A Comprehensive Review of Shoulder CT Morphometry: What Surgeons Wants to Know
- Affiliations
-
- 1Department of Radiology, Seoul National University Bundang Hospital, Seongnam, Korea. joongmoahn@gmail.com
- 2Department of Orthopaedic Surgery, Seoul National University Bundang Hospital, Seongnam, Korea.
- KMID: 2407932
- DOI: http://doi.org/10.3348/jksr.2018.78.4.265
Abstract
- A variety of surgical techniques have been employed for shoulder problems, i.e., arthroplasty, arthroscopy, and fracture fixation, etc. A thorough understanding and knowledge of the normal anatomy, physiology, biomechanics, and pathomechanics of the glenohumeral joint can help facilitate a successful pre-operative evaluation of the shoulder. The authors reviewed practical measurement methods of a shoulder computed tomography (CT) with three-dimensional volume-rendered images, from the orthopedic surgeon's viewpoint, to aid radiologists make structured reports. It is important that the radiologist be familiar with the normal and abnormal imaging appearances of the shoulder CT before and after the surgical procedures.
MeSH Terms
Figure
-
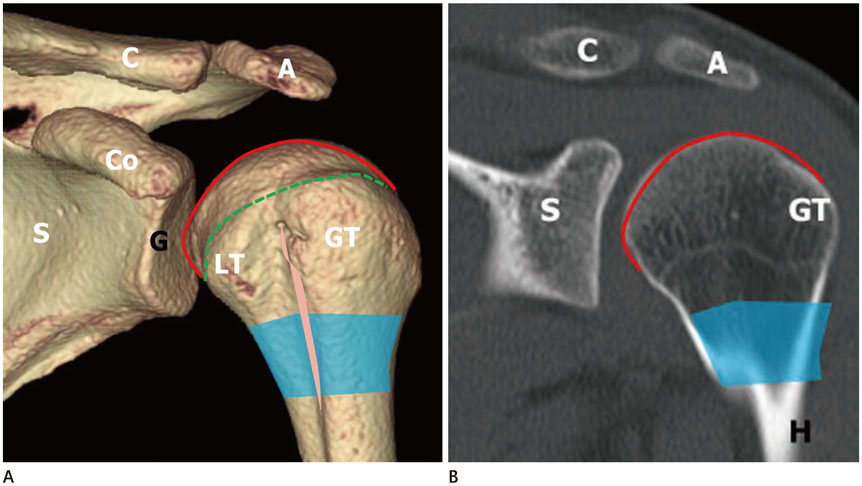
Fig. 1 The normal anatomy of the shoulder joint of a 20-year-old female. Three-dimensional volume-rendered (A), coronal-reformatted computed tomography images (B). The proximal humerus comprises the humeral head (shown in red line on online figure), anatomical neck (shown in green dotted line on online figure), surgical neck (shaded area), greater tubercle, lesser tubercle, and the bicipital groove (shown in pink line on online figure, between GT and LT). A = acromion, C = clavicle, Co = coracoid process, G = glenoid, GT = greater tubercle, H = humerus, LT = lesser tubercle, S = scapula

