Ann Hepatobiliary Pancreat Surg.
2018 Feb;22(1):36-41. 10.14701/ahbps.2018.22.1.36.
Management of residual gall bladder: A 15-year experience from a north Indian tertiary care centre
- Affiliations
-
- 1Department of Surgical Gastroenterology, Sanjay Gandhi Post Graduate Institute of Medical Sciences (SGPGIMS), Lucknow, India. rajneeshkumarsingh@hotmail.com
- KMID: 2409078
- DOI: http://doi.org/10.14701/ahbps.2018.22.1.36
Abstract
- BACKGROUNDS/AIMS
A residual gallbladder (RGB) following a partial/subtotal cholecystectomy may cause symptoms that require its removal. We present our large study regarding the problem of a RGB over a 15 year period.
METHODS
This study involved a retrospective analysis of patients managed for symptomatic RGB from January 2000 to December 2015.
RESULTS
A RGB was observed in 93 patients, who had a median age of 45 (25-70) years, and were comprised of 69 (74.2%) females. The most common presentation was recurrence pain (n=64, 68.8%). Associated choledocholithiasis was present in 23 patients (24.7%). An ultrasonography (USG) failed to diagnose RGB calculi in 10 (11%) patients; whereas, magnetic resonance cholangio-pancreatography (MRCP) accurately diagnosed RGB calculi in all the cases except for 2 (4%) and, additionally, detected common bile duct (CBD) stones in 12 patients. Completion cholecystectomy was performed in all patients (open 45 [48.4%]; laparoscopic 48 [51.6%] and 19 [20.4%] patients required a conversion to open). The RGB pathology included stones in 90 (96.8%), Mirizzi's syndrome in 10 (10.8%) and an internal fistula in 9 (9.7%) patients. Additional procedures included CBD exploration (n=6); Choledocho-duodenostomy (n=4) and Roux-en-Y hepatico-jejunostomy (n=3). The mortality and morbidity were nil and 11% (all wound infection), respectively. Two patients developed incisional hernia during follow up. The mean follow up duration was 23.1 months (3-108) in 65 patients and the outcome was excellent and good in 97% of the patients.
CONCLUSIONS
Post-cholecystectomy recurrent biliary colic should raise suspicion of RGB. MRCP is a useful investigation for the diagnosis and assessment of any associated problems and provides a roadmap for surgery. Laparoscopic completion cholecystectomy is feasible, but is technically difficult and has a high conversion rate.
Keyword
MeSH Terms
Figure
-

Fig. 1 MRC reconstruction displays a residual gallbladder with a stone (marked with solid arrow), as well as choledocholithiasis (marked with hollow arrow).
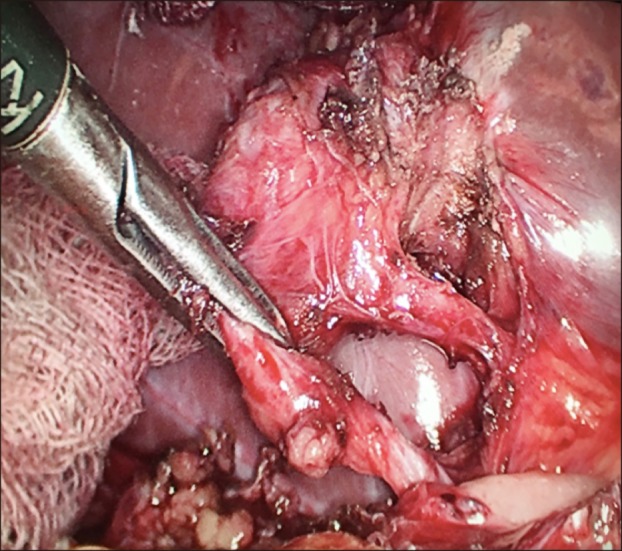
Fig. 2 Intraoperative picture during laparoscopic completion cholecystectomy that displays residual gallbladder with a triangle of safety after Calot's triangle dissection.
Reference
-
1. Philips JA, Lawes DA, Cook AJ, Arulampalam TH, Zaborsky A, Menzies D, et al. The use of laparoscopic subtotal cholecystectomy for complicated cholelithiasis. Surg Endosc. 2008; 22:1697–1700. PMID: 18071804.
Article2. Palanivelu C, Rangarajan M, Jategaonkar PA, Madankumar MV, Anand NV. Laparoscopic management of remnant cystic duct calculi: a retrospective study. Ann R Coll Surg Engl. 2009; 91:25–29. PMID: 18990269.
Article3. Michalowski K, Bornman PC, Krige JE, Gallagher PJ, Terblanche J. Laparoscopic subtotal cholecystectomy in patients with complicated acute cholecystitis or fibrosis. Br J Surg. 1998; 85:904–906. PMID: 9692560.
Article4. Walsh RM, Chung RS, Grundfest-Broniatowski S. Incomplete excision of the gallbladder during laparoscopic cholecystectomy. Surg Endosc. 1995; 9:67–70. PMID: 7725219.
Article5. Womack NA, Crider RL. The persistence of symptoms following cholecystectomy. Ann Surg. 1947; 126:31–55. PMID: 17858976.
Article6. Lum YW, House MG, Hayanga AJ, Schweitzer M. Postcholecystectomy syndrome in the laparoscopic era. J Laparoendosc Adv Surg Tech A. 2006; 16:482–485. PMID: 17004873.
Article7. Chow M, von Waldenfels A, Pace R. An unusual case of a retained stone following laparoscopic cholecystectomy. J Laparoendosc Surg. 1993; 3:513–518. PMID: 8251670.
