Accessory Talar Facet Impingement due to Accessory Anterolateral Talar Facet Misdiagnosed as Sinus Tarsi Syndrome
- Affiliations
-
- 1Department of Orthopaedic Surgery, Yeungnam University Hospital, Yeungnam University College of Medicine, Daegu, Korea. chpark77@naver.com
- KMID: 2407370
- DOI: http://doi.org/10.14193/jkfas.2018.22.1.16
Abstract
- PURPOSE
To evaluate the clinical and radiographic results of surgical treatment for patients with sinus tarsi pain due to accessory talar facet impingement.
MATERIALS AND METHODS
Between July 2013 and July 2015, nine patients who underwent surgery for the accessory talar facet impingement were reviewed. The mean follow-up period was 18.6 months (12~36 months), and the mean age was 33.1 years (19~60 years). Previous trauma history, duration of symptom, and types of surgery were analyzed. The clinical results were evaluated using the American Orthopaedic Foot and Ankle Society (AOFAS) ankle-hindfoot score and visual analogue scale (VAS). Radiographic results were assessed using Meary's angle, calcaneal pitch angle, heel alignment angle, and heel alignment ratio.
RESULTS
All patients had evident trauma history prior to the initial symptom. The mean duration of symptoms was 25.6 months (6~120 months). Four patients received only accessory anterolateral talar facet (AALTF) excision, and four patients received medial sliding calcaneal osteotomy (MSCO). One patient underwent both AALTF excision and MSCO. The AOFAS ankle-hindfoot score was significantly improved from 73 (62~77) preoperatively to 93 (67~100) postoperatively. The VAS score was decreased from 6 (5~7) preoperatively to 1 (0~5) postoperatively. The Meary's angle and calcaneal pitch angle showed no significant difference after surgery. The heel alignment angle and ratio increased from −3.6° (−10°~5°) and 0.22 (−0.15~0.6) preoperatively to 2.8° (1°~5°) and 0.42 (0.3~0.6) postoperatively, respectively.
CONCLUSION
If there is persistent sinus tarsi pain in patients with hindfoot valgus, accessory talar facet impingement caused by AALTF could be considered as a cause of chronic sinus tarsi pain.
Figure
-

Figure 1 A 33-year-old man with pain on sinus tarsi after severe ankle sprain. Magnetic resonance imaging shows cartilage continuity between articular surface of talar facet and focal abutting bone marrow edema (arrows).
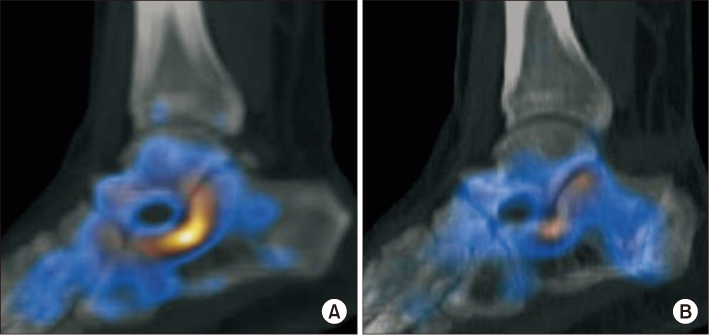
Figure 2 A) Preoperative single photon emission computed tomography/computed tomography (SPECT/CT) shows diffuse uptake at the calcaneus. (B) SPECT/CT taken 1 year after surgery shows decreased uptake at the calcaneus.

Figure 3 Subtalar arthroscopy shows partial tear of the interosseous talocalcaneal ligament (a) and the posterior facet of calcaneus (b).
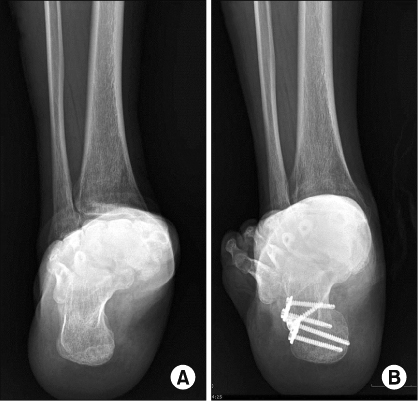
Figure 4 (A) Preoperative hindfoot alignment radiograph shows hindfoot valgus deformity, and (B) hindfoot valgus is corrected after medial sliding calcaneal osteotomy.