Fig. 2 The normal anatomy of glenoid in a 20-year-old female. Three-dimensional volume-rendered (A), sagittal-reformatted images (B). The glenoid is composed of the glenoid neck and fossa. The superior (shown in purple line on online figure, white arrows) and inferior (shown in orange line on online figure, black arrows) glenoid tubercles are two small tubercles located above and below the glenoid cavity on the scapula. A = acromion, C = clavicle, Co = coracoid process, G = glenoid, S′ = supraspinous fossa
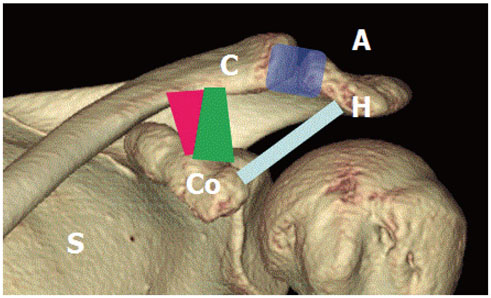
Fig. 3 The normal anatomy of shoulder joint of a 20-year-old female. Three-dimensional volume-rendered image demonstrates acromioclavicular ligament (shown in purple on online figure), coracoclavicular ligament comprised of conoid (shown in pink on online figure) and trapezoid (shown in green on online figure) components and the coracoacromial ligament (shown in light blue on online figure). A = acromion, C = clavicle, Co = coracoid process, H = humerus, S = scapula

Fig. 4 Glenoid version measurement by Friedman and Matsumura method. A. The glenoid version is measured as the angle (α) between line G and line S′ on axial image using the Friedman method. B. The glenoid version is measured as the angle (β) between line G and line S′ on the axial image using the Matsumura method. The Matsumura vault method showed larger glenoid retroversion (20°) than the Friedman glenoid version (13°) method. Line G = Line connecting the anterior and posterior margin of the glenoid, Line S = Line connecting the tip of the scapular vault to the center of the glenoid, Line S′ = Line perpendicular to line S

Fig. 5 Walch classificiation of glenoid wear. On the left, centered humeral head with minor (Walch type A1) or major (Walch type A2) central erosion is demonstrated. In the middle, the humeral head is posteriorly subluxed with narrowing of the posterior joint space, osteophytes, sclerosis (Walch type B1) and posterior rim erosion with retroverted glenoid (Walch type B2). On the right, Walch type C morphology is demonstrated as a glenoid retroversion more than 25 degrees regardless of the erosion. H = humeral head
