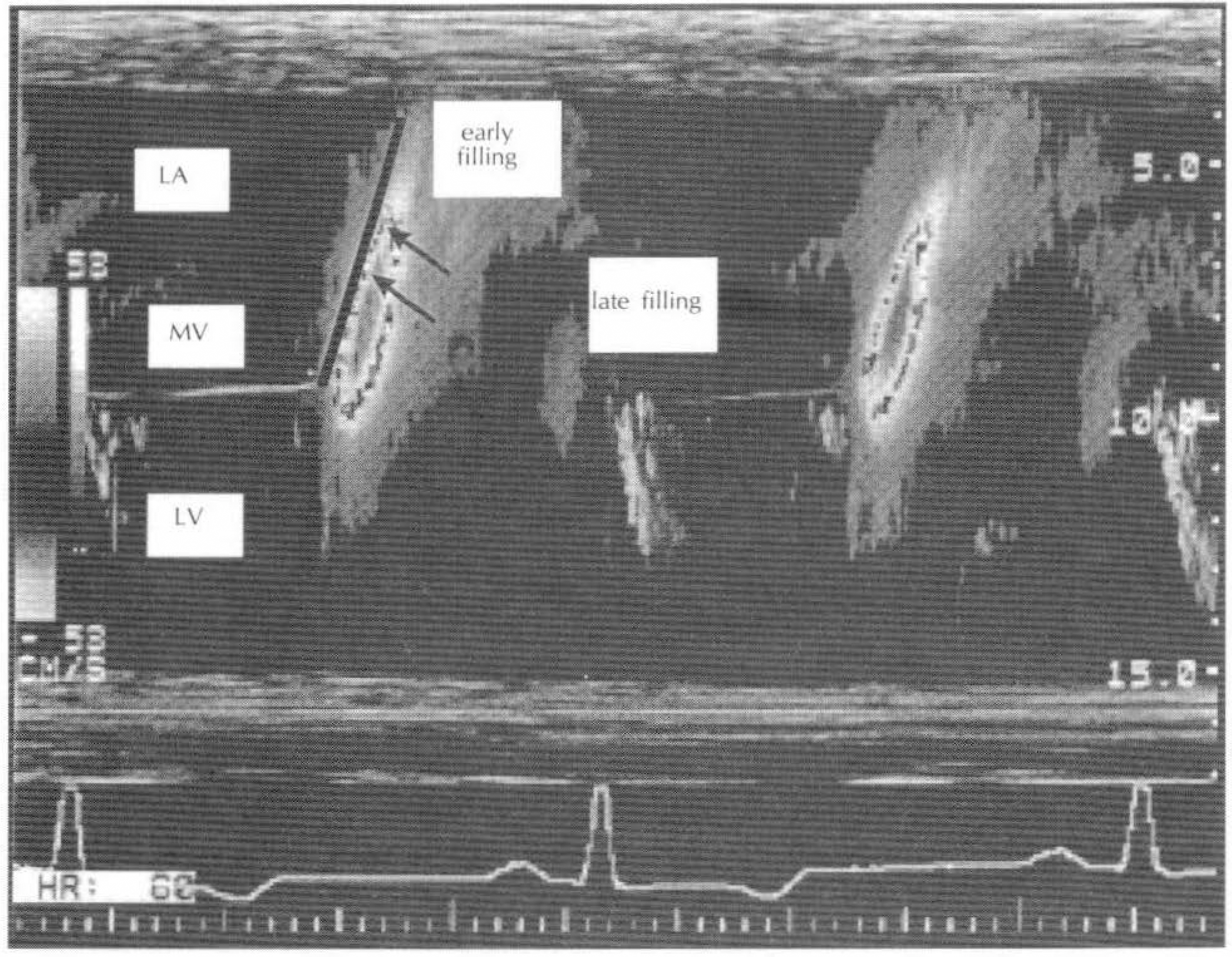
Fig. 2. Early flow propagation slope of LV inflow(arrows) was shown as a linear segment of early filling flow from mitral opeing to LV apical region and was defined as a border of red to yellow color change using color M-mode Doppler echocardiography.
