The Influence of Pregnancy Disorders Causing Preterm Delivery on In-Hospital Outcomes in Preterm Infants at Less than 32 Weeks of Gestation
- Affiliations
-
- 1Department of Pediatrics, Seoul National University College of Medicine, Seoul, Korea. ljinna@snu.ac.kr
- 2Department of Pediatrics, Seoul National University Hospital, Seoul, Korea.
- 3Department of Pediatrics, Seoul National University Boramae Medical Center, Seoul, Korea.
- 4Department of Biostatistics, Seoul National University Boramae Medical Center, Seoul, Korea.
- 5Department of Pediatrics, Seoul National University Bundang Hospital, Seoul, Korea.
- KMID: 2409118
- DOI: http://doi.org/10.14734/PN.2017.28.4.119
Abstract
OBJECTIVE
We assessed the influence of small for gestational age (GA) with placental disorders (SGA-P) and histologic chorioamnionitis (HCA) on the in-hospital outcomes of preterm infants.
METHODS
Preterm infants with a GA <32 weeks born at Seoul National University Hospital between 2007 and 2014 were included and divided into 4 groups according to the presence of SGA-P and HCA: group 1, SGA-P only; group 2, HCA only; group 3, both SGA-P and HCA; and group 4, no SGA-P or HCA. Multivariate logistic regression was done to compare neonatal outcomes including death, moderate to severe bronchopulmonary dysplasia (BPD) or death, patent ductus arteriosus with treatment, sepsis, necrotizing enterocolitis ≥stage 2b, and intraventricular hemorrhage ≥grade 3.
RESULTS
A total of 572 infants were included. There were 77 patients (13.5%) in group 1, 226 patients (39.5%) in group 2, and 24 patients (4.2%) in group 3. After adjusting for GA, cesarean section, 5 minute Apgar score, multiple pregnancy, premature rupture of membrane before 18 hours prior to delivery, and preeclampsia, group 1 showed higher risks of mortality (adjusted odds ratio [aOR] 3.15, 95% confidence