J Korean Ophthalmol Soc.
2018 Feb;59(2):169-175. 10.3341/jkos.2018.59.2.169.
Clinical Characteristics and Outcomes of Smartphone Overusers with Acute Acquired Comitant Esotropia
- Affiliations
-
- 1Department of Ophthalmology Chungbuk National University College of Medicine, Cheongju, Korea. mychoi@chungbuk.ac.kr
- KMID: 2403811
- DOI: http://doi.org/10.3341/jkos.2018.59.2.169
Abstract
- PURPOSE
To evaluate the clinical features and treatment outcomes of smartphone overusers with acute acquired comitant esotropia.
METHODS
We retrospectively reviewed the medical records of patients ≥ 15 years of age who used a smartphone for > 4 hours a day for > 1 year, and who were diagnosed with acute acquired comitant esotropia from May 2011 to January 2016. We analyzed sex, age at the time of manifestation and duration of esotropia, refractive error, deviated angle at the first and final visits, and the results of refraining from smartphone use, use of the Fresnel prism, and surgery for esotropia.
RESULTS
A total of 13 patients were studied, including 8 males and 5 females. The mean age at development of esotropia was 22.7 ± 9.7 years. The mean duration of esotropia before the first visit was 28.0 ± 33.0 months, and the mean follow-up period was 16.4 ± 16.4 months. The mean angle of esotropia was 21.8 ± 7.0 prism diopters (PD) at distance and 22.2 ± 7.9 PD at near. There were eight myopic patients; the other patients were emmetropia. The esotropia of all patients did not improve after refraining from smartphone use. There was no improvement in five patients who were wearing the Fresnel prism for ≥ 4 months. A total of six patients were treated with bilateral medial rectus recession; only one patient remained orthotropic at postoperative 6 months, three patients were undercorrected, and two had a recurrence.
CONCLUSIONS
Esotropia persisted after refraining from smartphone use or wearing a Fresnel prism in acute acquired comitant esotropia patients who were smartphone overusers, and the surgical prognosis of these patients was relatively poor.
Keyword
MeSH Terms
Figure
-
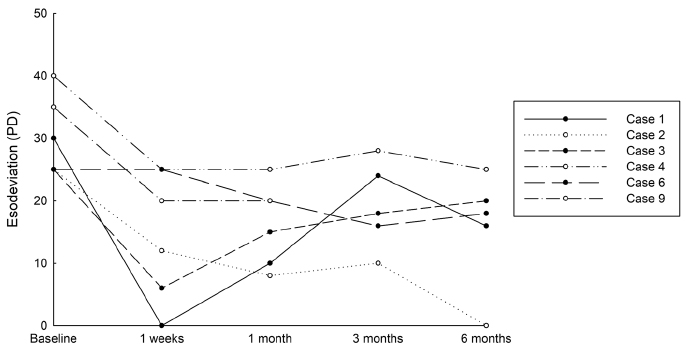
Figure 1 The course after first surgery of 6 patients who were performed bilateral medial rectus recession. Only one patient (Case 2) achieved orthotropia at postoperative 6 months. Two patients (Case 1, 3), showed good alignment within 10 prism diopter at postoperative 1 week, but the angles of esotropia were increased. The other 3 patients were undercorrected.
Reference
-
1. Clark AC, Nelson LB, Simon JW, et al. Acute acquired comitant esotropia. Br J Ophthalmol. 1989; 73:636–638.
Article2. von Noorden GK. Binocular Vision and Ocular Motility: Theory and Management of Strabismus. 6th ed: St Louis: C.V. Mosby Company;2002. p. 324–325.3. Williams AS, Hoyt CS. Acute comitant esotropia in children with brain tumors. Arch Ophthalmol. 1989; 107:376–378.
Article4. Lee JM, Kim SH, Lee JI, et al. Acute comitant esotropia in a child with a cerebellar tumor. Korean J Ophthalmol. 2009; 23:228–231.
Article5. Musazadeh M, Hartmann K, Simon F. Late onset esotropia as first symptom of a cerebellar tumor. Strabismus. 2004; 12:119–123.
Article6. Burian HM, Miller JE. Comitant convergent strabismus with acute onset. Am J Ophthalmol. 1958; 45(4 Pt 2):55–64.
Article7. Lee HS, Park SW, Heo H. Acute acquired comitant esotropia related to excessive smartphone use. BMC ophthalmol. 2016; 16:37.
Article8. Kwon MS, Nam KW, Seo BK. The Survey on Internet Overdependence. 1st ed. Seoul: Ministry of Science, ICT, and Future Planning, National Information Society Agency;2016. p. 27–54.9. Oh CS. A case of acute concomitant esotropia with central corneal ulcer. J Korean Ophthalmol Soc. 1984; 25:303–305.10. Hussaindeen JR, Mani R, Agarkar S, et al. Acute adult onset comitant esotropia associated with accommodative spasm. Optom Vis Sci. 2014; 91:4 Suppl 1. S46–S51.
Article11. Ishikawa S. Examination of the near triad in VDU operators. Ergonomics. 1990; 33:787–798.
Article12. Savino G, Abed E, Rebecchi MT, et al. Acute acquired concomitant esotropia and decompensated monofixation syndrome: a sensorymotor status assessment. Can J Ophthalmol. 2016; 51:258–264.
Article13. Spierer A. Acute concomitant esotropia of adulthood. Ophthalmology. 2003; 110:1053–1056.
Article14. Kim YT, Kim MM. Clinical aspect of acute comitant esotropia. J Korean Ophthalmol Soc. 2002; 43:539–543.15. Meyer E, Ludatscher RM, Lichtig C, et al. End-stage fibrosis of the lateral rectus muscle in myopia with esotropia. An ultrastructural study. Ophthalmic Res. 1990; 22:259–264.16. Repka MX, Connett JE, Scott WE. The one-year surgical outcome after prism adaptation for the management of acquired esotropia. Ophthalmology. 1996; 103:922–928.
Article17. Velez FG, Rosenbaum AL. Preoperative prism adaptation for acquired esotropia: long-term results. J AAPOS. 2002; 6:168–173.
Article18. Jotterand VH, Isenberg SJ. Enhancing surgery for acquired esotropia. Ophthalmic Surg. 1988; 19:263–266.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Two Cases of Acute Acquired Comitant Esotropia after Occlusion Therapy
- Two Cases of Acute Acquired Comitant Esotropia
- Acute Acquired Comitant Esotropia Associated with Chiari I Malformation
- Clinical Characteristics and Outcomes after Augmented Medial Rectus Muscle Recession in Patients with Acute Acquired Comitant Esotropia
- Clinical Aspect of Acute Comitant Esotropia
