Brown-Séquard Syndrome and Cervical Vertebral Fractures after Blunt Cervical Trauma in a Traffic Accident - A Case Report -
- Affiliations
-
- 1Department of Orthopaedic Surgery, Hanyang University College of Medicine, Seoul, Korea. cnkang65@hanyang.ac.kr
- 2Department of Orthopaedic Surgery, Sung-Ae Hospital, Seoul, Korea.
- KMID: 2408195
- DOI: http://doi.org/10.4184/jkss.2017.24.4.252
Abstract
- STUDY DESIGN: Case report
OBJECTIVES
To report a case of Brown-Séquard syndrome after blunt cervical trauma. SUMMARY OF LITERATURE REVIEW: Brown-Séquard syndrome is a rare disease characterized by hemisection of the spinal cord, and it shows the best prognosis of the various types of incomplete spinal cord injuries.
MATERIALS AND METHODS
A patient with Brown-Séquard syndrome that occurred after a traffic accident was followed up for 2 years and 6 months.
RESULTS
We observed normal recovery of motor strength, but sensory impairment and deep tendon hyperreflexia remained.
CONCLUSIONS
Brown-Séquard syndrome is known to have a good prognosis, but in this case, the neurological abnormality did not fully recover; therefore, we report this rare case and present a review of the literature.
MeSH Terms
Figure
-
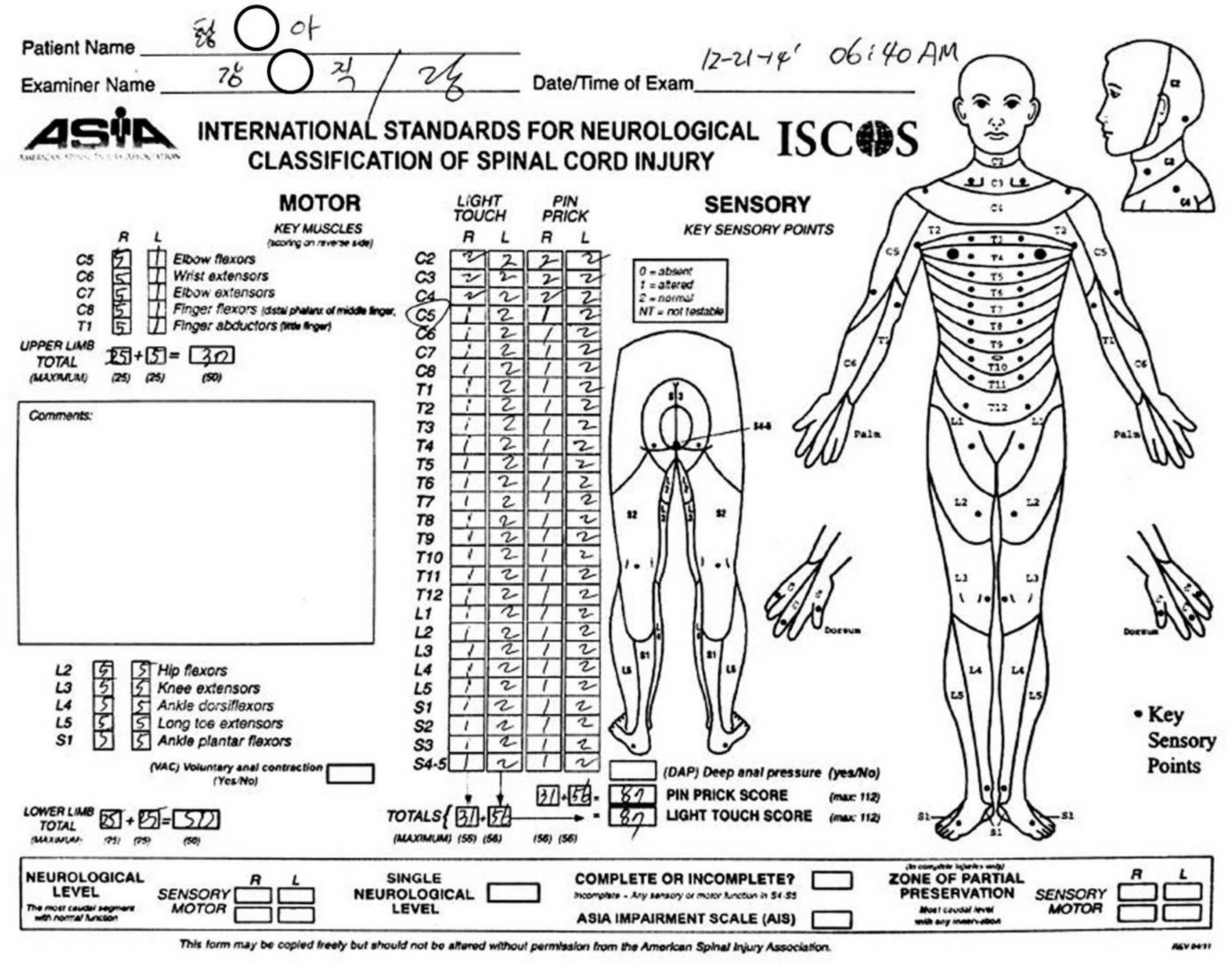
Fig. 1. The patient's medical record with an assessment using the American Spinal Injury Association (ASIA) impairment scale at the initial visit.