interval [CI] 1.13-8.80), moderate to severe BPD or death (aOR 9.12, 95% CI 3.98-20.90), sepsis (aOR 2.12, CI 1.01-4.46), and pulmonary hypertension (aOR 3.26, 95% CI 1.15-9.22) compared with group 4. There were no significant differences in mortality and in-hospital outcomes between groups 2 and 4 or between groups 3 and 4.
CONCLUSION
Close monitoring and early intervention are suggested in SGA-P infants.
Keyword
MeSH Terms
-
Apgar Score
Bronchopulmonary Dysplasia
Cesarean Section
Chorioamnionitis
Ductus Arteriosus, Patent
Early Intervention (Education)
Enterocolitis, Necrotizing
Female
Fetal Growth Retardation
Gestational Age
Hemorrhage
Humans
Hypertension, Pulmonary
Infant
Infant, Newborn
Infant, Premature*
Logistic Models
Membranes
Mortality
Odds Ratio
Patient Outcome Assessment
Placenta Diseases
Pre-Eclampsia
Pregnancy*
Pregnancy, Multiple
Rupture
Seoul
Sepsis
Figure
-
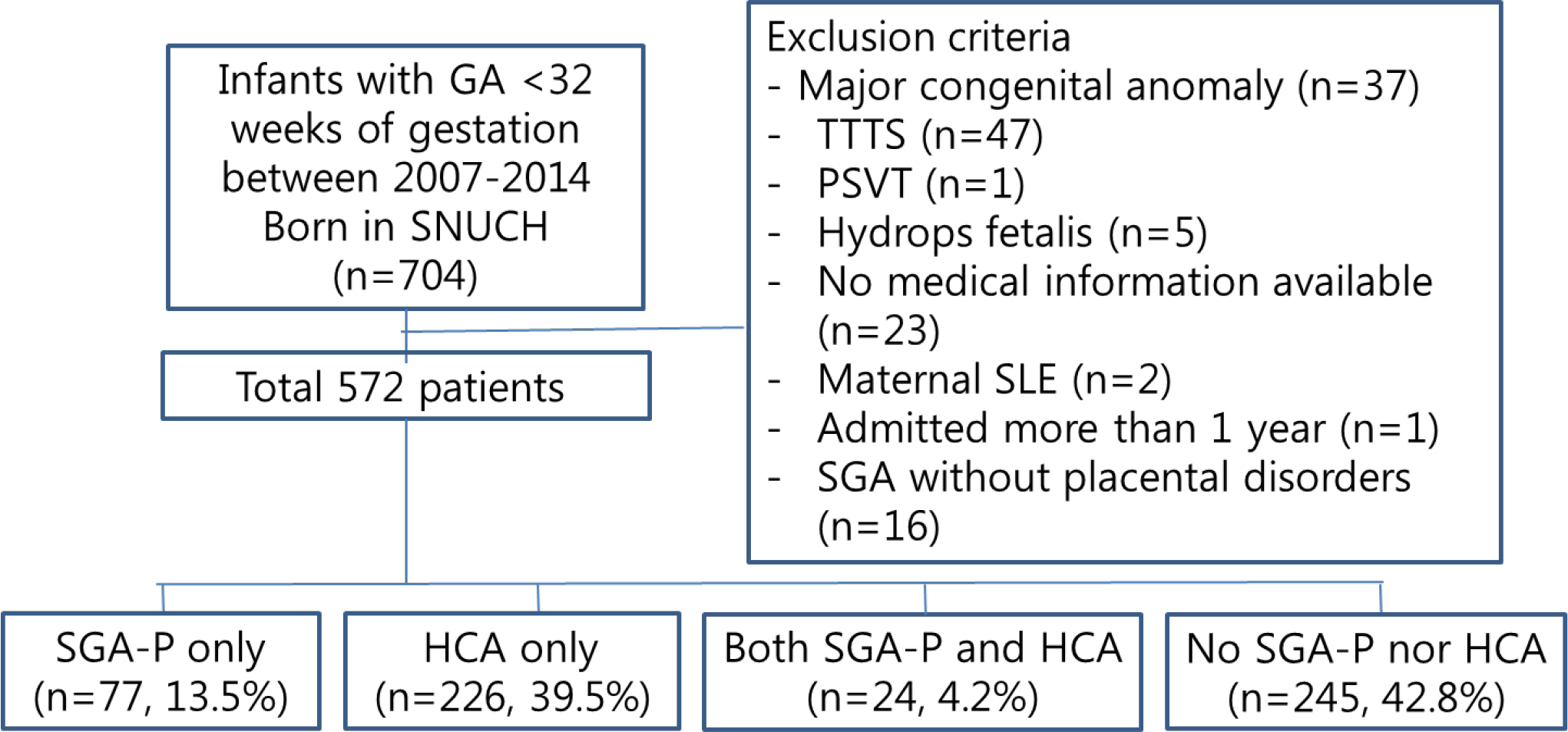
Fig. 1 Flow chart of the study population. A total of 572 patients with <32 weeks of gestation born between 2007 and 2014 were included in the analysis. 77 patients (13.5%) were in group 1, 226 patients (39.5%) were in group 2, and 24 patients (4.2%) were in group 3. GA, gestational age; SNUCH, Seoul National University Children's Hospital; TTTS, twin to twin transfusion syndrome; PSVT, paroxysmal supraventricular tachycardia; SLE, systemic lupus erythematosus; SGA-P; small for gestational age with placental disorders; HCA, histologic chorioamnionitis.

Fig. 2 The proportion of 4 groups according to the gestational age at birth. The percentage of histologic chorioamnionitis group was decreased and the percentage of small for gestational age with placental disorders was increased as the gestational age gets older (P=0.045). SGA-P, small for gestational age with placental disorders; HCA, histologic chorioamnionitis.