Article8. Woods MS, Farha GJ, Street DE. Cystic duct remnant fistulization to the gastrointestinal tract. Surgery. 1992; 111:101–104. PMID: 1728064.9. Satorras AM, Villanueva L, Vázquez J, Pigni L, Salem AM, Ramos A. Acute cholecystitis secondary to recurrent cholelithiasis after subtotal cholecystectomy. Cir Esp. 2005; 77:51–53. PMID: 16420885.10. Walsh RM, Ponsky JL, Dumot J. Retained gallbladder/cystic duct remnant calculi as a cause of postcholecystectomy pain. Surg Endosc. 2002; 16:981–984. PMID: 12163968.
Article11. Chowbey PK, Bandyopadhyay SK, Sharma A, Khullar R, Soni V, Baijal M. Laparoscopic reintervention for residual gallstone disease. Surg Laparosc Endosc Percutan Tech. 2003; 13:31–35. PMID: 12598755.
Article12. Tantia O, Jain M, Khanna S, Sen B. Post cholecystectomy syndrome: Role of cystic duct stump and re-intervention by laparoscopic surgery. J Minim Access Surg. 2008; 4:71–75. PMID: 19547688.
Article13. Rozsos I, Magyaródi Z, Orbán P. Cystic duct syndrome and minimally invasive surgery. Orv Hetil. 1997; 138:2397–2401. PMID: 9380377.14. Chowbey P, Soni V, Sharma A, Khullar R, Baijal M. Residual gallstone disease - Laparoscopic management. Indian J Surg. 2010; 72:220–225. PMID: 23133251.
Article15. Pernice LM, Andreoli F. Laparoscopic treatment of stone recurrence in a gallbladder remnant: report of an additional case and literature review. J Gastrointest Surg. 2009; 13:2084–2091. PMID: 19415394.
Article16. Rogy MA, Függer R, Herbst F, Schulz F. Reoperation after cholecystectomy. The role of the cystic duct stump. HPB Surg. 1991; 4:129–134. PMID: 1931779.17. Daly TD, Martin CJ, Cox MR. Residual gallbladder and cystic duct stones after laparoscopic cholecystectomy. ANZ J Surg. 2002; 72:375–377. PMID: 12028103.
Article18. Rieger R, Wayand W. Gallbladder remnant after laparoscopic cholecystectomy. Surg Endosc. 1995; 9:844. PMID: 7482201.
Article19. Mergener K, Clavien PA, Branch MS, Baillie J. A stone in a grossly dilated cystic duct stump: a rare cause of postcholecystectomy pain. Am J Gastroenterol. 1999; 94:229–231. PMID: 9934761.
Article20. Ibrarullah MD, Kacker LK, Sikora SS, Saxena R, Kapoor VK, Kaushik SP. Partial cholecystectomy--safe and effective. HPB Surg. 1993; 7:61–65. PMID: 8260436.21. Chowbey PK, Sharma A, Khullar R, Mann V, Baijal M, Vashistha A. Laparoscopic subtotal cholecystectomy: a review of 56 procedures. J Laparoendosc Adv Surg Tech A. 2000; 10:31–34. PMID: 10706300.
Article22. Ji W, Li LT, Li JS. Role of laparoscopic subtotal cholecystectomy in the treatment of complicated cholecystitis. Hepatobiliary Pancreat Dis Int. 2006; 5:584–589. PMID: 17085347.23. Blackard WG Jr, Baron TH. Leaking gallbladder remnant with cholelithiasis complicating laparoscopic cholecystectomy. South Med J. 1995; 88:1166–1168. PMID: 7481995.
Article24. Beldi G, Glättli A. Laparoscopic subtotal cholecystectomy for severe cholecystitis. Surg Endosc. 2003; 17:1437–1439. PMID: 12799885.
Article25. Kim JY, Kim KW, Ahn CS, Hwang S, Lee YJ, Shin YM, et al. Spectrum of biliary and nonbiliary complications after laparoscopic cholecystectomy: radiologic findings. AJR Am J Roentgenol. 2008; 191:783–789. PMID: 18716110.
Article26. Wani NA, Khan NA, Shah AI, Khan AQ. Post-cholecystectomy Mirizzi's syndrome: magnetic resonance cholangiopancreatography demonstration. Saudi J Gastroenterol. 2010; 16:295–298. PMID: 20871198.
Article27. Shelton JH, Mallat DB. Endoscopic retrograde removal of gallbladder remnant calculus. Gastrointest Endosc. 2006; 64:272–273. PMID: 16860084.
Article28. Kodali VP, Petersen BT. Endoscopic therapy of postcholecystectomy Mirizzi syndrome. Gastrointest Endosc. 1996; 44:86–90. PMID: 8836726.
Article29. Benninger J, Rabenstein T, Farnbacher M, Keppler J, Hahn EG, Schneider HT. Extracorporeal shockwave lithotripsy of gallstones in cystic duct remnants and Mirizzi syndrome. Gastrointest Endosc. 2004; 60:454–459. PMID: 15332046.
Article30. Rozsos I, Magyaródi Z, Orbán P. The removal of cystic duct and gallbladder remnant by microlaparotomy. Acta Chir Hung. 1997; 36:297–298. PMID: 9408381.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Clinical Analysis on Primary Cancer of the Gall Bladder
- Gall bladder wal varices:Easy diagnosis with multiphase incremental bolus dynamic CT
- Management for the Polypoid Lesions of Gall Bladder
- The Experience of the Treatment of Scapular and Midback Pain in a Patient with Gall Bladder Cancer: A case report
- Demographics of Thoracolumbar Fracture in Indian Population Presenting to a Tertiary Level Trauma Centre
