Cancer Res Treat.
2015 Oct;47(4):862-870. 10.4143/crt.2014.203.
Long-Term Outcome of Definitive Radiotherapy for Early Glottic Cancer: Prognostic Factors and Patterns of Local Failure
- Affiliations
-
- 1Department of Radiation Oncology, Seoul National University College of Medicine, Seoul, Korea. wuhg@snu.ac.kr
- 2Cancer Research Institution, Seoul National University College of Medicine, Seoul, Korea.
- 3Institute of Radiation Medicine, Medical Research Center, Seoul National University, Seoul, Korea.
- 4Department of Otorhinolaryngology-Head and Neck Surgery, Seoul National University College of Medicine, Seoul, Korea.
- KMID: 2403406
- DOI: http://doi.org/10.4143/crt.2014.203
Abstract
- PURPOSE
This study evaluates the long-term results of definitive radiotherapy (RT) for early glottic cancer. Clinical and treatment factors related to local control and patterns of failure are analyzed.
MATERIALS AND METHODS
We retrospectively reviewed 222 patients with T1-2N0 squamous cell carcinoma of the glottic larynx treated with definitive RT from 1981 to 2010. None of the patients received elective nodal RT or combined chemotherapy. The median total RT dose was 66 Gy. The daily fraction size was < 2.5 Gy in 69% and 2.5 Gy in 31% of patients. The RT field extended from the hyoid bone to the cricoid cartilage.
RESULTS
The median age was 60 years, and 155 patients (70%) had T1 disease. The 5-year rates of local recurrence-free survival (LRFS) and ultimate LRFS with voice preservation were 87.8% and 90.3%, respectively. T2 (hazard ratio [HR], 2.30; 95% confidence interval [CI], 1.08 to 4.94) and anterior commissural involvement (HR, 3.37; 95% CI, 1.62 to 7.02) were significant prognostic factors for LRFS. In 34 patients with local recurrence, tumors recurred in the ipsilateral vocal cord in 28 patients. There were no contralateral vocal cord recurrences. Most acute complications included grade 1-2 dysphagia and/or hoarseness. There was no grade 3 or greater chronic toxicity.
CONCLUSION
Definitive RT achieved a high cure rate, voice preservation, and tolerable toxicity in early glottic cancer. T2 stage and anterior commissural involvement were prognostic factors for local control. Further optimization of the RT method is needed to reduce the risk of ipsilateral tumor recurrence.
Keyword
MeSH Terms
Figure
-

Fig. 1. Kaplan-Meier curve for local recurrence-free survival (A) and ultimate local recurrence-free survival (B) with voice preservation.