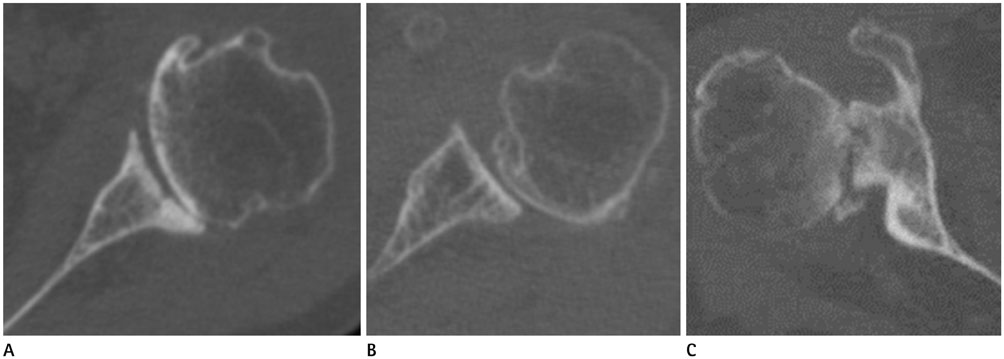
Fig. 6 CT images of glenoid wear by walch classification. A. Axial CT image of the left shoulder of a 50-year-old female showing central erosion without retroverted glenoid, consistent with Walch type A1 morphology. B. Axial CT image of the shoulder of a 61-year-old male showing narrowing of the posterior joint space, posterior subluxation of humeral head and subchondral sclerosis without retroverted glenoid classified as Walch type B1 morphology. C. Axial CT image of the shoulder of a 71-year-old female showing marked posterior glenoid wear with fragmentation of the posterior glenoid rim with retroverted glenoid, compatible with Walch type C morphology. CT = computed tomography
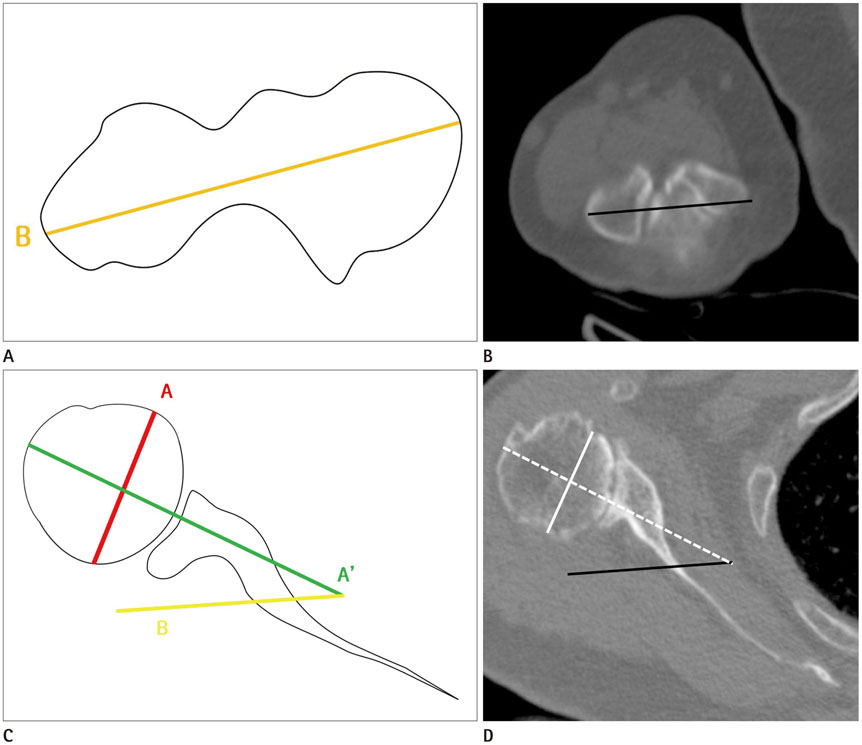
Fig. 7 Measurement of Humeral head retroversion. A, B. Illustration (A), CT axial image (B) a 67-year-old female shows transepiphyseal line (line B) between the most prominent medial and lateral epicondyles. C. The humeral head retroversion is defined as the angular difference between the orientation of the proximal humeral head (line A′) and the axis of the elbow at the level of distal humerus (line B). D. Axial shoulder computed tomography image demonstrates the transepiphyseal line and humeral head retroversion. Line A = a line passing through the center of the head of the humerus, Line A′ = a line perpendicular to line A, Line B = transepicondylar axis
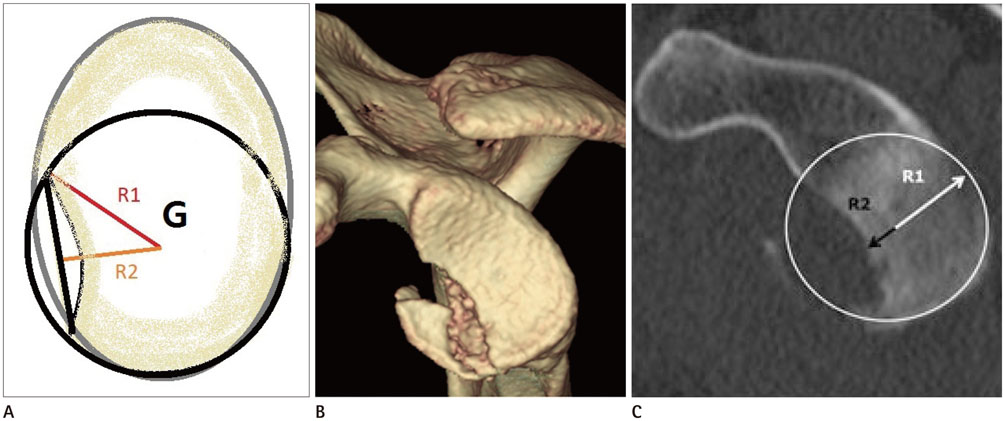
Fig. 8 Measurement of the bony Bankart lesion. A. A best fit circle (black circle) is drawn covering the curve of inferior portion of the glenoid (grey line) R2 is the line from the center of the glenoid center to the margin of the bony Bankart lesion. B, C. Volume-rendered (B), sagittal computed tomography (C) images show a bony Bankart lesion at the antero-inferior glenoid. G = glenoid