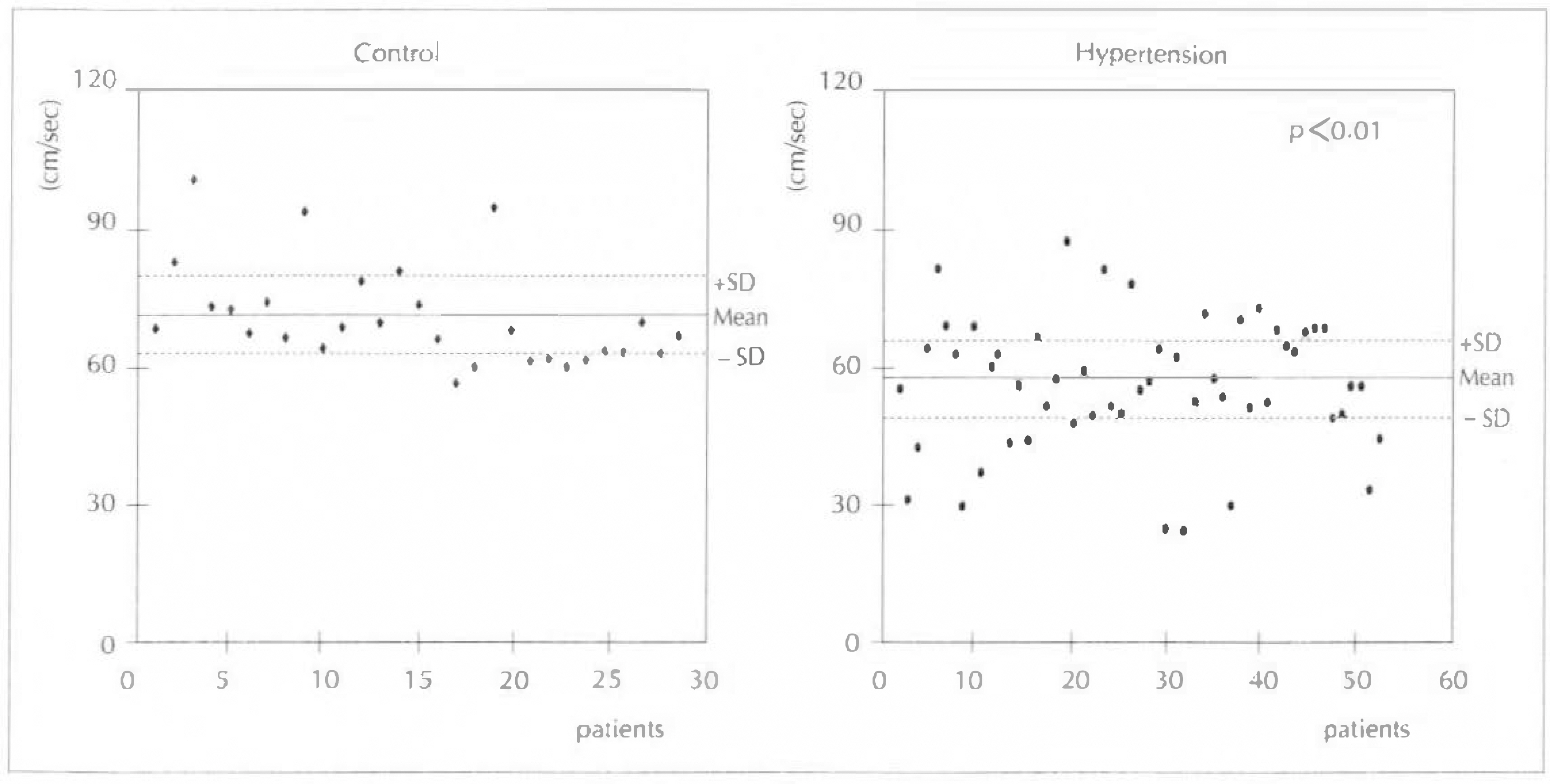
Fig. 3. Comparison of early flow propagation slope of E wave using color M-mode Doppler echocardiography between the patients with hypertension and normal control group.