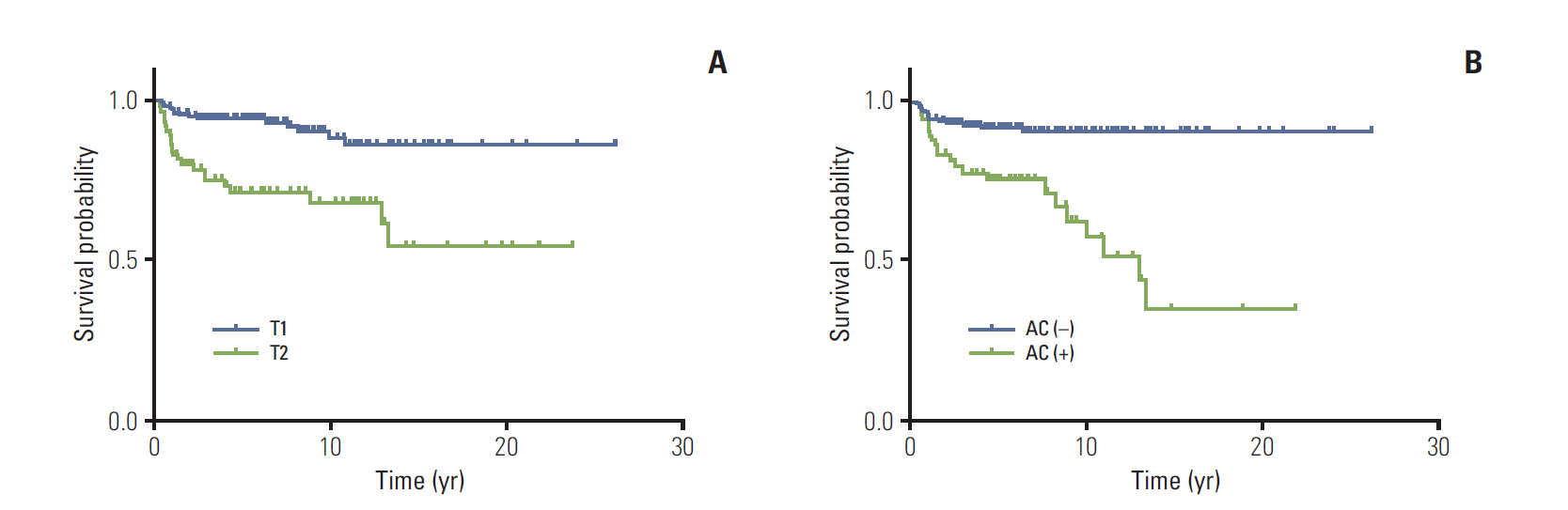
Fig. 2. Local recurrence-free survival according to T-stage (T1 vs. T2, p < 0.001) (A) and anterior commissural involvement (no vs. yes, p < 0.001) (B) by Kaplan-Meier analyses. AC, anterior commissure.

Fig. 3. Local recurrence-free survival according to fraction size (2.5 Gy vs. < 2.5 Gy, p=0.042) (A) and overall treatment time (< 50 days vs. ≥ 50 days, p=0.001) (B) by Kaplan-Meier analyses.
Reference
-
References
1. Park CI, Shin KH, Park SW, Shin SS, Kim KH. Prognostic factors for local control and survival in T1-T2 glottic cancer. J Korean Cancer Assoc. 1997; 29:984–91.2. American Society of Clinical Oncology, Pfister DG, Laurie SA, Weinstein GS, Mendenhall WM, Adelstein DJ, et al. American Society of Clinical Oncology clinical practice guideline for the use of larynx-preservation strategies in the treatment of laryngeal cancer. J Clin Oncol. 2006; 24:3693–704.
Article3. Taylor SM, Kerr P, Fung K, Aneeshkumar MK, Wilke D, Jiang Y, et al. Treatment of T1b glottic SCC: laser vs. radiation: a Canadian multicenter study. J Otolaryngol Head Neck Surg. 2013; 42:22.
Article4. Mendenhall WM, Mancuso AA, Amdur RJ, Werning JW. Early vocal cord carcinoma. In : Halperin EC, Wazer DE, Perez CA, Brady LW, editors. Perez and Brady’s principles and practice of radiation oncology. 6th ed. Philadelphia, PA: Lippincott Williams & Wilkins;2013. p. 856.5. Rodel RM, Steiner W, Muller RM, Kron M, Matthias C. Endoscopic laser surgery of early glottic cancer: involvement of the anterior commissure. Head Neck. 2009; 31:583–92.
Article6. Kim SJ, Suh CO, Kim GE, Park CY. Radiation therapy of laryngeal cancer. J Korean Cancer Assoc. 1982; 14:3–12.7. Chera BS, Amdur RJ, Morris CG, Kirwan JM, Mendenhall WM. T1N0 to T2N0 squamous cell carcinoma of the glottic larynx treated with definitive radiotherapy. Int J Radiat Oncol Biol Phys. 2010; 78:461–6.
Article8. Khan MK, Koyfman SA, Hunter GK, Reddy CA, Saxton JP. Definitive radiotherapy for early (T1-T2) glottic squamous cell carcinoma: a 20 year Cleveland Clinic experience. Radiat Oncol. 2012; 7:193.
Article9. Tong CC, Au KH, Ngan RK, Cheung FY, Chow SM, Fu YT, et al. Definitive radiotherapy for early stage glottic cancer by 6 MV photons. Head Neck Oncol. 2012; 4:23.
Article10. Kim TG, Ahn YC, Nam HR, Chung MK, Jeong HS, Son YI, et al. Definitive radiation therapy for early glottic cancer: experience of two fractionation schedules. Clin Exp Otorhinolaryngol. 2012; 5:94–100.
