Conservative Treatment of Proximal Humeral Fracture
- Affiliations
-
- 1Department of Orthopedic Surgery, Ewha Womans University Mokdong Hospital, Ewha Womans University School of Medicine, Seoul, Korea. sjshin622@ewha.ac.kr
- KMID: 2402712
- DOI: http://doi.org/10.12671/jkfs.2018.31.1.29
Abstract
- A proximal humeral fracture is an osteoporotic fracture that often occurs in elderly women. Approximately 80% of all proximal humeral fractures are non-displaced fractures, which can be treated with conservative treatment to achieve stable union. The treatment plan for fractures involving displaced and comminuted fractures is controversial. Malunion, avascular necrosis of the humeral head, and shoulder stiffness due to conservative treatment can occur but the functional deterioration is low and the patient satisfaction is high. The indications for the conservative management of proximal humeral fractures include a non-displaced fracture and a 2-part fracture, low-functional demanded 3-part fracture, and operative-limited 4-part fracture. Recently, the surgical indications have expanded as technological advances in surgical fixation methods and functional needs of elderly patients are increasing. Current treatment policy decisions tend to be determined by the personal preference and expert opinion rather than by evidence-based decision-making.
MeSH Terms
Figure
-
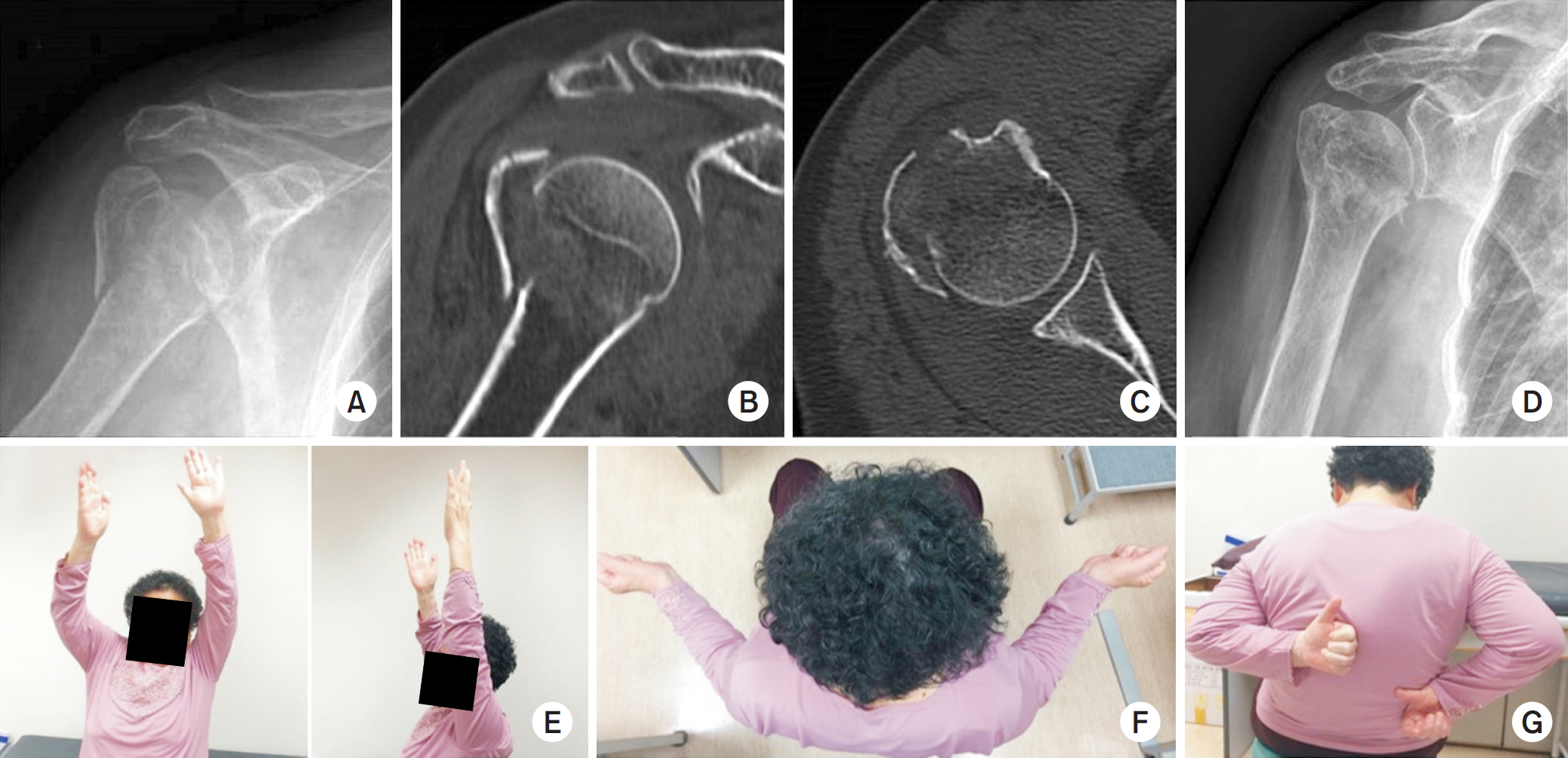