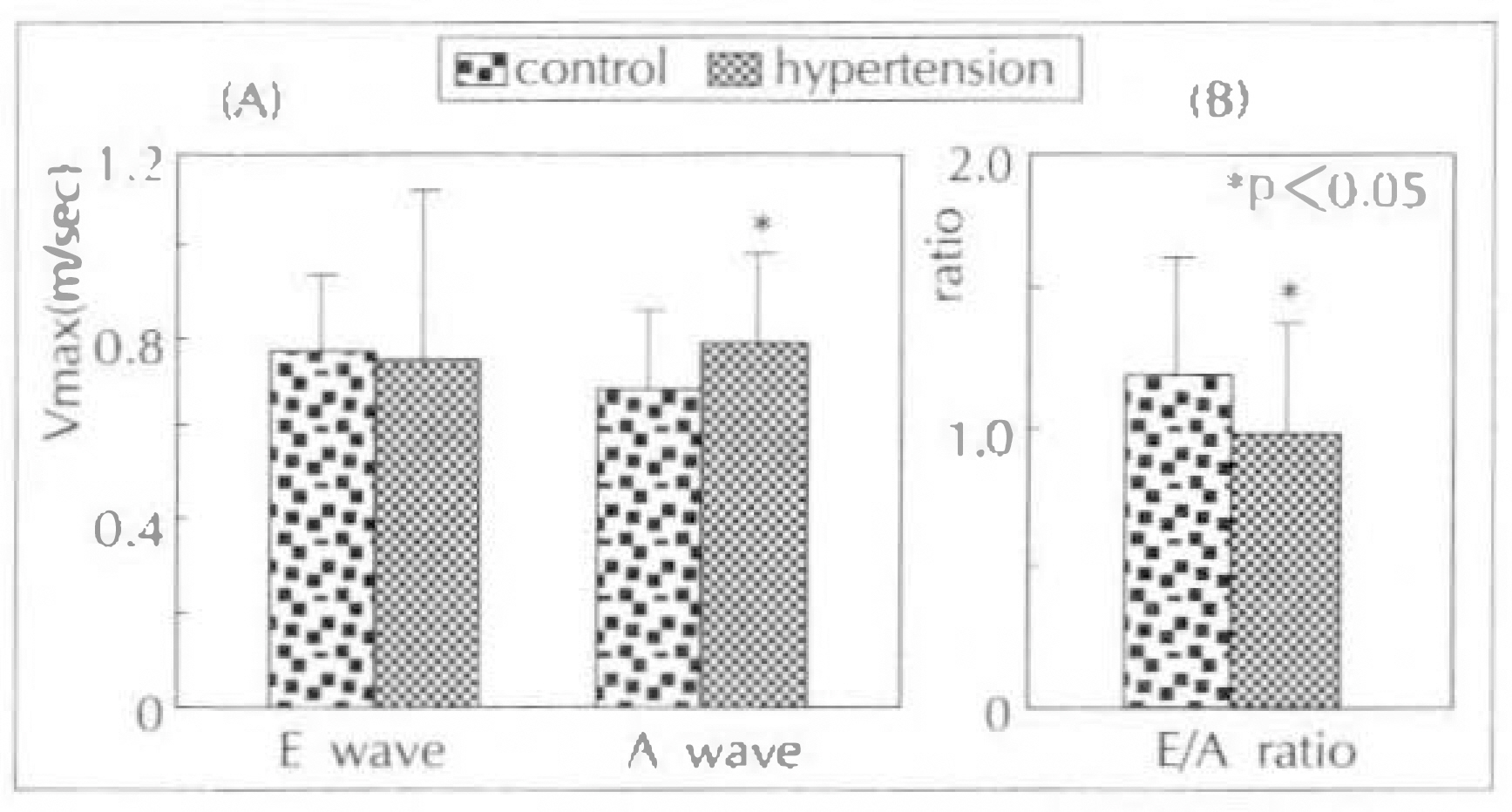
Fig. 4. Comparison of peak velocities(Vmax) of E & A waves(A) and E/A ratio(B) using Doppler echocardiography between the patients with hypertension and normal control group.