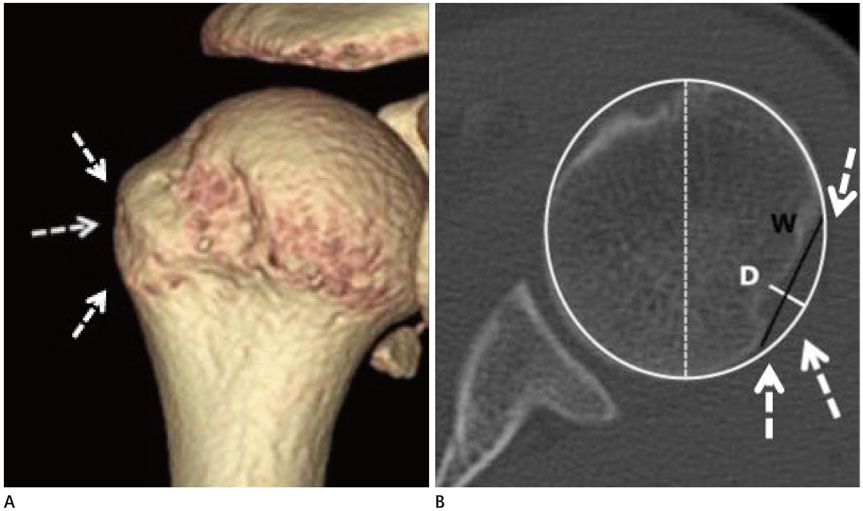
Fig. 9 Measurement of the Hill-Sachs lesion. Volume-rendered (A), axial shoulder computed tomography (B) images show a Hill-Sachs lesion (arrows). W (black line) is the distance between anterior and posterior margin of the defect, while D (white line) is the distance between the floor of the defect and the imaginary contour of the humeral head. The relative percentage to the diameter (white dotted line) of the humeral head was also calculated. D = depth, W = width
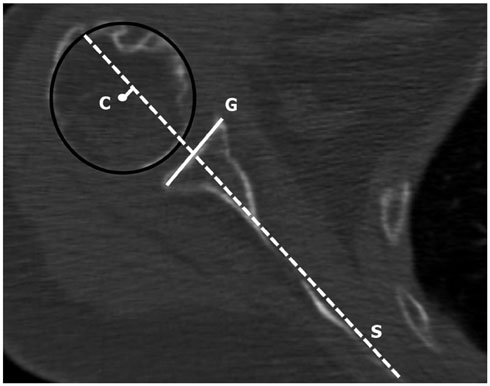
Fig. 10 Quantifying the humeral position relative to glenoid fossa on axial shoulder computed tomography image in a 76-year-old female. The humeral translation distance is defined as the distance from the center of the humeral head to the scapular line (line S, at mid glenoid level). Line G = line connecting anterior and posterior end of osseous glenoid, Line S = axis of scapula, line from anterior surface of the scapular body to the midpoint of line G.
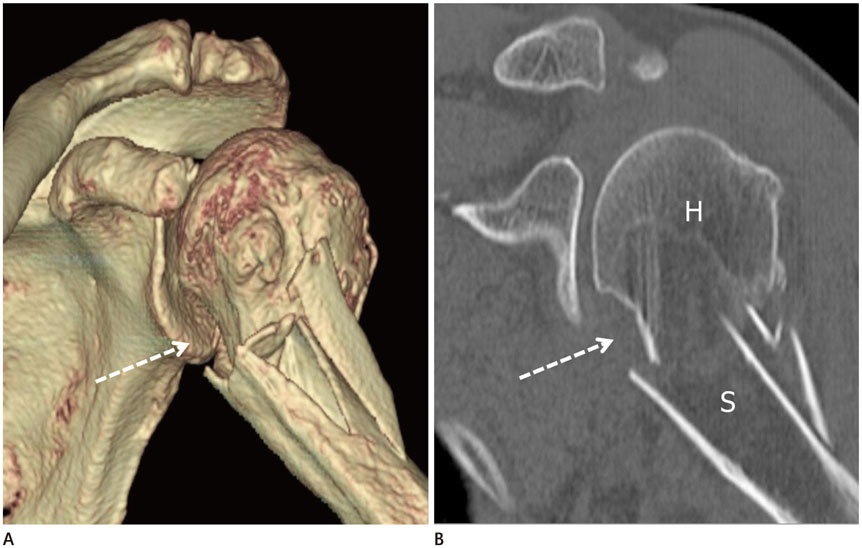
Fig. 11 Comminuted humeral surgical neck fracture in a 50-year-old female after a fall. Volume-rendered (A), shoulder computed tomography (B) images show a significant angulation(≥ 45′) (arrows) with displacement of the surgical neck, suggesting a two-part fracture. H = humerus, S = scapula
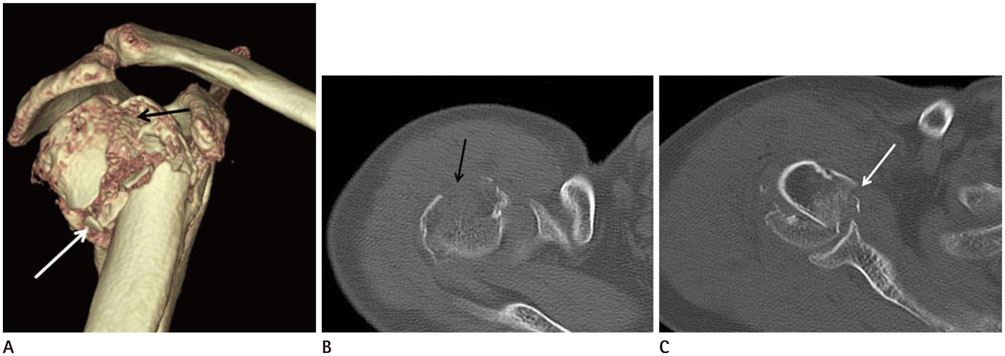
Fig. 12 Comminuted right humeral fracture in a 40-year-old female involved in a traffic accident. Volume-rendered (A), axial shoulder computed tomography (B, C) images show a significant displacement (≥ 1 cm) of greater tuberosity (black arrows) and impaction at surgical neck (white arrows), suggesting a three-part fracture.