Fig. 1. A 68-year-old woman with a displaced 2-part fracture of the proximal humerus on the right shoulder. After informed consent from the patient, we used a picture of the patient. (A) Initial simple radiograph. (B) Coronal cut of the initial computed tomography (CT) image. (C) Axial cut of the initial CT image. (D) Follow-up at 3 months. The range of motion of the shoulder measured after 3 months of conservative treatment. (E) Forward flexion. (F) External rotation. (G) Internal rotation.
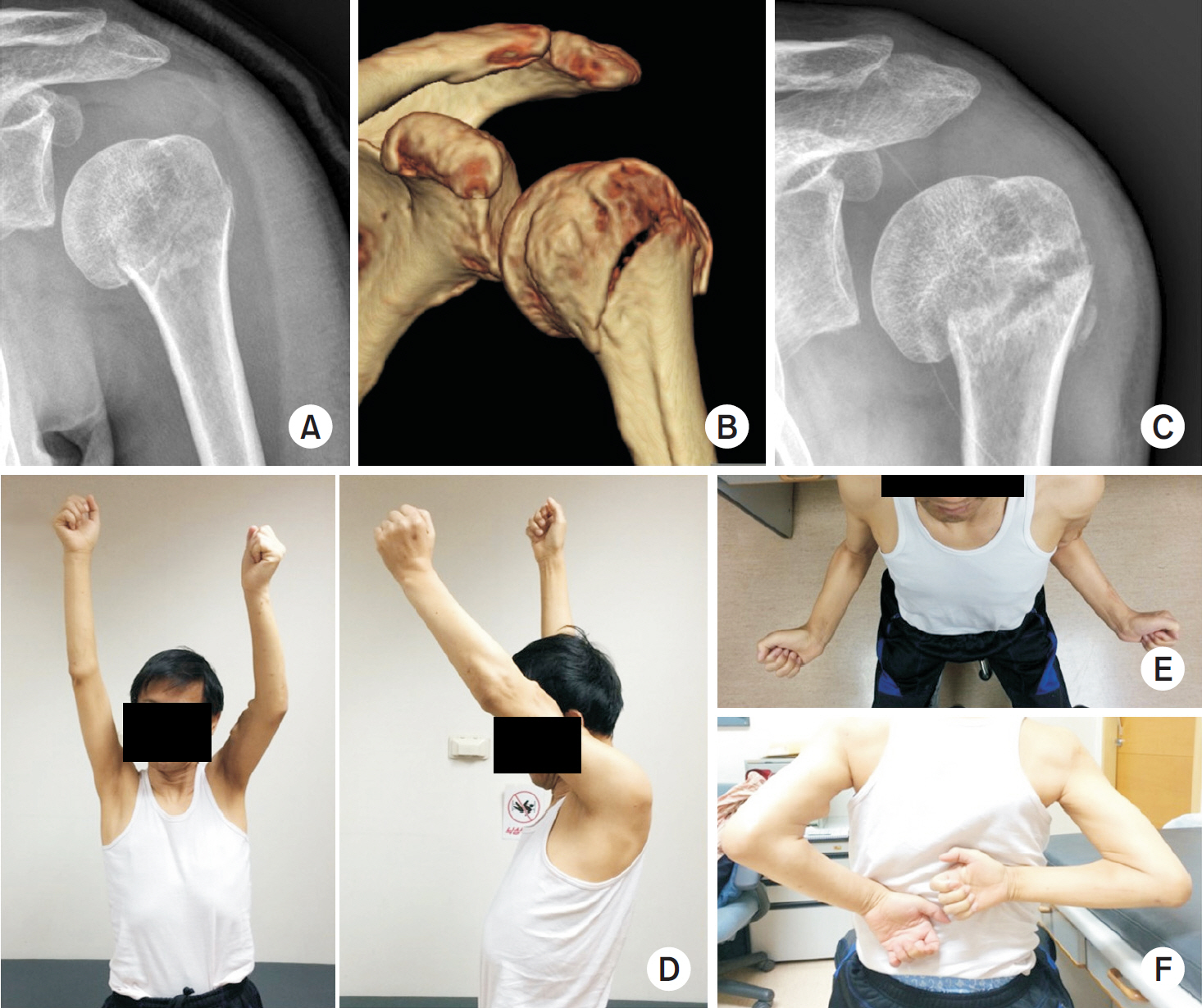
Fig. 2. A 54-year-old man with a 2-part fracture of the proximal humerus on the left shoulder. After informed consent from the patient, we used a picture of the patient. (A) Initial simple radiograph. (B) Three-dimensional reconstruction of initial computed tomography image. (C) Partial union at 15 months after conservative treatment. The range of motion of the shoulder was measured after 15 months of conservative treatment. (D) Forward flexion. (E) External rotation. (F) Internal rotation.
Reference
-
References
1. Horak J, Nilsson BE. Epidemiology of fracture of the upper end of the humerus. Clin Orthop Relat Res. 112:250–253. 1975.
Article2. Giannotti S, Bottai V, Dell'osso G, et al. Indices of risk assessment of fracture of the proximal humerus. Clin Cases Miner Bone Metab. 9:37–39. 2012.3. Zyto K, Ahrengart L, Sperber A, Törnkvist H. Treatment of displaced proximal humeral fractures in elderly patients. J Bone Joint Surg Br. 79:412–417. 1997.