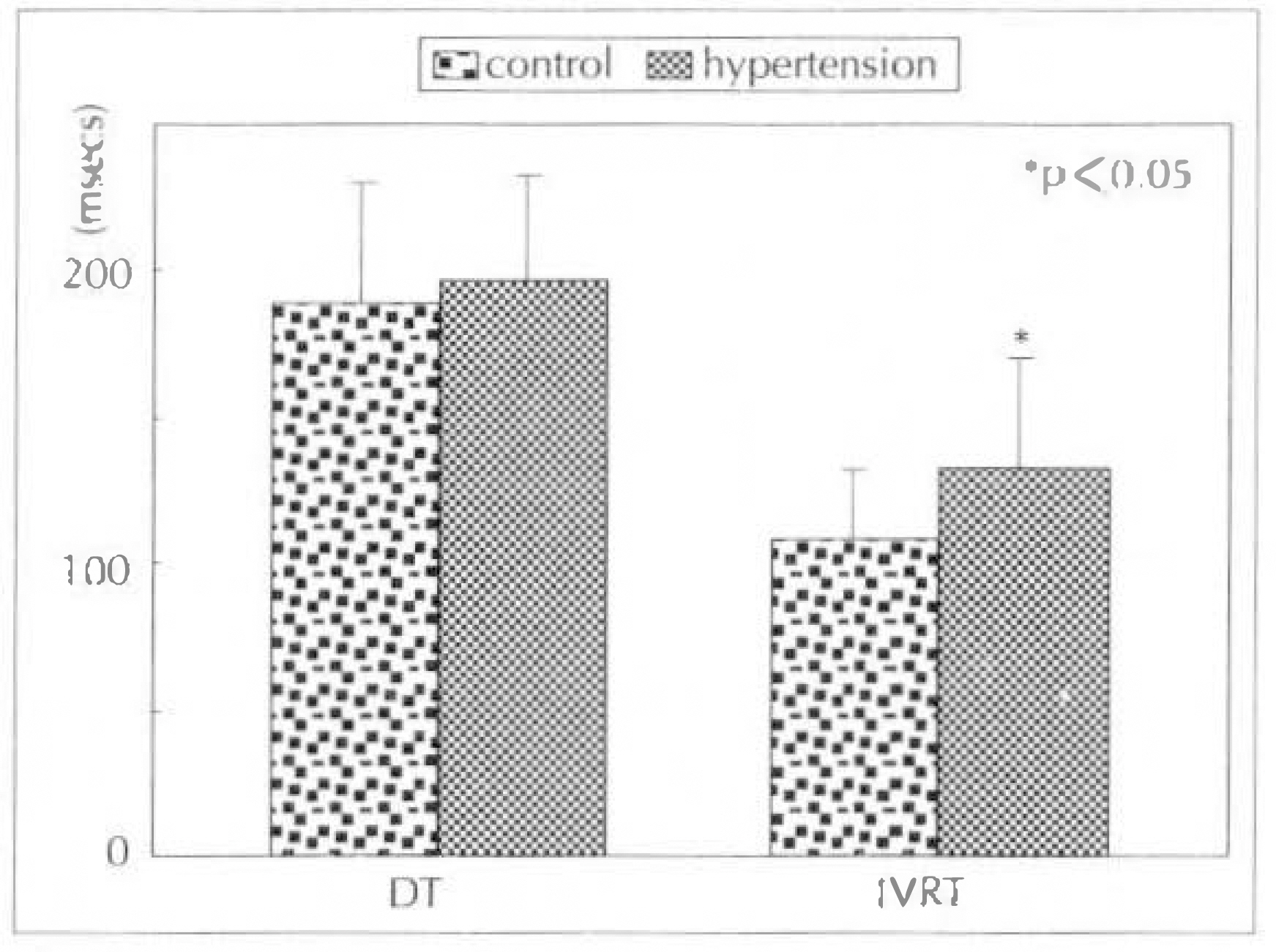
Fig. 5. Comparison of deceleration time(DT) of E wave and isovolumic relaxation time(IVRT) using Doppler echocardiography between the patients with hypertension and normal control group.