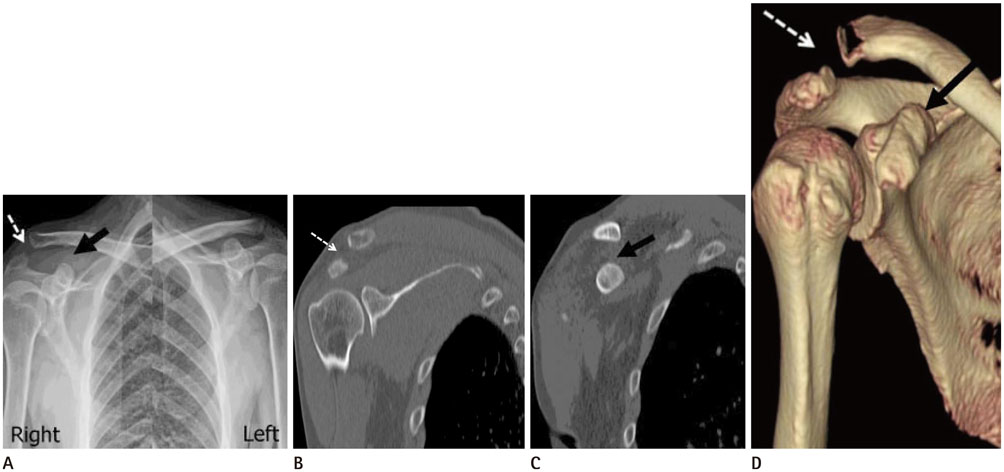
Fig. 13 Plain radiograph, CT images of a 53-year-old male after a fall. Plain radiograph demonstrates widening of the AC joint space (white arrow in A), and CC interval (black arrow in A). There was a 50% (between 25–100%) increase in the CC interval, the lesion was classified as Rockwood Type III. CT images also revealed widening of the AC (white arrow in B, D) and CC spaces (black arrow in C, D).
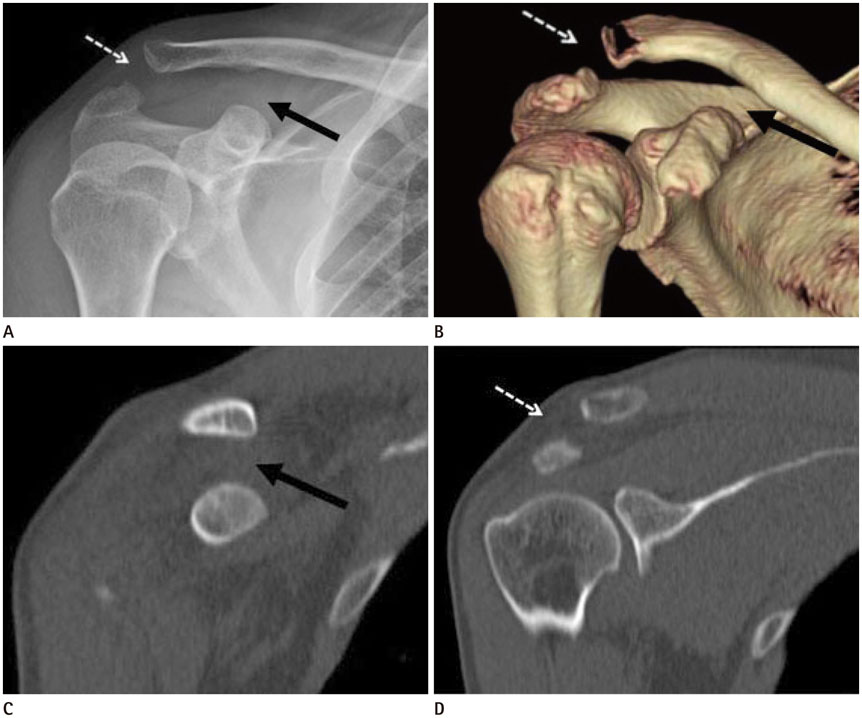
Fig. 14 Plain radiograph, CT images of a 21-year-old male after a fall. The plain radiograph demonstrates the widening of AC joint space (white arrow in A), CC interval (black arrow in A). Because the CC joint space was twice wider than the normal left, the lesion was classified as Rockwood Type V. CT images also revealed separation of the AC (white arrow in B, D) and CC spaces (black arrow in B, C). AC = acromioclavicular, CC = coracoclavicular, CT = computed tomography
Reference
-
1. Pearl ML. Proximal humeral anatomy in shoulder arthroplasty: implications for prosthetic design and surgical technique. J Shoulder Elbow Surg. 2005; 14:1 Suppl S. 99S–104S.