Article4. Neer CS 2nd. Displaced proximal humeral fractures. I. Classification and evaluation. J Bone Joint Surg Am. 52:1077–1089. 1970.
Article5. Misra A, Kapur R, Maffulli N. Complex proximal humeral fractures in adults: a systematic review of management. Injury. 32:363–372. 2001.6. Handoll HH, Gibson JN, Madhok R. Interventions for treating proximal humeral fractures in adults. Cochrane Database Syst Rev. 4:CD000434. 2003.
Article7. Court-Brown CM, Garg A, McQueen MM. The epidemiology of proximal humeral fractures. Acta Orthop Scand. 72:365–371. 2001.
Article8. Lee SH, Dargent-Molina P, Bréart G. EPIDOS Group. Epide-miologie de l'Osteoporose Study: Risk factors for fractures of the proximal humerus: results from the EPIDOS prospective study. J Bone Miner Res. 17:817–825. 2002.9. Saitoh S, Nakatsuchi Y, Latta L, Milne E. Distribution of bone mineral density and bone strength of the proximal humerus. J Shoulder Elbow Surg. 3:234–242. 1994.
Article10. Gerber C, Terrier F, Ganz R. The role of the coracoid process in the chronic impingement syndrome. J Bone Joint Surg Br. 67:703–708. 1985.
Article11. Neer CS 2nd. Impingement lesions. Clin Orthop Relat Res. 173:70–77. 1983.
Article12. Brooks CH, Revell WJ, Heatley FW. Vascularity of the humeral head after proximal humeral fractures. An anatomical cadaver study. J Bone Joint Surg Br. 75:132–136. 1993.
Article13. Meyer C, Alt V, Hassanin H, et al. The arteries of the humeral head and their relevance in fracture treatment. Surg Radiol Anat. 27:232–237. 2005.