Cited by 1 articles
-
Various Pathologic Conditions of Sinus Tarsi Syndrome Assessed by Imaging and Arthroscopic Findings
Jeong Jin Park, Seung Jae Cho, Seong Hyeon Jo, Chul Hyun Park
J Korean Foot Ankle Soc. 2024;28(2):60-67. doi: 10.14193/jkfas.2024.28.2.60.
Reference
-
1. O'Connor D. The sinus tarsi syndrome. A clinical entity. J Bone Joint Surg. 1958; 40:720.2. Frey C, Feder KS, DiGiovanni C. Arthroscopic evaluation of the subtalar joint: does sinus tarsi syndrome exist? Foot Ankle Int. 1999; 20:185–191.
Article3. Pisani G, Pisani PC, Parino E. Sinus tarsi syndrome and subtalar joint instability. Clin Podiatr Med Surg. 2005; 22:63–77.
Article4. Martus JE, Femino JE, Caird MS, Hughes RE, Browne RH, Farley FA. Accessory anterolateral facet of the pediatric talus. An anatomic study. J Bone Joint Surg Am. 2008; 90:2452–2459.5. Niki H, Hirano T, Akiyama Y, Beppu M. Accessory talar facet impingement in pathologic conditions of the peritalar region in adults. Foot Ankle Int. 2014; 35:1006–1014.
Article6. Martus JE, Femino JE, Caird MS, Kuhns LR, Craig CL, Farley FA. Accessory anterolateral talar facet as an etiology of painful talocalcaneal impingement in the rigid flatfoot: a new diagnosis. Iowa Orthop J. 2008; 28:1–8.7. Helgeson K. Examination and intervention for sinus tarsi syndrome. N Am J Sports Phys Ther. 2009; 4:29–37.8. Ha S, Hong SH, Paeng JC, Lee DY, Cheon GJ, Arya A, et al. Comparison of SPECT/CT and MRI in diagnosing symptomatic lesions in ankle and foot pain patients: diagnostic performance and relation to lesion type. PLoS One. 2015; 10:e0117583.
Article9. Ravindra VM, Mazur MD, Bisson EF, Barton C, Shah LM, Dailey AT. The usefulness of single-photon emission computed tomography in defining painful upper cervical facet arthropathy. World Neurosurg. 2016; 96:390–395.
Article10. Sewell RB. A study of the astragalus. J Anat Physiol. 1904; 39:74–88.7.11. Kelikian AS, Sarrafian SK. Sarrafian's anatomy of the foot and ankle: descriptive, topographic, functional. Philadelphia: Lippincott Williams & Wilkins;2011.12. Hirano T, Niki H, Akiyama Y, Beppu M. Anatomical characteristics of the accessory antero-lateral talar facet. J Orthop Sci. 2015; 20:124–128.
Article13. Hattori K, Sakuma E, Nakayama M, Kozaki A, Wada I, Otsuka T. An anatomic study of the accessory anterolateral talar facet. Folia Morphol (Warsz). 2015; 74:61–64.
Article14. Malicky ES, Crary JL, Houghton MJ, Agel J, Hansen ST Jr, Sangeorzan BJ. Talocalcaneal and subfibular impingement in symptomatic flatfoot in adults. J Bone Joint Surg Am. 2002; 84:2005–2009.
Article15. Donovan A, Rosenberg ZS. Extraarticular lateral hindfoot impingement with posterior tibial tendon tear: MRI correlation. AJR Am J Roentgenol. 2009; 193:672–678.
Article16. Neumann JA, Mannava S, Gross CE, Wooster BM, Busch MT. Arthroscopic debridement of pediatric accessory anterolateral talar facet causing impingement. Arthrosc Tech. 2016; 5:e413–e417.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Various Pathologic Conditions of Sinus Tarsi Syndrome Assessed by Imaging and Arthroscopic Findings
- Treatment of Facet Joint Syndrome
- Tram Track Lesion of the Talar Dome
- Arthrography of the lumbar facet joint and facet block
- Three-Dimensional Volume Analysis of Partial Avascular Necrosis after Talar Neck Fracture