Article11. Mourad WF, Hu KS, Shourbaji RA, Woode R, Harrison LB. Long-term follow-up and pattern of failure for T1-T2 glottic cancer after definitive radiation therapy. Am J Clin Oncol. 2013; 36:580–3.
Article12. Fowler JF, Harari PM, Leborgne SP, Li F, Leborgne JH. Acute radiation reactions in oral and pharyngeal mucosa: tolerable levels in altered fractionation schedules. Radiother Oncol. 2003; 69:161–8.
Article13. Qi XS, Yang Q, Lee SP, Li XA, Wang D. An estimation of radiobiological parameters for head-and-neck cancer cells and the clinical implications. Cancers (Basel). 2012; 4:566–80.
Article14. Marshak G, Brenner B, Shvero J, Shapira J, Ophir D, Hochman I, et al. Prognostic factors for local control of early glottic cancer: the Rabin Medical Center retrospective study on 207 patients. Int J Radiat Oncol Biol Phys. 1999; 43:1009–13.
Article15. Tong CC, Au KH, Ngan RK, Chow SM, Cheung FY, Fu YT, et al. Impact and relationship of anterior commissure and time-dose factor on the local control of T1N0 glottic cancer treated by 6 MV photons. Radiat Oncol. 2011; 6:53.
Article16. Nur DA, Oguz C, Kemal ET, Ferhat E, Sulen S, Emel A, et al. Prognostic factors in early glottic carcinoma implications for treatment. Tumori. 2005; 91:182–7.
Article17. Burke LS, Greven KM, McGuirt WT, Case D, Hoen HM, Raben M. Definitive radiotherapy for early glottic carcinoma: prognostic factors and implications for treatment. Int J Radiat Oncol Biol Phys. 1997; 38:1001–6.
Article18. Mendenhall WM, Amdur RJ, Morris CG, Hinerman RW. T1-T2N0 squamous cell carcinoma of the glottic larynx treated with radiation therapy. J Clin Oncol. 2001; 19:4029–36.
Article19. Yamazaki H, Nishiyama K, Tanaka E, Koizumi M, Chatani M. Radiotherapy for early glottic carcinoma (T1N0M0): results of prospective randomized study of radiation fraction size and overall treatment time. Int J Radiat Oncol Biol Phys. 2006; 64:77–82.
Article20. Moon SH, Cho KH, Chung EJ, Lee CG, Lee KC, Chai GY, et al. A prospective randomized trial comparing hypofractionation with conventional fractionation radiotherapy for T1-2 glottic squamous cell carcinomas: results of a Korean Radiation Oncology Group (KROG-0201) study. Radiother Oncol. 2014; 110:98–103.
Article21. Levendag PC, Teguh DN, Keskin-Cambay F, Al-Mamgani A, van Rooij P, Astreinidou E, et al. Single vocal cord irradiation: a competitive treatment strategy in early glottic cancer. Radiother Oncol. 2011; 101:415–9.
Article22. Chera BS, Amdur RJ, Morris CG, Mendenhall WM. Carotidsparing intensity-modulated radiotherapy for early-stage squamous cell carcinoma of the true vocal cord. Int J Radiat Oncol Biol Phys. 2010; 77:1380–5.
Article23. Osman SO, Astreinidou E, de Boer HC, Keskin-Cambay F, Breedveld S, Voet P, et al. IMRT for image-guided single vocal cord irradiation. Int J Radiat Oncol Biol Phys. 2012; 82:989–97.
Article24. Le QT, Fu KK, Kroll S, Ryu JK, Quivey JM, Meyler TS, et al. Influence of fraction size, total dose, and overall time on local control of T1-T2 glottic carcinoma. Int J Radiat Oncol Biol Phys. 1997; 39:115–26.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Radiotherapy of Early Stage Glottic Cancer
- Analysis on the Treatment Outcome of Early Glottic Cancer
- Radiotherapy Versus Cordectomy in the Management of Early Glottic Cancer
- Prognostic Factors for Local Control in Early Glottic Cancer Treated with Radiation Therapy
- Results of Radiation Therapy in Early Glottic Cancer