Article14. Edelson G, Kelly I, Vigder F, Reis ND. A three-dimensional classification for fractures of the proximal humerus. J Bone Joint Surg Br. 86:413–425. 2004.
Article15. Neer CS 2nd. Four-segment classification of proximal humeral fractures: purpose and reliable use. J Shoulder Elbow Surg. 11:389–400. 2002.
Article16. Marsh JL, Slongo TF, Agel J, et al. Fracture and dislocation classification compendium – 2007: Orthopaedic Trauma Association classification, database and outcomes committee. J Orthop Trauma. 21:S1–S133. 2007.17. Sidor ML, Zuckerman JD, Lyon T, Koval K, Cuomo F, Schoenberg N. The Neer classification system for proximal humeral fractures. An assessment of interobserver reliability and intraobserver reproducibility. J Bone Joint Surg Am. 75:1745–1750. 1993.
Article18. Beznoska J, Sosna A. A modified Desault bandage for fixation of the proximal humerus. Acta Chir Orthop Traumatol Cech. 61:39–41. 1994.19. Koval KJ, Gallagher MA, Marsicano JG, Cuomo F, McShi-nawy A, Zuckerman JD. Functional outcome after minimally displaced fractures of the proximal part of the humerus. J Bone Joint Surg Am. 79:203–207. 1997.
Article20. Hodgson SA, Mawson SJ, Stanley D. Rehabilitation after two-part fractures of the neck of the humerus. J Bone Joint Surg Br. 85:419–422. 2003.
Article21. Rath E, Alkrinawi N, Levy O, Debbi R, Amar E, Atoun E. Minimally displaced fractures of the greater tuberosity: outcome of nonoperative treatment. J Shoulder Elbow Surg. 22:e8–e11. 2013.
Article22. Court-Brown CM, Garg A, McQueen MM. The translated two-part fracture of the proximal humerus. Epidemiology and outcome in the older patient. J Bone Joint Surg Br. 83:799–804. 2001.23. Hauschild O, Konrad G, Audige L, et al. Operative versus nonoperative treatment for two-part surgical neck fractures of the proximal humerus. Arch Orthop Trauma Surg. 133:1385–1393. 2013.
Article24. Rasmussen S, Hvass I, Dalsgaard J, Christensen BS, Holstad E. Displaced proximal humeral fractures: results of conservative treatment. Injury. 23:41–43. 1992.
Article25. Iyengar JJ, Devcic Z, Sproul RC, Feeley BT. Nonoperative treatment of proximal humerus fractures: a systematic review. J Orthop Trauma. 25:612–617. 2011.
Article26. Torrens C, Corrales M, Vilà G, Santana F, Cáceres E. Functional and quality-of-life results of displaced and nondisplaced proximal humeral fractures treated conservatively. J Orthop Trauma. 25:581–587. 2011.
Article27. Fjalestad T, Hole MØ. Displaced proximal humeral fractures: operative versus nonoperative treatment: a 2-year extension of a randomized controlled trial. Eur J Orthop Surg Traumatol. 24:1067–1073. 2014.28. Olerud P, Ahrengart L, Ponzer S, Saving J, Tidermark J. Internal fixation versus nonoperative treatment of displaced 3-part proximal humeral fractures in elderly patients: a randomized controlled trial. J Shoulder Elbow Surg. 20:747–755. 2011.
Article29. den Hartog D, de Haan J, Schep NW, Tuinebreijer WE. Primary shoulder arthroplasty versus conservative treatment for comminuted proximal humeral fractures: a systematic literature review. Open Orthop J. 4:87–92. 2010.
Article30. McLaurin TM. Proximal humerus fractures in the elderly are we operating on too many? Bull Hosp Jt Dis. 62:24–32. 2004.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Comparative study between operative and conservative treatment in 3 part and 4 part fracture of the proximal humerus
- Inter-rater agreement among shoulder surgeons on treatment options for proximal humeral fractures among shoulder surgeons
- Operative Treatment of Fracture of The Proximal Humerus
- A Clinical Study of Proximal Humeral Fractures
- Fracture-separation of the distal humeral epiphysis in children