Reference
-
1). Gagliardi L., Rusconi F., Da Frè M., Mello G., Carnielli V., Di Lallo D, et al. Pregnancy disorders leading to very preterm birth influence neonatal outcomes: results of the population-based ACTION cohort study. Pediatr Res. 2013. 73:794–801.
Article2). McElrath TF., Hecht JL., Dammann O., Boggess K., Onderdonk A., Marken-son G, et al. Pregnancy disorders that lead to delivery before the 28th week of gestation: an epidemiologic approach to classification. Am J Epidemiol. 2008. 168:980–9.
Article3). Klebanoff MA., Shiono PH. Top down, bottom up and inside out: reflections on preterm birth. Paediatr Perinat Epidemiol. 1995. 9:125–9.4). Monier I., Ancel PY., Ego A., Jarreau PH., Lebeaux C., Kaminski M, et al. Fetal and neonatal outcomes of preterm infants born before 32 weeks of gestation according to antenatal vs postnatal assessments of restricted growth. Am J Obstet Gynecol. 2017. 216:516. .e1-516.e10.5). Giapros V., Drougia A., Krallis N., Theocharis P., Andronikou S. Morbidity and mortality patterns in small-for-gestational age infants born pre-term. J Matern Fetal Neonatal Med. 2012. 25:153–7.
Article6). Lee HJ., Kim EK., Kim HS., Choi CW., Kim BI., Choi JH. Chorioamnionitis, respiratory distress syndrome and bronchopulmonary dysplasia in extremely low birth weight infants. J Perinatol. 2011. 31:166–70.
Article7). Hartling L., Liang Y., Lacaze-Masmonteil T. Chorioamnionitis as a risk factor for bronchopulmonary dysplasia: a systematic review and meta-analysis. Arch Dis Child Fetal Neonatal Ed. 2012. 97:F8–17.
Article8). Kim SY., Choi CW., Jung E., Lee J., Lee JA., Kim H, et al. Neonatal morbidities associated with histologic chorioamnionitis defined based on the site and extent of inflammation in very low birth weight infants. J Korean Med Sci. 2015. 30:1476–82.
Article9). Hendson L., Russell L., Robertson CM., Liang Y., Chen Y., Abdalla A, et al. Neonatal and neurodevelopmental outcomes of very low birth weight infants with histologic chorioamnionitis. J Pediatr. 2011. 158:397–402.
Article10). Olsen IE., Groveman SA., Lawson ML., Clark RH., Zemel BS. New intrauterine growth curves based on United States data. Pediatrics. 2010. 125:e214–24.
Article11). Salafia CM., Weigl C., Silberman L. The prevalence and distribution of acute placental inflammation in uncomplicated term pregnancies. Obstet Gynecol. 1989. 73(3 Pt 1):383–9.
Article12). Kim SY., Shin SH., Kim HS., Jung YH., Kim EK., Choi JH. Pulmonary arterial hypertension after ibuprofen treatment for patent ductus arteriosus in very low birth weight infants. J Pediatr. 2016. 179:49–53. .e1.
Article13). Papile LA., Burstein J., Burstein R., Koffler H. Incidence and evolution of subependymal and intraventricular hemorrhage: a study of infants with birth weights less than 1,500 gm. J Pediatr. 1978. 92:529–34.
Article14). Bell MJ., Ternberg JL., Feigin RD., Keating JP., Marshall R., Barton L, et al. Neonatal necrotizing enterocolitis. Therapeutic decisions based upon clinical staging. Ann Surg. 1978. 187:1–7.15). Nobile S., Marchionni P., Carnielli VP. Neonatal outcome of small for gestational age preterm infants. Eur J Pediatr. 2017. 176:1083–8.
Article16). Vayssière C., Sentilhes L., Ego A., Bernard C., Cambourieu D., Flamant C, et al. Fetal growth restriction and intrauterine growth restriction: guidelines for clinical practice from the French college of gynaecologists and obstetricians. Eur J Obstet Gynecol Reprod Biol. 2015. 193:10–8.