Article2. Whiston TB. Fractures of the surgical neck of the humerus. J Bone Joint Surg Br. 1954; 36-B:423–427.
Article3. Sandstrom CK, Kennedy SA, Gross JA. Acute shoulder trauma: what the surgeon wants to know. Radiographics. 2015; 35:475–492.
Article4. Fukuda K, Craig EV, An KN, Cofield RH, Chao EY. Biomechanical study of the ligamentous system of the acromioclavicular joint. J Bone Joint Surg Am. 1986; 68:434–440.
Article5. Hoenecke HR Jr, Hermida JC, Flores-Hernandez C, D'Lima DD. Accuracy of CT-based measurements of glenoid version for total shoulder arthroplasty. J Shoulder Elbow Surg. 2010; 19:166–171.
Article6. Shapiro TA, McGarry MH, Gupta R, Lee YS, Lee TQ. Biomechanical effects of glenoid retroversion in total shoulder arthroplasty. J Shoulder Elbow Surg. 2007; 16:3 Suppl. S90–S95.
Article7. Friedman RJ, Hawthorne KB, Genez BM. The use of computerized tomography in the measurement of glenoid version. J Bone Joint Surg Am. 1992; 74:1032–1037.
Article8. Iannotti JP, Norris TR. Influence of preoperative factors on outcome of shoulder arthroplasty for glenohumeral osteoarthritis. J Bone Joint Surg Am. 2003; 85-A:251–258.
Article9. Inui H, Sugamoto K, Miyamoto T, Machida A, Hashimoto J, Nobuhara K. Evaluation of three-dimensional glenoid structure using MRI. J Anat. 2001; 199(Pt 3):323–328.
Article10. Matsumura N, Ogawa K, Ikegami H, Collin P, Walch G, Toyama Y. Computed tomography measurement of glenoid vault version as an alternative measuring method for glenoid version. J Orthop Surg Res. 2014; 9:17.
Article11. Farron A, Terrier A, Büchler P. Risks of loosening of a prosthetic glenoid implanted in retroversion. J Shoulder Elbow Surg. 2006; 15:521–526.
Article12. Walch G, Badet R, Boulahia A, Khoury A. Morphologic study of the glenoid in primary glenohumeral osteoarthritis. J Arthroplasty. 1999; 14:756–760.
Article13. Boileau P, Bicknell RT, Mazzoleni N, Walch G, Urien JP. CT scan method accurately assesses humeral head retroversion. Clin Orthop Relat Res. 2008; 466:661–669.
Article14. Kronberg M, Broström LA. Humeral head retroversion in patients with unstable humeroscapular joints. Clin Orthop Relat Res. 1990; (260):207–211.
Article15. Boileau P, Walch G, Liotard JP. [Radio-cinematographic study of active elevation of the prosthetic shoulder]. Rev Chir Orthop Reparatrice Appar Mot. 1992; 78:355–364.16. Robertson DD, Yuan J, Bigliani LU, Flatow EL, Yamaguchi K. Three-dimensional analysis of the proximal part of the humerus: relevance to arthroplasty. J Bone Joint Surg Am. 2000; 82-A:1594–1602.
Article17. Hempfing A, Leunig M, Ballmer FT, Hertel R. Surgical landmarks to determine humeral head retrotorsion for hemiarthroplasty in fractures. J Shoulder Elbow Surg. 2001; 10:460–463.
Article18. Kummer FJ, Perkins R, Zuckerman JD. The use of the bicipital groove for alignment of the humeral stem in shoulder arthroplasty. J Shoulder Elbow Surg. 1998; 7:144–146.
