Corrective Septorhinoplasty in Acute Nasal Bone Fractures
- Affiliations
-
- 1Department of Otorhinolaryngology-Head and Neck Surgery, Chungbuk National University Hospital, Chungbuk National University College of Medicine, Cheongju, Korea. hwatas@naver.com
- KMID: 2407792
- DOI: http://doi.org/10.21053/ceo.2017.00346
Abstract
OBJECTIVES
Closed reduction is generally recommended for acute nasal bone fractures, and rhinoplasty is considered in cases with an unsatisfactory outcome. However, concomitant rhinoplasty with fracture reduction might achieve better surgical outcomes. This study investigated the surgical techniques and outcomes in patients who underwent rhinoplasty and fracture reduction concomitantly, during the acute stage of nasal bone fracture.
METHODS
Forty-five patients who underwent concomitant rhinoplasty and fracture reduction were enrolled. Nasal bone fractures were classified into three major types (type I, simple fracture; type II, fracture line that mimics nasal osteotomy; and type III, comminuted fracture) based on computed tomography images and preoperative facial images. Two independent otolaryngology-head and neck surgeons evaluated the surgical outcomes and telephone based survey were made to evaluate patients satisfaction.
RESULTS
Among 45 patients, there were 39 males and 6 females. Type I was the commonest type of fracture with 18 patients (40%), while the most frequently used surgical technique for corrective surgery was dorsal augmentation with 44 patients (97.8%). The mean visual analogue scale satisfaction score of the surgeons and patients were 7.62 and 8, respectively, with no significant differences between fracture types.
CONCLUSION
Concomitant rhinoplasty with fracture reduction can be performed for acute nasal bone fracture patients, and it might lead to better aesthetic outcomes.
Keyword
Figure
-
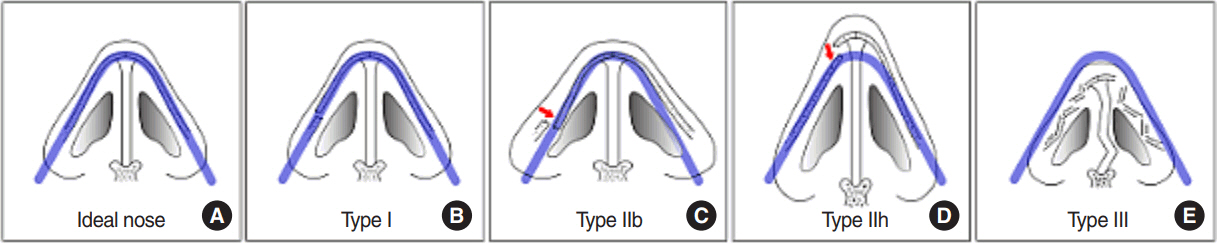
Fig. 1. Types of nasal bone fractures. Blue line indicates an ideal shape and location of the nasal bone. (A) Aesthetically ideal bony pyramid. (B) Type I, minimally displaced nasal bone fracture, which remains within the blue line. (C) Type IIb, a broad based nose, with unaffected bone outside the blue line and the fractured bone inside the blue line. (D) Type IIh, a hump nose with intact bone above the blue line and fractured bone inside the blue line. (E) Type III, comminuted fracture with a septal fracture where all components collapse away from the blue line. Arrows indicate directions of displacement of fracture site in favorable way.
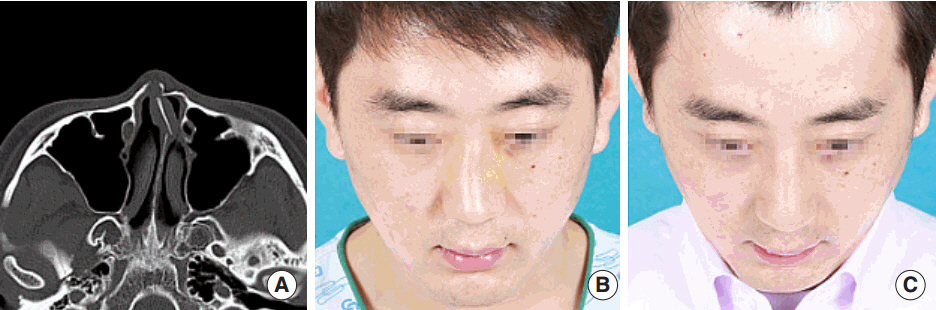
Fig. 2. Facial photographs and computed tomography (CT) image of case 1. (A) Preoperative facial bone CT shows a broad base bony pyramid with left nasal bone fracture. The fracture line mimics a lateral osteotomy. (B) Preoperative facial photograph shows a right side broad base nose. (C) Postoperative facial photograph shows a well-corrected broad base nose.
