A comparison between the right side and the left side of head skin in a patient who received more than 450 sessions of left stellate ganglion block: A case report
- Affiliations
-
- 1Department of Anesthesiology and Pain Medicine, Dankook University College of Medicine, Cheonan, Korea. leemose@dankook.ac.kr
- 2Department of Dermatology, Dankook University College of Medicine, Cheonan, Korea.
- KMID: 2405857
- DOI: http://doi.org/10.17085/apm.2017.12.4.371
Abstract
- Stellate ganglion block (SGB) is an effective method that is used by pain clinicians to treat patients who have pain in the head, neck and arm area. SGB acts mainly by increasing regional blood flow via peripheral vasodilation and decreasing pain sensation by reducing the afferent sensory signals of the sympathetic nervous system in the region. This patient had received more than 450 sessions of left SGB continually for the past 6 years to relieve her left-sided facial pain caused by facial trauma. Out of our curiosity, we tried to obtain some objective dermatological measurements like skin elasticity, water content, and hair follicle density on her scalp and we found that the values were different between the left side of her face and the right side of her face. Here, we report the results and we want pain clinicians to know that repeated SGBs may improve skin elasticity, water content in the skin, and increase the number of hair follicles on the scalp.
MeSH Terms
Figure
-
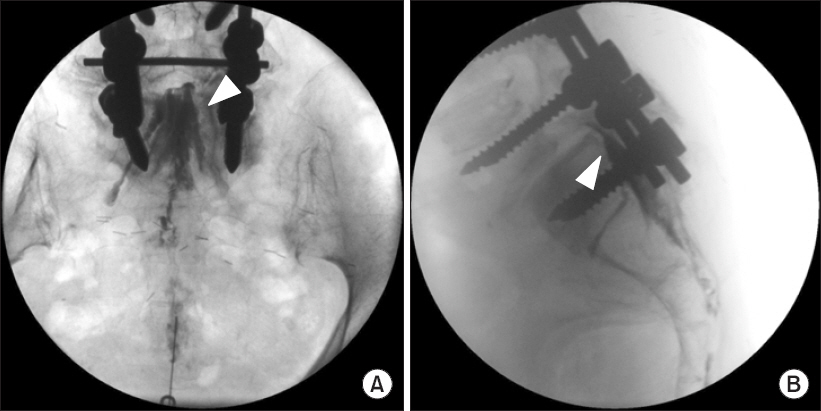
Fig. 1 Fluoroscopic images of contrast spread after caudal epidural block. (A) Anteroposterior view of contrast spread. (B) Lateral view of contrast spread. Arrowhead: contrast spread in the epidural space.
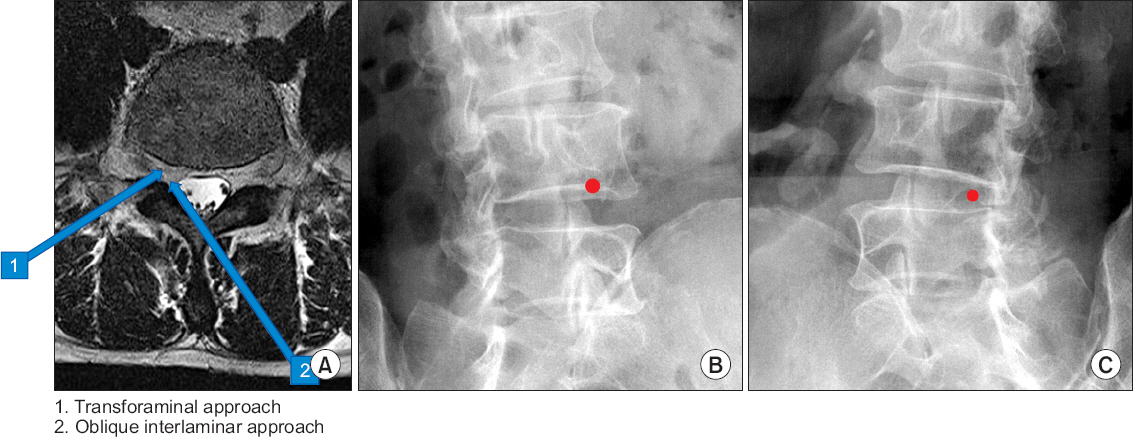
Fig. 2 Comparison of transforaminal versus oblique interlaminar approach. (A) Needle entry points of transforaminal approach versus oblique interlaminar approach. (B) Initial needle entry point of right transforaminal approach. (C) Initial needle entry point of right oblique interlaminar approach.
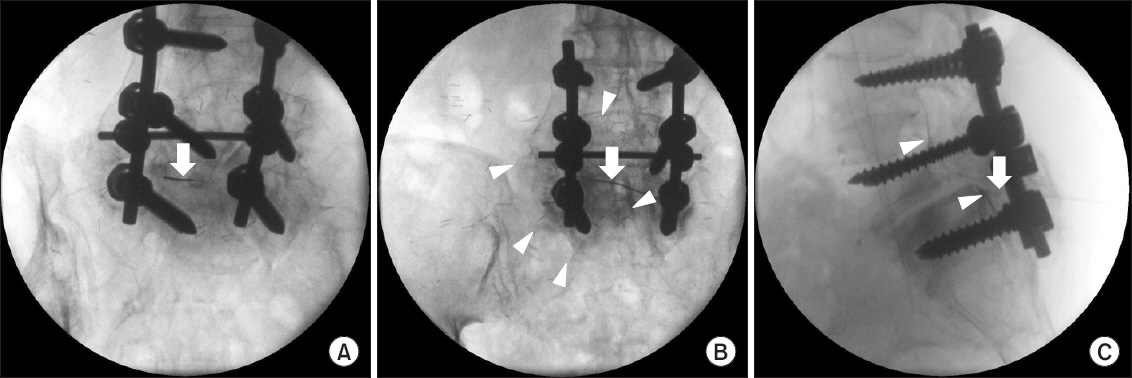
Fig. 3 Fluoroscopic images of contrast spread after oblique interlaminar approach. (A) Initial entry point of right oblique L5-S1 interlaminar approach. (B) Anteroposterior view of contrast spread. (C) Lateral view of contrast spread. Arrow: a 22-G, 80-mm Tuohy needle, Arrowhead: contrast spread in the epidural space.