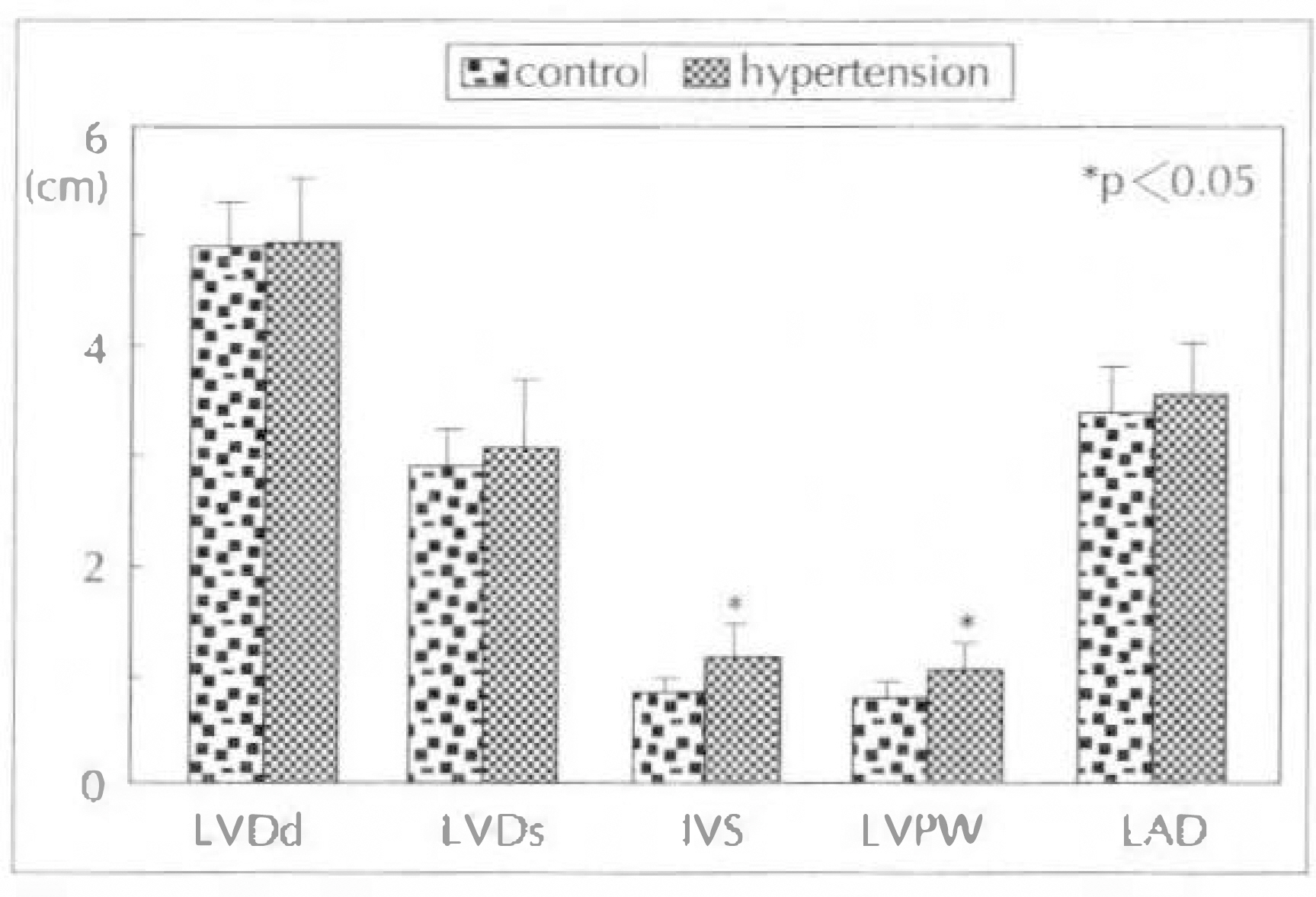
Fig. 6. Comparisom of LV diastolic dimension(LVDd), LV systolic dimension(LVDs), interventricular septum (IVS), LV posterior wall(LVPW) and LA dimension (LAD) using two-dimensional echocardiography between the patients with hypertension and normal control group.