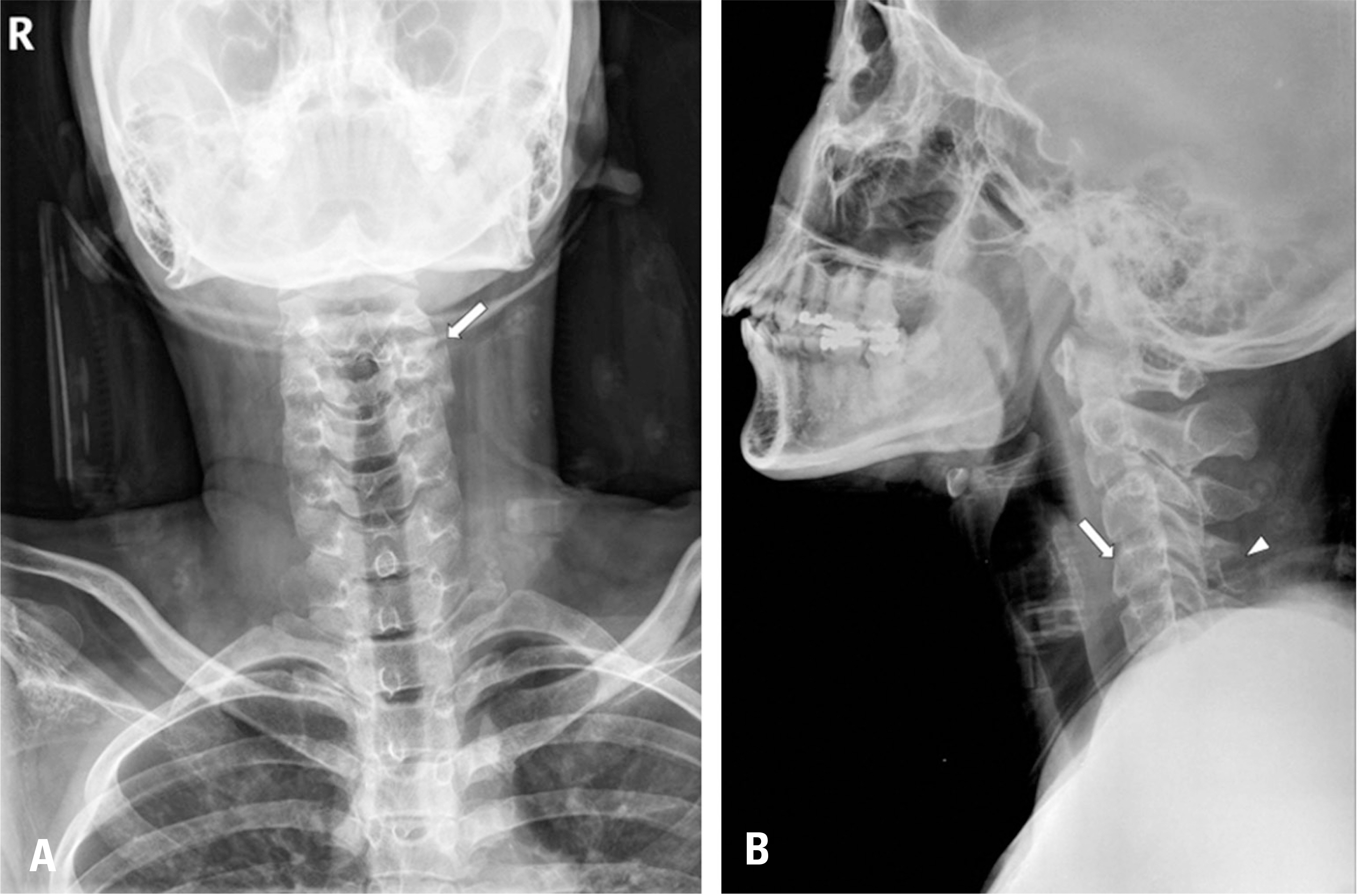
Fig. 2. Simple radiographs of the cervical spine. The anteroposterior view (A) shows a fracture of the left superior articular process of C3 (arrow). The lateral view (B) shows fractures of the body of C4 (arrow) and the spinous process of C4 (arrowhead).
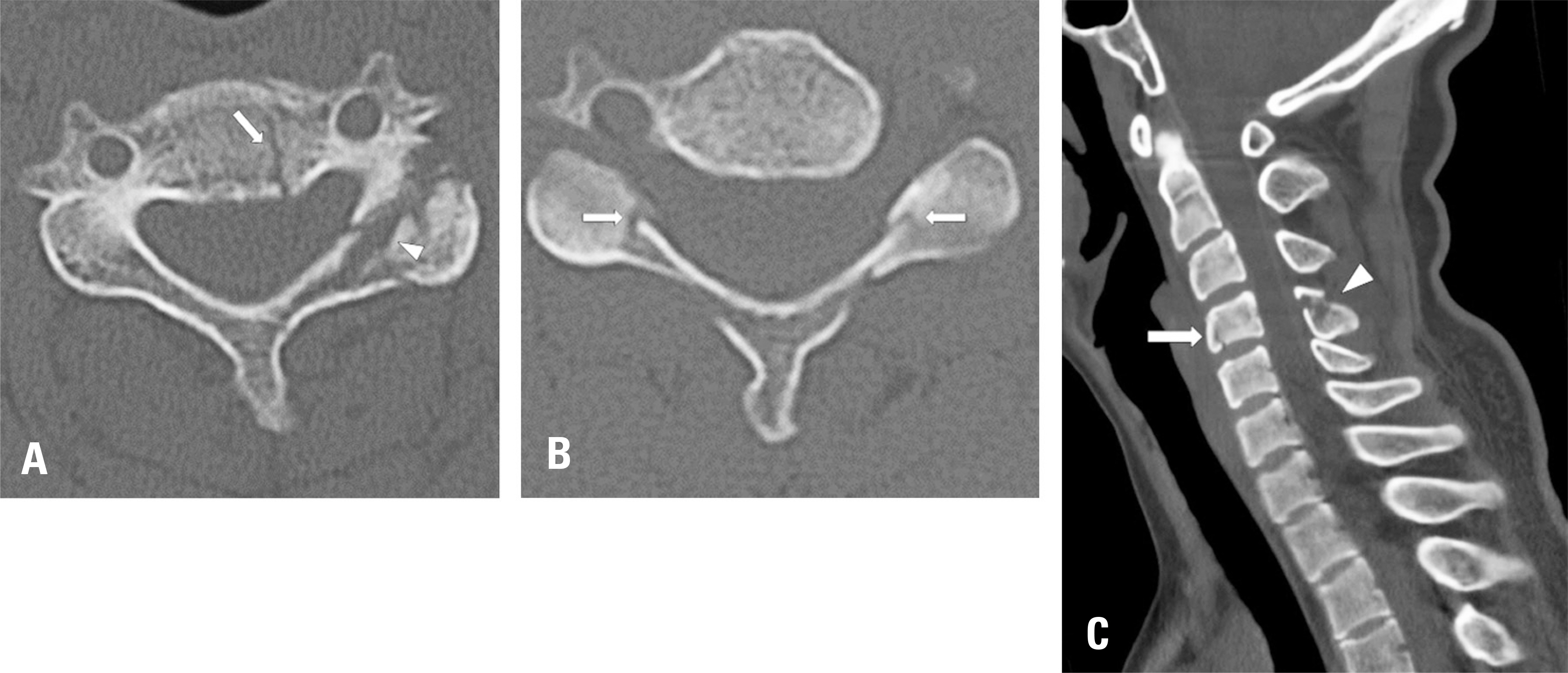
Fig. 3. Computed tomography of the cervical spine. The axial view of C3 (A) shows fractures of the body (arrow), left superior articular process, and lamina (arrowhead). The axial view of C4 (B) shows fractures of both lamina (arrow). The midsagittal view (C) shows fractures of the body of C4 (arrow) and the spinous process of C4 (arrowhead). There was no spinal canal encroachment.