Article19. Hertel R, Knothe U, Ballmer FT. Geometry of the proximal humerus and implications for prosthetic design. J Shoulder Elbow Surg. 2002; 11:331–338.
Article20. McPherson EJ, Friedman RJ, An YH, Chokesi R, Dooley RL. Anthropometric study of normal glenohumeral relationships. J Shoulder Elbow Surg. 1997; 6:105–112.
Article21. Krahl VE. The phylogeny and ontogeny of humeral torsion. Am J Phys Anthropol. 1976; 45(3 pt. 2):595–599.
Article22. Saka M, Yamauchi H, Yoshioka T, Hamada H, Gamada K. Conventional humeral retroversion measurements using computed tomography slices or ultrasound images are not correlated with the 3-dimensional humeral retroversion angle. Orthop J Sports Med. 2015; 3:2325967115573701.
Article23. Saka M, Yamauchi H, Hoshi K, Yoshioka T, Hamada H, Gamada K. Reliability and validity in measurement of true humeral retroversion by a three-dimensional cylinder fitting method. J Shoulder Elbow Surg. 2015; 24:809–813.
Article24. Boileau P, Villalba M, Héry JY, Balg F, Ahrens P, Neyton L. Risk factors for recurrence of shoulder instability after arthroscopic Bankart repair. J Bone Joint Surg Am. 2006; 88:1755–1763.
Article25. Taylor DC, Arciero RA. Pathologic changes associated with shoulder dislocations. Arthroscopic and physical examination findings in first-time, traumatic anterior dislocations. Am J Sports Med. 1997; 25:306–331.26. Stevens KJ, Preston BJ, Wallace WA, Kerslake RW. CT imaging and three-dimensional reconstructions of shoulders with anterior glenohumeral instability. Clin Anat. 1999; 12:326–336.
Article27. Itoi E, Lee SB, Amrami KK, Wenger DE, An KN. Quantitative assessment of classic anteroinferior bony Bankart lesions by radiography and computed tomography. Am J Sports Med. 2003; 31:112–118.
Article28. Itoi E, Lee SB, Berglund LJ, Berge LL, An KN. The effect of a glenoid defect on anteroinferior stability of the shoulder after Bankart repair: a cadaveric study. J Bone Joint Surg Am. 2000; 82:35–46.
Article29. Saliken DJ, Bornes TD, Bouliane MJ, Sheps DM, Beaupre LA. Imaging methods for quantifying glenoid and Hill-Sachs bone loss in traumatic instability of the shoulder: a scoping review. BMC Musculoskelet Disord. 2015; 16:164.
Article30. Burkhart SS, Debeer JF, Tehrany AM, Parten PM. Quantifying glenoid bone loss arthroscopically in shoulder instability. Arthroscopy. 2002; 18:488–491.
Article31. Chuang TY, Adams CR, Burkhart SS. Use of preoperative three-dimensional computed tomography to quantify glenoid bone loss in shoulder instability. Arthroscopy. 2008; 24:376–382.
Article32. Sugaya H. Techniques to evaluate glenoid bone loss. Curr Rev Musculoskelet Med. 2014; 7:1–5.
Article33. Bois AJ, Fening SD, Polster J, Jones MH, Miniaci A. Quantifying glenoid bone loss in anterior shoulder instability: reliability and accuracy of 2-dimensional and 3-dimensional computed tomography measurement techniques. Am J Sports Med. 2012; 40:2569–2577.34. Nofsinger C, Browning B, Burkhart SS, Pedowitz RA. Objective preoperative measurement of anterior glenoid bone loss: a pilot study of a computer-based method using unilateral 3-dimensional computed tomography. Arthroscopy. 2011; 27:322–329.
Article35. Assunção JH, Gracitelli ME, Borgo GD, Malavolta EA, Bordalo-Rodrigues M, Ferreira Neto AA. Tomographic evaluation of Hill-Sachs lesions: is there a correlation between different methods of measurement. Acta Radiol. 2017; 58:77–83.
Article36. Richards RD, Sartoris DJ, Pathria MN, Resnick D. Hill-Sachs lesion and normal humeral groove: MR imaging features allowing their differentiation. Radiology. 1994; 190:665–668.