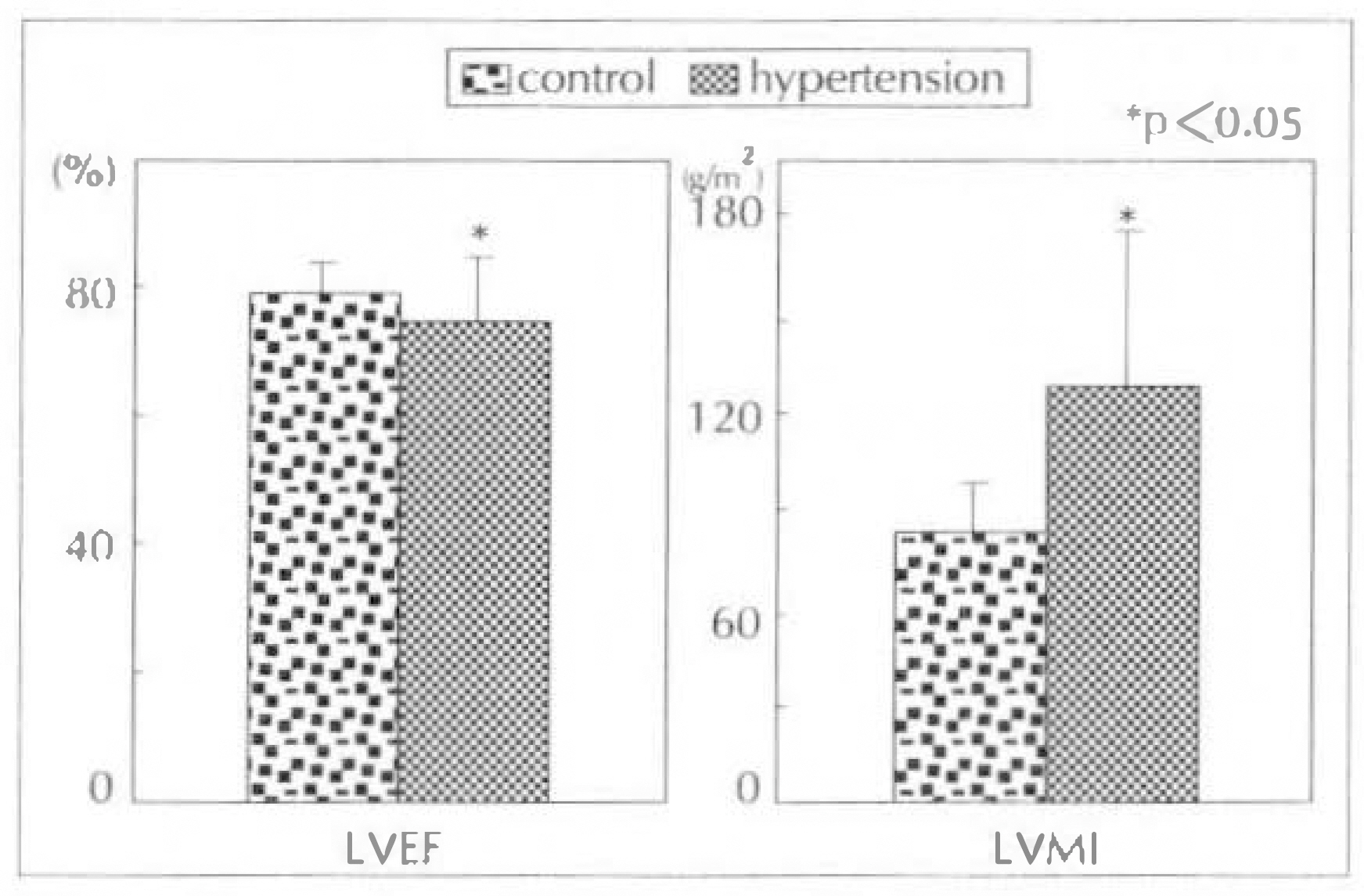
Fig. 7. Comparison of LV ejection fraction(LVEF), LV mass index(LVMI) using two-dimensional echocardiography between the patients with hypertension and normal control group.