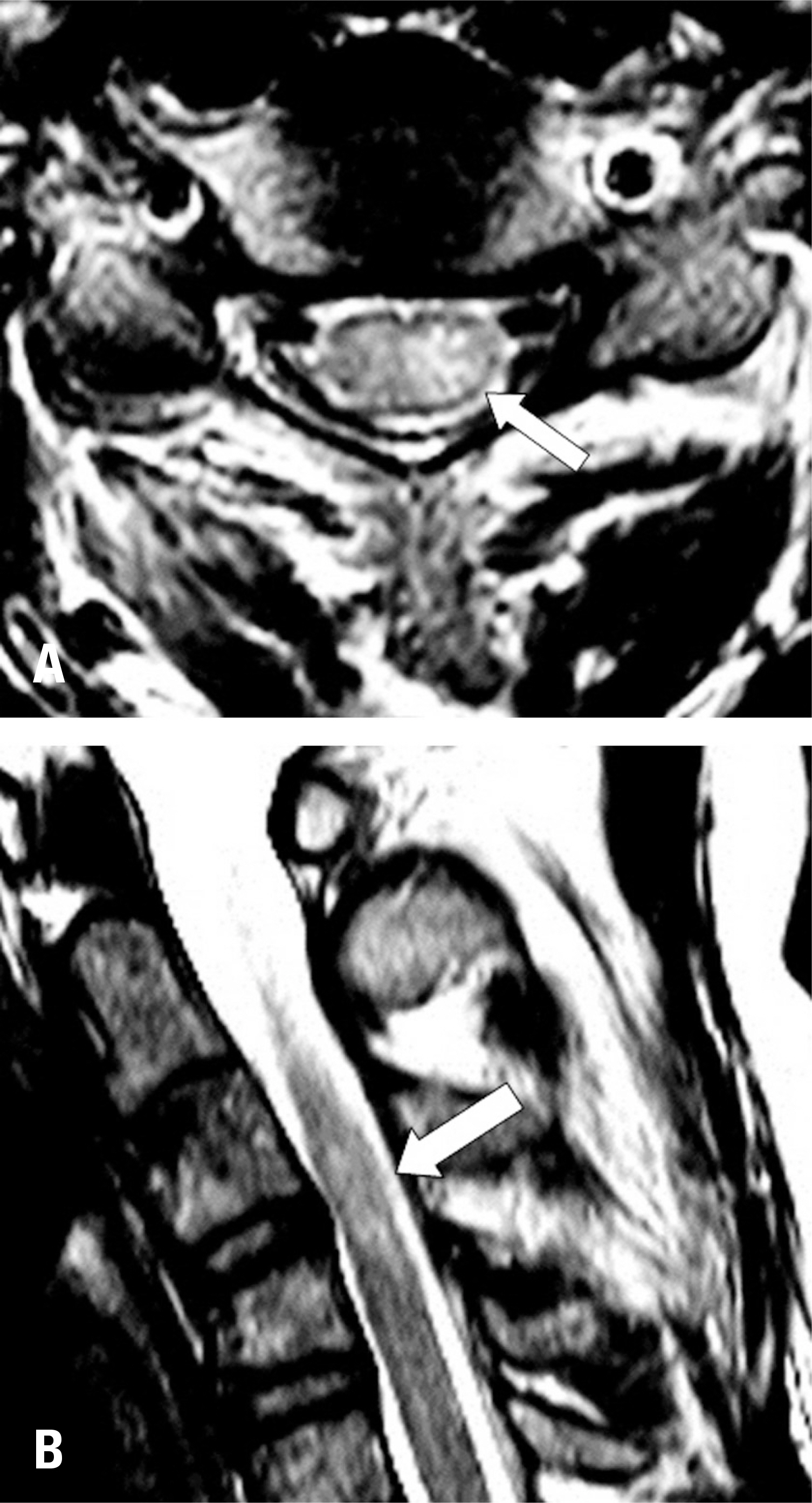
Fig. 4. The axial (A) and midsagittal (B) view of T2-weighted magnetic resonance images. The arrow indicates high signal intensity in the left side of the spinal cord at the C3-C4 level.