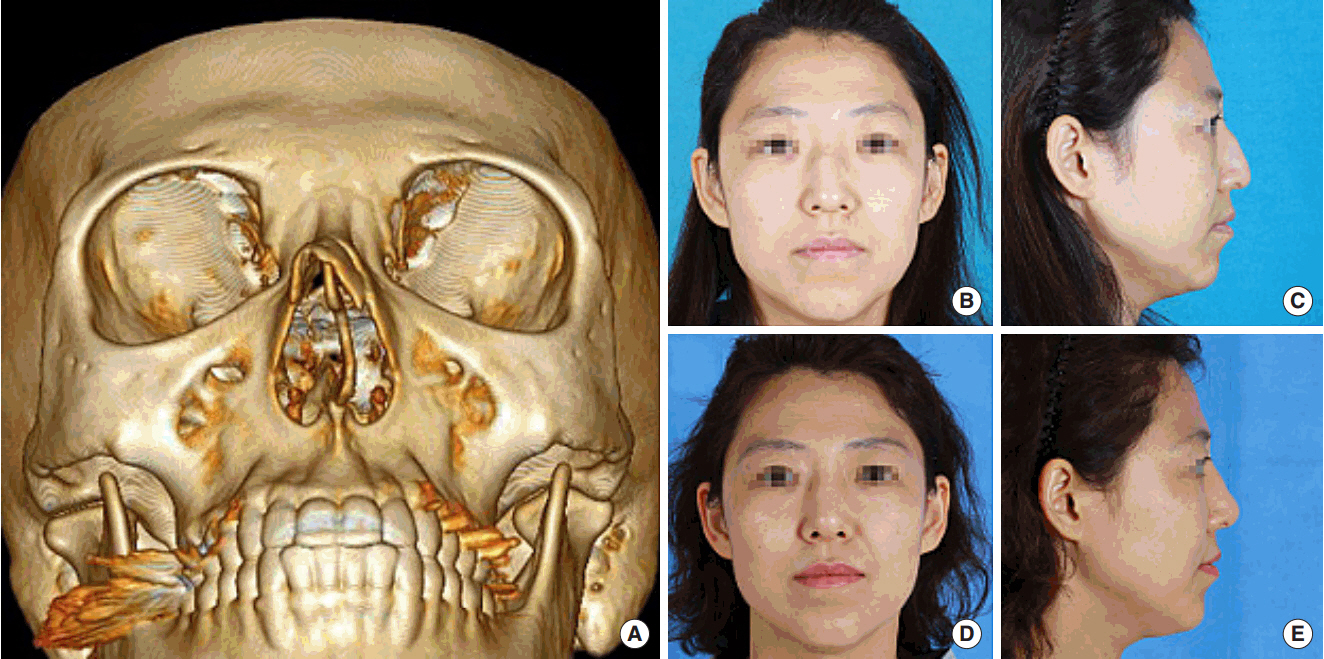
Fig. 3. Facial photographs and three-dimensionally reconstructed computed tomography (CT) image of case 2. (A) Preoperative three-dimensionally reconstructed CT image shows a hump nose with left nasal bone fracture. The fracture lines mimic a medial and lateral osteotomies. (B, C) Preoperative facial photographs show a hump nose with right side deviation. (D, E) Postoperative facial photograph shows a well-corrected hump nose.
Reference
-
1. Rhee SC, Kim YK, Cha JH, Kang SR, Park HS. Septal fracture in simple nasal bone fracture. Plast Reconstr Surg. 2004; Jan. 113(1):45–52.
Article2. Murray JA, Maran AG, Mackenzie IJ, Raab G. Open v closed reduction of the fractured nose. Arch Otolaryngol. 1984; Dec. 110(12):797–802.3. Haug RH, Prather JL. The closed reduction of nasal fractures: an evaluation of two techniques. J Oral Maxillofac Surg. 1991; Dec. 49(12):1288–92.
Article4. Renner GJ. Management of nasal fractures. Otolaryngol Clin North Am. 1991; Feb. 24(1):195–213.
Article5. Pollock RA. Nasal trauma: pathomechanics and surgical management of acute injuries. Clin Plast Surg. 1992; Jan. 19(1):133–47.6. Mondin V, Rinaldo A, Ferlito A. Management of nasal bone fractures. Am J Otolaryngol. 2005; May-Jun. 26(3):181–5.
Article7. Watson DJ, Parker AJ, Slack RW, Griffiths MV. Local versus general anaesthetic in the management of the fractured nose. Clin Otolaryngol Allied Sci. 1988; Dec. 13(6):491–4.
Article8. Rohrich RJ, Adams WP Jr. Nasal fracture management: minimizing secondary nasal deformities. Plast Reconstr Surg. 2000; Aug. 106(2):266–73.
Article9. Murray JA, Maran AG. The treatment of nasal injuries by manipulation. J Laryngol Otol. 1980; Dec. 94(12):1405–10.
Article10. Fernandes SV. Nasal fractures: the taming of the shrewd. Laryngoscope. 2004; Mar. 114(3):587–92.
Article11. Staffel JG. Optimizing treatment of nasal fractures. Laryngoscope. 2002; Oct. 112(10):1709–19.
Article12. Clark WD, Stiernberg CM. Early aggressive treatment of nasal fractures. Ear Nose Throat J. 1986; Oct. 65(10):481–3.13. Kim JH, Lee JW, Park CH. Cosmetic rhinoseptoplasty in acute nasal bone fracture. Otolaryngol Head Neck Surg. 2013; Aug. 149(2):212–8.
Article14. Chen CT, Hu TL, Lai JB, Chen YC, Chen YR. Reconstruction of traumatic nasal deformity in Orientals. J Plast Reconstr Aesthet Surg. 2010; Feb. 63(2):257–64.
Article15. Wong CH, Daniel RK. Immediate functional and cosmetic open rhinoplasty following acute nasal fractures: our experience with Asian noses. Aesthet Surg J. 2013; May. 33(4):505–15.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Clinical Study of Patients that Rhinoplasty was Performed Concomitantly with Nasal Bone Fracture Reduction
- The Clinical Effectiveness of Open Septorhinoplasty for Primary Treatment of Nasal bone Fracture
- Complications After Inadequate Treatment of Nasal Bone Fracture Combined With Septal Fracture: A Case Report
- Usefulness of Ultrasonography-Assisted Closed Reduction for Nasal Fracture under Local Anesthesia
- The Current Knowledge of the Treatment of Nasal Bone Fractures