Reference
-
References
1). Wever KT, Janicki S. The heart is a muscle-pump system and the concept of heart failure. Am Heart J. 98:371. 1979.2). Liang C, Sherman LG, Doherty JU, Wellington K, Lee VW, Hood WB. Sustained improvement of cardiac function in patients with congestive heart failure after short-term infusion of dobutamine. Circulation. 69:119. 1984.
Article3). Chatterijee K, Parmley WW. Vasodilator therapy in chronic heart failure. Annu Rev Pharmacol Toxicol. 22:475. 1980.4). Gaasch WH, Lewinter MM. Left ventricular diastolic dysfunction and heart failure. 1st Eed. p. 354. Philadelphia: Lea & Febiger Co.;1994.5). Fouad FM, Slominski M, Tarazi RC. Left ventricular diastolic function in hypertension: Relation to left ventricular mass and systolic function. J Am Coll Cardiol. 3:1500. 1984.
Article6). Inouye I, Massie B, Loge D, Topic N, Silverstein D, Simpson P, Tubau J. Abnormal left ventricular filling: An early finding in mild to moderate systemic hypertension. Am J Cardiol. 56:921. 1985.
Article7). Snider AR, Gidding SS, Rocchini AP, Rosenthal A, Dick M 2d, Crowley DC, Peter J. Doppler evaluation of left ventricular diastolic filling in children with systemic hypertension. Am J Cardiol. 56:921. 1985.
Article8). Bonow RO, Bacharach SL, Green MV, Kent KM, Rosing DR, Lipson LC, Leon MB, Epstein SE. Impaired left ventricular diastolic filling in patients with coronary artery disease: Assessment with radionuclide angiography. Circulation. 64:315. 1981.
Article9). Reduto LA, Wickemeyer WJ, Young JB, Del Ventura LA, Reld JW, Glaeser DH, Quinones MA, Miller RR. Left ventricular diastolic performance at rest and during exercise in patients with coronary artery disease. Circulation. 63:1228. 1981.10). Bonow RO, Kent KM, Rosing DR, Lipson LC, Bacharach SL, Green MV, Epstein SE. Improved left ventricular diastolic filling in patients with coronary artery disease after percutaneous transluminal coronary angioplasty. Circulation. 66:1159. 1982.
Article11). Wigle ED, Sasson Z, Henderson MA, Ruddy TD, Fulop J, Rakowski H, Williams WG. Hypertrophic cardiomyopathy: The importance of the site and the extent of hypertrophy. A review Prog Cardiovasc Dis. 3:1500. 1984.12). Brug RJ, Williams GA, Labovitz AJ. Effect of aging on left ventricular diastolic filling in normal subjects. Am J Cardiol. 59:971. 1987.13). Riggs TW, Transue D. Doppler echocardiographic evaluation of left ventricular diastolic function in adolescents with diabetes mellitus. Am J Cardiol. 65:899. 1990.
Article14). Grossman W, McLaurin LP. Diastolic properties of the left ventricle. Ann Intern Med. 84:316. 1976.
Article15). Shah PM, Pai RG. Diastolic heart failure. Curr Probl Cardiol. December 1992.16). Agati L, Fedele F, Penco M, Sciomer S, Dagianti A. Left ventricular filling pattern in hypertensive patients after reversal of myocardial hypertrophy. Int J Cardiol. 17:177. 1987.
Article17). Phillips RA, Coplan NL, Krakoff LR, Yeager K, Ross RS, Gorlin R, Goldman ME. Doppler echocardiographic analysis of left ventricular filling in treated hypertensive patients. J Am Coll Cardiol. 9:317. 1987.18). Kitabatake A, Inoue M, Asao M, Tanouchi J, Masuyama T, Abe H, Morita H, Senda S, Matsuo H. Transmitral blood flow reflecting diastolic behavior of the left ventricle in health and disease: A study by pulsed Doppler technique. Jpn Circ J. 46:92. 1982.