Article37. Kodali P, Jones MH, Polster J, Miniaci A, Fening SD. Accuracy of measurement of Hill-Sachs lesions with computed tomography. J Shoulder Elbow Surg. 2011; 20:1328–1334.
Article38. Cho SH, Cho NS, Rhee YG. Preoperative analysis of the Hill-Sachs lesion in anterior shoulder instability: how to predict engagement of the lesion. Am J Sports Med. 2011; 39:2389–2395.39. Kaar SG, Fening SD, Jones MH, Colbrunn RW, Miniaci A. Effect of humeral head defect size on glenohumeral stability: a cadaveric study of simulated Hill-Sachs defects. Am J Sports Med. 2010; 38:594–599.40. Provencher MT, Frank RM, Leclere LE, Metzger PD, Ryu JJ, Bernhardson A, et al. The Hill-Sachs lesion: diagnosis, classification, and management. J Am Acad Orthop Surg. 2012; 20:242–252.
Article41. Yun G, Kang Y, Ahn JM, Lee E, Lee JW, Oh JH, et al. Posterior decentering of the humeral head on shoulder MR arthrography: significant association with posterior synovial proliferation. AJR Am J Roentgenol. 2017; 208:1297–1303.
Article42. Shah N, Tung GA. Imaging signs of posterior glenohumeral instability. AJR Am J Roentgenol. 2009; 192:730–735.
Article43. Tung GA, Hou DD. MR arthrography of the posterior labrocapsular complex: relationship with glenohumeral joint alignment and clinical posterior instability. AJR Am J Roentgenol. 2003; 180:369–375.
Article44. Court-Brown CM, Caesar B. Epidemiology of adult fractures: a review. Injury. 2006; 37:691–697.
Article45. Neer CS 2nd. Displaced proximal humeral fractures. II. Treatment of three-part and four-part displacement. J Bone Joint Surg Am. 1970; 52:1090–1103.46. Murray IR, Amin AK, White TO, Robinson CM. Proximal humeral fractures. J Bone Joint Surg Br. 2011; 93-B:1–11.
Article47. Sidor ML, Zuckerman JD, Lyon T, Koval K, Cuomo F, Schoenberg N. The Neer classification system for proximal humeral fractures. An assessment of interobserver reliability and intraobserver reproducibility. J Bone Joint Surg Am. 1993; 75:1745–1150.
Article48. Siebenrock KA, Gerber C. The reproducibility of classification of fractures of the proximal end of the humerus. J Bone Joint Surg Am. 1993; 75:1751–1755.
Article49. Berkes MB, Dines JS, Little MT, Garner MR, Shifflett GD, Lazaro LE, et al. The impact of three-dimensional CT imaging on intraobserver and interobserver reliability of proximal humeral fracture classifications and treatment recommendations. J Bone Joint Surg Am. 2014; 96:1281–1286.
Article50. Cho CH, Oh JH, Jung GH, Moon GH, Rhyou IH, Yoon JP, et al. The interrater and intrarater agreement of a modified neer classification system and associated treatment choice for lateral clavicle fractures. Am J Sports Med. 2015; 43:2431–2436.
Article51. Hertel R, Hempfing A, Stiehler M, Leunig M. Predictors of humeral head ischemia after intracapsular fracture of the proximal humerus. J Shoulder Elbow Surg. 2004; 13:427–433.
Article52. Min W, Davidovitch RI, Tejwani NC. Three-and four-part proximal humerus fractures: evolution to operative care. Bull NYU Hosp Jt Dis. 2012; 70:25–34.53. Mazzocca AD, Arciero RA, Bicos J. Evaluation and treatment of acromioclavicular joint injuries. Am J Sports Med. 2007; 35:316–329.
Article54. Williams GR, Nguyen VD, Rockwood CA. Classification and radiographic analysis of acromioclavicular dislocations. Appl Radiol. 1989; 18:29–34.55. Senna LF, Pires E. Modified axillary radiograph of the shoulder: a new position. Rev Bras Ortop. 2016; 52:115–118.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Dynamic ultrasonography of the shoulder
- Current Concepts and Recent Trends in Arthroscopic Treatment of Large to Massive Rotator Cuff Tears: A Review
- Rate of incidental findings on routine preoperative computed tomography for shoulder arthroplasty
- Ultrasound Guidance for Intra-Articular Shoulder Injections for Frozen Shoulder
- Extravasation of Joint Fluid into the Mediastinum and the Deep Neck during Arthroscopic Shoulder Surgery