Reference
-
1. McKinley W, Santos K, Meade M, et al. Incidence and outcomes of spinal cord injury clinical syndromes. J Spinal Cord Med. 2007; 30(3):215–24. DOI: 10.1080/10790268.2007.11753929.
Article2. Miranda P, Gomez P, Alday R, et al. Brown-Sequard syndrome after blunt cervical spine trauma: clinical and radiological correlations. Eur Spine J. 2007 Aug; 16(8):1165–70. DOI: 10.1007/s00586-007-0345-7.
Article3. Brown-séquard E. Experimental and Clinical Researches on the Physiology and Pathology of the Spinal Cord, and some other parts of the Nervous Centres. Am J Med Sci. 1855 Jul; 30(59):161–5. DOI: 10.1097/00000441-185507000-00023.
Article4. Johnson S, Jones M, Zumsteg J. Brown-Séquard syndrome without vascular injury associated with Horner's syndrome after a stab injury to the neck. J Spinal Cord Med. 2016; 39(1):111–4. DOI: 10.1179/2045772314Y.0000000297.
Article5. Garcia-Manzanares M, Belda-Sanchis J, Giner-Pascual M, et al. Brown-Sequard syndrome associated with Horner's syndrome after a penetrating trauma at the cervicomedullary junction. Spinal Cord. 2000 Nov; 38(11):705–7. DOI: 10.1038/sj.sc.3101062.
Article6. Roth EJ, Park T, Pang T, et al. Traumatic cervical Brown-Sequard and Brown-Sequard-plus syndromes: the spectrum of presentations and outcomes. Paraplegia. 1991 Nov; 29(9):582–9. DOI: 10.1038/sc.1991.86.
Article7. Mataliotakis GI, Tsirikos AI. Spinal cord trauma: pathophysiology, classification of spinal cord injury syndromes, treatment principles and controversies. Orthop Trauma. 2016; 30(5):440–9. DOI: 10.1016/j.mporth.2016.07.006.
Article8. Oller D, Boone S. Blunt cervical spine Brown-Séquard injury. A report of three cases. Am Surg. 1991 Jun; 57(6):361–5.9. Little JW, Halar E. Temporal course of motor recovery after Brown-Sequard spinal cord injuries. Spinal Cord. 1985 Feb; 23(1):39–46. DOI: 10.1038/sc.1985.7.
Article10. Lim E, Wong Y, Lo Y, et al. Traumatic atypical Brown-Sequard syndrome: case report and literature review. Clin Neurol Neurosurg. 2003 Apr; 105(2):143–5. DOI: 10.1016/s0303-8467 (03)00009-x.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Cervical Spinal Cord Infarction Presenting Brown-Séquard-plus Syndrome
- Unilateral loss of thoracic motion after blunt trauma: a sign of acute Brown-Séquard syndrome
- Extradural Cervical Disc Herniation Causing Sudden Brown-se'quard Syndrome: A Case Report
- Vertebral Artery Injury Following Blunt Trauma to the Cervical Spine Case Report and Literature Review
- Brown-Séquard Syndrome Caused by Acute Traumatic Cervical Disc Herniation