Article17). Eriksson L., Haglund B., Odlind V., Altman M., Ewald U., Kieler H. Perinatal conditions related to growth restriction and inflammation are associated with an increased risk of bronchopulmonary dysplasia. Acta Paediatr. 2015. 104:259–63.
Article18). DiGiulio DB., Gervasi MT., Romero R., Vaisbuch E., Mazaki-Tovi S., Kusanovic JP, et al. Microbial invasion of the amniotic cavity in pregnancies with small-for-gestational-age fetuses. J Perinat Med. 2010. 38:495–502.
Article19). De Wolf F., Brosens I., Renaer M. Fetal growth retardation and the maternal arterial supply of the human placenta in the absence of sustained hypertension. Br J Obstet Gynaecol. 1980. 87:678–85.20). The Executive Committee of Korean Neonatal Network. 2015 Korean Neonatal Network Annual Report. Cheongwon: Korean Centers for Disease Control and Prevention;2016.21). Pugni L., Pietrasanta C., Acaia B., Merlo D., Ronchi A., Ossola MW, et al. Chorioamnionitis and neonatal outcome in preterm infants: a clinical overview. J Matern Fetal Neonatal Med. 2016. 29:1525–9.
Article22). Lee SY., Leung CW. Histological chorioamnionitis-implication for bacterial colonization, laboratory markers of infection, and early onset sepsis in very-low-birth-weight neonates. J Matern Fetal Neonatal Med. 2012. 25:364–8.23). Ylijoki M., Lehtonen L., Lind A., Ekholm E., Lapinleimu H., Kujari H, et al. Chorioamnionitis and five-year neurodevelopmental outcome in pre-term infants. Neonatology. 2016. 110:286–95.
Article24). Kramer BW., Kallapur S., Newnham J., Jobe AH. Prenatal inflammation and lung development. Semin Fetal Neonatal Med. 2009. 14:2–7.
Article25). Tröger B., Göpel W., Faust K., Müller T., Jorch G., Felderhoff-Müser U, et al. Risk for late-onset blood-culture proven sepsis in very-low-birth weight infants born small for gestational age: a large multicenter study from the German Neonatal Network. Pediatr Infect Dis J. 2014. 33:238–43.26). Xanthou M. Immunologic deficiencies in small-for-dates neonates. Acta Paediatr Scand Suppl. 1985. 319:143–9.
Article27). Tröger B., Müller T., Faust K., Bendiks M., Bohlmann MK., Thonnissen S, et al. Intrauterine growth restriction and the innate immune system in preterm infants of </=32 weeks gestation. Neonatology. 2013. 103:199–204.28). Mirza H., Ziegler J., Ford S., Padbury J., Tucker R., Laptook A. Pulmonary hypertension in preterm infants: prevalence and association with bronchopulmonary dysplasia. J Pediatr. 2014. 165:909–14. .e1.
Article29). Mestan KK., Check J., Minturn L., Yallapragada S., Farrow KN., Liu X, et al. Placental pathologic changes of maternal vascular underperfusion in bronchopulmonary dysplasia and pulmonary hypertension. Placenta. 2014. 35:570–4.
Article30). Nagiub M., Kanaan U., Simon D., Guglani L. Risk factors for development of pulmonary hypertension in infants with bronchopulmonary dysplasia: systematic review and meta-analysis. Paediatr Respir Rev. 2017. 23:27–32.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Evaluation of Preterm Delivery between 32(+0)-33(+6) Weeks of Gestation
- The Effects of Incomplete Antenatal Corticosteroid Therapy Prior to Delivery on Clinical Outcomes of Preterm Infants
- Neonatal outcomes of very low birthweight infants from spontaneous and indicated preterm delivery
- Effects of Stressed Pregnancies on Preterm Neonatal Outcomes
- Epidemiologic Study of Preterm Birth in Chosun University Hospital