Article19). Genovesi-Ebert A, Marabotti C, Palombo C, Giaconi S, Ghione S. Left ventricular filling: Relationship with arterial blood pressure left ventricualr mass, age, heart rate and body fluid. Hypertension. 9:345. 1991.20). Pearson AC, Labovitz AJ, Mrosek D, Williams GA, Kennedy HL. Assessment of diastolic function in normal and hypertrophied heart: Comparison of Doppler echocardiography and M-mode echocardiography. Am Heart J. 113:1417. 1987.21). Szlachcic J, Tubau JF, O'Kelly B, Massie BM. Correlates of diastolic filling abnormalities in hypertension: A Doppler echocardiographic study. Am Heart J. 120:386. 1990.
Article22). Stugaard M, Smiseth OA, Risce C, Ihlen H. Intraventricular early diastolic filling during acute myocardial ischemia: Assessment by multigated color M-mode Doppler. Circulation. 88:2705. 1993.23). Brun P, Tribouilloy C, Duval AM, Iserin L, Meguira A, Pelle G. Left ventricular flow propagation during early filling is related to wall relaxation: A color M-mode Doppler analysis. J Am Coll Cardiol. 20:420. 1992.
Article24). Stugaard M, Brodahi U, Torp H, Ihlen H. Abnormalities of left ventricular filling in patients with coronary artery disease: Assessment by colour M-mode Doppler. Eur Heart J. 15:318. 1994.25). Stanling MR, Montgomery DG, Mancini GBJ, Walsh RA. Load independence of the rate of isovolumic relaxation in man. Circulation. 76:1274. 1987.
Article26). Varma SK, Owen RM, Smucker ML, Feldman MD. Is a preload independent measure of isovolumetric relaxation? Circulation. 80:1557. 1989.27). Brun P, Tribouilloy C, Dural AM, Iserin L, Meguira A, Pelle G, Dubois-Rande JL. Left ventricular flow propagation during early filling is related to wall relaxation: A color M-mode Doppler analysis. JACC. 20:420. 1992.
Article28). Smith VE, White WB, Karimeddini MF. Echocardiographic assessment of left ventricular diastolic performance in hypertensive subjects: Correlation with changes in left ventricular mass. Hypertension. 9:11–81. 1987.
Article29). Colcun SD, Sander SP, McPherson D, Borow KM. Left ventricular diastolic function in elite athletes with physiologic cardiac hypertrophy. J Am Coll Cardiol. 5:862. 1985.30). Marcus ML, Koyanagi S, Harrison DG, Doty DB, Hiratzka LF, Eastham CL. Abnormalites in coronary circulation secondary to cardiac hypertrophy. Perspect Cardiovasc Res. 8:273. 1983.31). Gelpi RJ, Pasipoularides A, Lader AS, Patrick TA, Chase N, Hittinger L, Shannon RP, Bishop SP, Vatner SF. Changes in diastolic cardiac function in developing and stable perinephritic hypertension in conscious dogs. Circ Res. 68:555. 1991.
Article32). Malholtra A, Penpargkul S, Schaible T, Sheuer J. Contractile proteins and sarcoplasmic reticulum in physiologic cardiac hypertrophy. Am J Physiol. 241:H263. 1981.33). Sordahl LA, McCollum WB, Wood WG, Schwartz A. Mitochondria and sarcoplasmic reticulum function in cardiac hypertrophy and failure. Am J Physiol. 224:497. 1978.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Doppler ultrasonography of the lower extremity arteries: anatomy and scanning guidelines
- The Role of Doppler Time Index for Evaluation of Left Ventricular Diastolic Function by Patterns of Left Ventricular Hypertrophy in Hypertensive Patients
- Color doppler echocardiographic evaluation of residual ductal flow after surgical ligation
- Echocardiographic Diagnosis of Pulmonary Arterial Hypertension in Chronic Lung Disease with Hypoxemia
- Differential Findings of Color M-mode Doppler Echocardiography according to the In-hospital Congestive Heart Failure Following Actue Myocardial Infarction
