Temporary Haptic Externalization and Four-point Fixation of Intraocular Lens in Scleral Fixation to Enhance Stability
- Affiliations
-
- 1Department of Ophthalmology, VHS Medical Center, Seoul, Korea.
- 2Department of Ophthalmology, Seoul National University Hospital, Seoul National University College of Medicine, Seoul, Korea. hjw68@snu.ac.kr
- KMID: 2402716
- DOI: http://doi.org/10.3341/kjo.2017.0038
Abstract
- PURPOSE
To report the results of a new technique for intraocular lens scleral fixation of temporary haptic externalization and four-point fixation for enhanced stability.
METHODS
Two 10-0 polypropylene strands were fixed at two points 2 mm apart on each haptic of a conventional three-piece intraocular lens, using our previously reported method of temporary haptic externalization after injector implantation. Postoperative refractive outcome and stability were evaluated.
RESULTS
Although the intraocular lens was fixed at a total of four points, no intraoperative difficulties were observed during the process. Patients showed successful fixation of the intraocular lens postoperatively. The fixed intraocular lens showed good centering and minimal tilting. When compared to the two-point fixation technique, postoperative astigmatism was significantly smaller in the four-point fixation group (1.80 ± 0.84 vs. 1.00 ± 0.0.50, p = 0.033). Lens-induced astigmatism calculated from subtraction of corneal astigmatism from total astigmatism was also significantly smaller in the four-point fixation group (2.23 ± 0.98 vs.1.17 ± 0.0.70, p = 0.043). No postoperative complications were identified during a mean follow-up period of 14.8 months (range, 10 to 19 months).
CONCLUSIONS
By fixing the intraocular lens at two points on each side of the haptics, this method minimizes the tilting of the intraocular lens and thus decreases postoperative lens-induced astigmatism. Also, the possibility of intraocular lens dislocation in the long term might be decreased by this two-point fixation technique.
Keyword
MeSH Terms
Figure
-
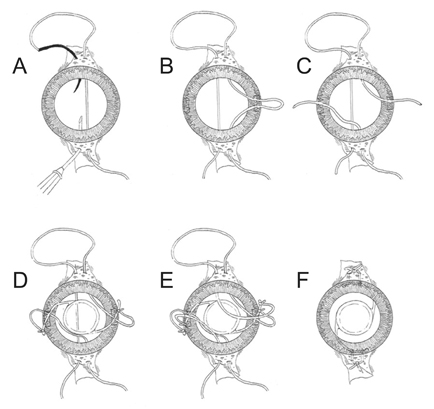
Fig. 1 Schematic drawing of the procedure of temporary haptic externalization and four-point fixation in scleral fixation of the intraocular lens (surgeon's view from the superior of eye). (A) Double-armed 10–0 polypropylene sutures are passed through the sclera and across to the opposite side. (B) The suture thread closer to the 3 o'clock side is pulled through the 3 o'clock corneal incision and cut in two. (C) 12 o'clock end is pulled out through the 9 o'clock corneal incision. (D,E) A 3-piece intraocular lens is inserted through the 3 o'clock corneal incision site. The haptics should be pulled out through the 3 and 9 o'clock incisions. The previously passed sutures are tied to each haptic. (F) The intraocular lens is inserted into the anterior chamber and then into the posterior cavity while gently pulling the sutures at 6 and 12 o'clock.
Reference
-
1. Malbran ES, Malbran E Jr, Negri I. Lens guide suture for transport and fixation in secondary IOL implantation after intracapsular extraction. Int Ophthalmol. 1986; 9:151–160.
Article2. Por YM, Lavin MJ. Techniques of intraocular lens suspension in the absence of capsular/zonular support. Surv Ophthalmol. 2005; 50:429–462.
Article3. Kim DH, Heo JW, Hwang SW, et al. Modified transscleral fixation using combined temporary haptic externalization and injector intraocular lens implantation. J Cataract Refract Surg. 2010; 36:707–711.
Article4. Hayashi K, Hayashi H, Nakao F, Hayashi F. Intraocular lens tilt and decentration, anterior chamber depth, and refractive error after trans-scleral suture fixation surgery. Ophthalmology. 1999; 106:878–882.5. Asadi R, Kheirkhah A. Long-term results of scleral fixation of posterior chamber intraocular lenses in children. Ophthalmology. 2008; 115:67–72.
Article6. McAllister AS, Hirst LW. Visual outcomes and complications of scleral-fixated posterior chamber intraocular lenses. J Cataract Refract Surg. 2011; 37:1263–1269.
Article7. Bergren RL. Four-point fixation technique for sutured posterior chamber intraocular lenses. Arch Ophthalmol. 1994; 112:1485–1487.
Article8. Teichmann KD, Teichmann IA. Haptic design for continuous-loop, scleral fixation of posterior chamber lens. J Cataract Refract Surg. 1998; 24:889.
Article9. Cordoves L, Gomez A, Mesa CG, Abreu JA. Sulcus transscleral sutured posterior chamber lenses. J Cataract Refract Surg. 1999; 25:156–157.10. Chakrabarti A, Gandhi RK, Chakrabarti M. Ab externo 4-point scleral fixation of posterior chamber intraocular lenses. J Cataract Refract Surg. 1999; 25:420–426.11. Azar DT, Wiley WF. Double-knot transscleral suture fixation technique for displaced intraocular lenses. Am J Ophthalmol. 1999; 128:644–646.
Article12. Rao SK, Gopal L, Fogla R, et al. Ab externo 4-point scleral fixation. J Cataract Refract Surg. 2000; 26:9–10.
Article13. Sewelam A. Four-point fixation of posterior chamber intraocular lenses in children with unilateral aphakia. J Cataract Refract Surg. 2003; 29:294–300.
Article14. Lin CP, Tseng HY. Suture fixation technique for posterior chamber intraocular lenses. J Cataract Refract Surg. 2004; 30:1401–1404.
Article15. Fass ON, Herman WK. Sutured intraocular lens placement in aphakic post-vitrectomy eyes via small-incision surgery. J Cataract Refract Surg. 2009; 35:1492–1497.
Article16. Fass ON, Herman WK. Four-point suture scleral fixation of a hydrophilic acrylic IOL in aphakic eyes with insufficient capsule support. J Cataract Refract Surg. 2010; 36:991–996.
Article17. Munoz-Escriva L, Furlan WD. Statistical analysis when dealing with astigmatism: assessment of different spherocylindrical notations. Ophthalmic Epidemiol. 2001; 8:27–37.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- In situ Scleral Suture Fixation of an Injector-delivered Intraocular Lens
- The Effect of Scleral Sutured Intraocular Lens with Optic-haptic Junction Fixation in the Capsular Bag
- Outcomes of Re-fixation after the First Intraocular Lens Scleral Fixation
- Intraocular Lens Scleral Fixation by Flanged Fixation Using 5-0 Polyprophylene
- Scleral Fixation of a Single-Piece AcrySof Toric Intraocular Lens: A Case Report