Reference
-
1. Abdi S, Datta S, Lucas LF. Role of epidural steroids in the management of chronic spinal pain:a systematic review of effectiveness and complications. Pain Physician. 2005; 8:127–43. PMID: 16850050.2. Quintero N, Laffont I, Bouhmidi L, Rech C, Schneider AE, Gavardin T, et al. Transforaminal epidural steroid injection and paraplegia:case report and bibliographic review. Ann Readapt Med Phys. 2006; 49:242–7. DOI: 10.1016/j.annrmp.2006.03.004. PMID: 16675057.3. Candido KD, Raghavendra MS, Chinthagada M, Badiee S, Trepashko DW. A prospective evaluation of iodinated contrast flow patterns with fluoroscopically guided lumbar epidural steroid injections:the lateral parasagittal interlaminar epidural approach versus the transforaminal epidural approach. Anesth Analg. 2008; 106:638–44. DOI: 10.1213/ane.0b013e3181605e9b. PMID: 18227326.4. Jeong JS, Shim JC, Woo JP, Shim JH, Kim DW, Kim KS. Epidural contrast flow patterns of retrograde interlaminar ventral epidural injections stratified by the final catheter tip placement. Anesth Pain Med. 2013; 8:158–65.5. Kraemer J, Ludwig J, Bickert U, Owczarek V, Traupe M. Lumbar epidural perineural injection:a new technique. Eur Spine J. 1997; 6:357–61. DOI: 10.1007/BF01142687. PMID: 9391811. PMCID: PMC3454603.6. Sizer PS Jr, Phelps V, Dedrick G, Matthijs O. Differential diagnosis and management of spinal nerve root-related pain. Pain Pract. 2002; 2:98–121. DOI: 10.1046/j.1533-2500.2002.02012.x. PMID: 17147684.7. Cavanaugh JM. Neural mechanisms of lumbar pain. Spine (Phila Pa 1976). 1995; 20:1804–9. DOI: 10.1097/00007632-199508150-00011.8. Saal JS, Franson RC, Dobrow R, Saal JA, White AH, Goldthwaite N. High levels of inflammatory phospholipase A2 activity in lumbar disc herniations. Spine (Phila Pa 1976). 1990; 15:674–8. DOI: 10.1097/00007632-199007000-00011.9. Lee HM, Weinstein JN, Meller ST, Hayashi N, Spratt KF, Gebhart GF. The role of steroids and their effects on phospholipase A2. An animal model of radiculopathy. Spine (Phila Pa 1976). 1998; 23:1191–6. DOI: 10.1097/00007632-199806010-00001.10. Rahimzadeh P, Sharma V, Imani F, Faiz HR, Ghodraty MR, Nikzad-Jamnani AR, et al. Adjuvant hyaluronidase to epidural steroid improves the quality of analgesia in failed back surgery syndrome:a prospective randomized clinical trial. Pain Physician. 2014; 17:E75–82. PMID: 24452659.11. Park AR, Kim WM, Heo BH. Delayed allergic reaction to secondary administrated epidural hyaluronidase. Korean J Pain. 2015; 28:153–5. DOI: 10.3344/kjp.2015.28.2.153. PMID: 25852839. PMCID: PMC4387462.12. Lutz GE, Vad VB, Wisneski RJ. Fluoroscopic transforaminal lumbar epidural steroids:an outcome study. Arch Phys Med Rehabil. 1998; 79:1362–6. DOI: 10.1016/S0003-9993(98)90228-3.13. Manchikanti L. Transforaminal lumbar epidural steroid injections. Pain Physician. 2000; 3:374–98. PMID: 16906179.14. Botwin KP, Natalicchio J, Hanna A. Fluoroscopic guided lumbar interlaminar epidural injections:a prospective evaluation of epidurography contrast patterns and anatomical review of the epidural space. Pain Physician. 2004; 7:77–80. PMID: 16868616.15. Botwin KP, Gruber RD, Bouchlas CG, Torres-Ramos FM, Freeman TL, Slaten WK. Complications of fluoroscopically guided transforaminal lumbar epidural injections. Arch Phys Med Rehabil. 2000; 81:1045–50. DOI: 10.1053/apmr.2000.7166. PMID: 10943753.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Bilateral Facial Nerve Palsy Treated with Serial Stellate Ganglion Block
- Stellate Ganglion Block for Shoulder Hand Syndrome following Hemiplegia
- Blood Pressure, Pulse Rate and Temperature Changes of the Ipsilateral Upper Extremity after Unilateral Stellate Ganglion Block
- Percutaneous Radiofrequency Thermocoagulation of Stellate Ganglion
- Continuous Stellate Ganglion Block for Raynaud'S Disease
