Total Transcanal Endoscopic Facial Nerve Decompression for Traumatic Facial Nerve Palsy
- Affiliations
-
- 1Department of Otorhinolaryngology, Muhimbili University of Health and Allied Sciences, Dar es Salaam, Tanzania.
- 2Department of Otorhinolaryngology, Yonsei University College of Medicine, Seoul, Korea. ismoonmd@yuhs.ac
- KMID: 2407871
- DOI: http://doi.org/10.3349/ymj.2018.59.3.457
Abstract
- A few approaches can be used to decompress traumatic facial nerve paralysis including the middle cranial fossa approach or transmastoid approach depending on the site of injury. In some specific situation of treating traumatic facial nerve palsy whose injured site was confined from the geniculate ganglion to the second genu, transcanal endoscopic approach for facial nerve decompression can be used. We performed two cases of total endoscopic transcanal facial nerve decompression in patients with traumatic facial nerve palsy. After a six month follow-up, both patients showed improvement in facial function by 2 grades according to House-Brackmann grade system. In terms of treatment outcomes, total transcanal endoscopic facial nerve decompression for traumatic facial nerve palsy is an alternative for lesions limited to the tympanic segment I, and has an advantages of being minimally invasive and is cosmetically acceptable without an external scar or bony depression due to drilling.
MeSH Terms
Figure
-
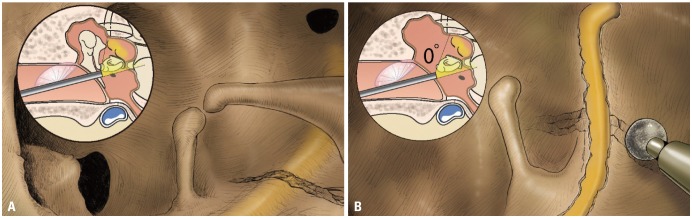
Fig. 1 Schematic drawings of total transcanal endoscopic facial nerve decompression. (A) After tympanomeatal flap elevation, fracture line across the tympanic segment of facial nerve was noted. The disarticulated incudostapedial joint was also found. (B) After removal of malleus and incus, decompression of facial nerve was performed using microdrills. Using this approach, facial nerve can be exposed from geniculate ganglion to second genu.
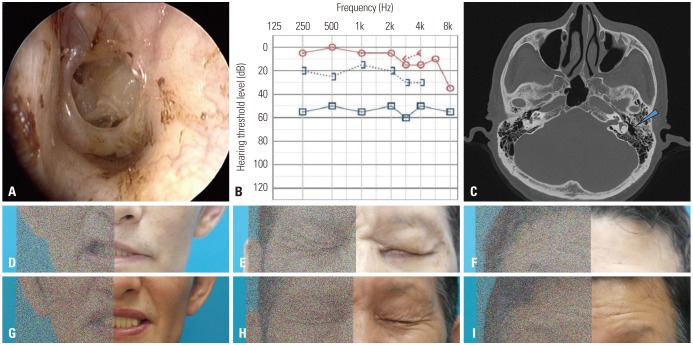
Fig. 2 Otologic manifestations and facial expressions of case 1. (A and B) Traumatic tympanic membrane perforation and conductive hearing loss were noted in the left ear. (C) Pre-operative CT scan, axial view. Note the left temporal bone fracture as shown by the blue arrow. (D-F) Pre-operative and (G-I) six-month post-operative photos of the patient. There was a significant improvement in facial nerve function from House-Brackmann grade IV to II.
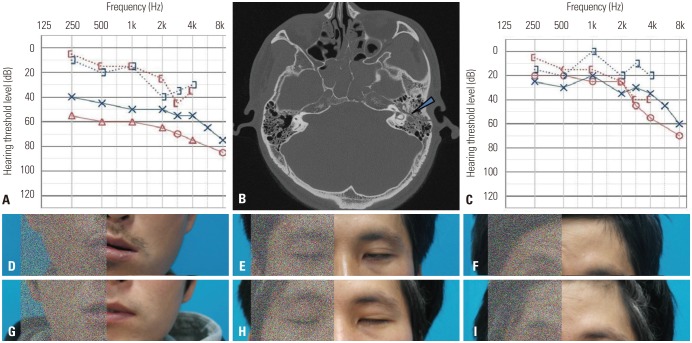
Fig. 3 Otologic manifestations and facial expressions of case 2. (A) Pure tone audiometry showed bilateral conductive hearing loss (average ABG=30 dB). (B) Pre-operative CT scan, axial view. Note the left temporal bone fracture as shown by the blue arrow. (C) Three-month post-operative pure tone audiometry showed improvement. (D-F) Pre-operative and (G-I) five-month post-operative photos of the patient. Patient showed improvement in facial function from House-Brackmann grade V to III.
Reference
-
1. Hato N, Nota J, Hakuba N, Gyo K, Yanagihara N. Facial nerve decompression surgery in patients with temporal bone trauma: analysis of 66 cases. J Trauma. 2011; 71:1789–1792. PMID: 22182890.
Article2. Ulug T, Ulubil SA. Management of facial paralysis in temporal bone fractures: a prospective study analyzing 11 operated fractures. Am J Otolaryngol. 2005; 26:230–238. PMID: 15991088.
Article3. Nash JJ, Friedland DR, Boorsma KJ, Rhee JS. Management and outcomes of facial paralysis from intratemporal blunt trauma: a systematic review. Laryngoscope. 2010; 120:1397–1404. PMID: 20564723.
Article4. Darrouzet V, Duclos JY, Liguoro D, Truilhe Y, De Bonfils C, Bebear JP. Management of facial paralysis resulting from temporal bone fractures: our experience in 115 cases. Otolaryngol Head Neck Surg. 2001; 125:77–84. PMID: 11458219.
Article5. Marchioni D, Alicandri-Ciufelli M, Piccinini A, Genovese E, Monzani D, Tarabichi M, et al. Surgical anatomy of transcanal endoscopic approach to the tympanic facial nerve. Laryngoscope. 2011; 121:1565–1573. PMID: 21671230.
Article6. Marchioni D, Molteni G, Presutti L. Endoscopic anatomy of the middle ear. Indian J Otolaryngol Head Neck Surg. 2011; 63:101–113. PMID: 22468244.
Article7. Marchioni D, Alicandri-Ciufelli M, Mattioli F, Nogeira JF, Tarabichi M, Villari D, et al. From external to internal auditory canal: surgical anatomy by an exclusive endoscopic approach. Eur Arch Otorhinolaryngol. 2013; 270:1267–1275. PMID: 23010794.
Article8. Marchioni D, Soloperto D, Rubini A, Nogueira JF, Badr-El-Dine M, Presutti L. Endoscopic facial nerve surgery. Otolaryngol Clin North Am. 2016; 49:1173–1187. PMID: 27468633.
Article9. Liu Y, Han J, Zhou X, Gao K, Luan D, Xie F, et al. Surgical management of facial paralysis resulting from temporal bone fractures. Acta Otolaryngol. 2014; 134:656–660. PMID: 24665853.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Report of facial nerve decompression in the traumatic facial palsy
- Facial Nerve Paralysis and Surgical Management
- Facial Nerve Decompression for Bell's Palsy: An Endless Debate
- Facial Nerve Decompression via Middle Fossa Approach: Report of Three Cases
- Facial Nerve Decompression for Facial Nerve Palsy with Temporal Bone Fracture: Analysis of 25 Cases
