Tentorial Dural Arteriovenous Fistulas: A Single-Center Cohort of 12 Patients
- Affiliations
-
- 1Department of Radiology, St. Elisabeth Hospital, Tilburg, The Netherlands. hgjkortman@gmail.com
- 2Department of Neurosurgery, St. Elisabeth Hospital, Tilburg, The Netherlands.
- 3Department of Radiology, Academic Medical Center, Amsterdam, The Netherlands.
- KMID: 2401781
- DOI: http://doi.org/10.7461/jcen.2017.19.4.284
Abstract
OBJECTIVE
Tentorial dural arteriovenous fistulas usually drain into cortical veins and often present with hemorrhage. Treatment goal is occlusion of the draining vein, either by surgery or endovascular techniques. We present the multimodality treatment results of 12 patients with tentorial dural arteriovenous fistulas.
MATERIALS AND METHODS
Between January 2007 and January 2017, 12 consecutive patients with tentorial dural arteriovenous fistulas were treated. There were 11 men and 1 woman with a mean age of 62 years (range 44-85). Clinical presentation was hemorrhage in 8 (67%), pulsatile tinnitus in 2 (17%) and an incidental finding in 2 (17%). The fistula location was at the tentorium cerebelli in 5 (42%), the torcula Herophilii in 4 (33%) and petroclival in 3 (25%).
RESULTS
In 11 patients, arterial embolization with Onyx or PHIL was the primary treatment. Complete obliteration was achieved in one session in 5 (45%) and in 2 sessions in 4 (36%). In 2 patients additional surgery was needed. Primary surgery was performed in 1 patient followed by endovascular coil occlusion via the venous route. One patient with exclusive pial feeders from the posterior inferior cerebellar artery had a clinically silent P3 occlusion during trans arterial embolization. Finally, all 12 fistula were completely occluded, confirmed with angiography after 8-12 weeks. There were no permanent procedural complications.
CONCLUSION
Patients with tentorial dural arteriovenous fistulas were effectively and safely cured with a strategy of endovascular treatment with various techniques and surgery. Surgical and endovascular techniques are complementary in the treatment of these challenging vascular disorders.
MeSH Terms
Figure
-
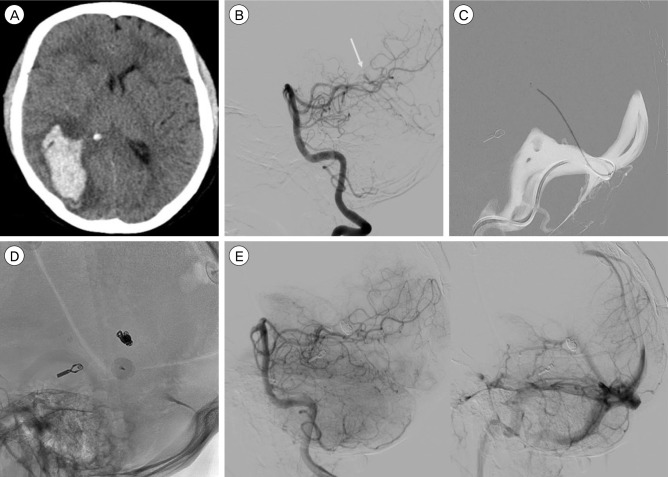
Fig. 1 A 50-year-old male with a right occipital hematoma. (A) Computed tomography scan showing the occipital hematoma. (B) Left vertebral artery angiogram demonstrates a small tentorial dural fistula supplied by the medial dural branch of the superior cerebellar to a deep cortical vein and ultimately draining into the straight sinus. Arrow shows drainage point in the straight sinus. (C) Trans venous navigation via the straight sinus into the draining cortical vein. (D) Lateral radiograph showing the final coil mass in the cortical draining vein close to the straight sinus. (E) Left vertebral angiogram demonstrates obliteration of the fistula with patent straight sinus.
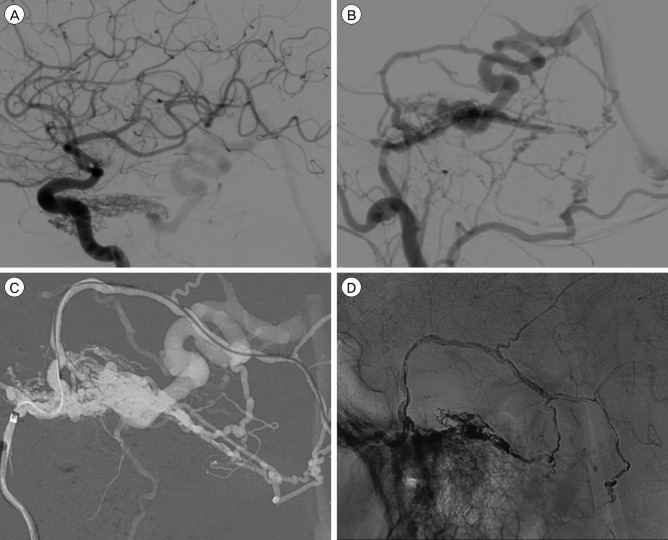
Fig. 2 A 57-year-old male presenting with debilitating tinnitus. (A) Lateral angiogram demonstrating a petroclival tentorial dural arteriovenous fistula with feeders from the inferolateral trunk and meningohypophyseal trunk. (B) Lateral angriogram with external carotid artery injection demonstrating feeders from the middle meningeal artery (MMA) and occipital artery. (C) Digital subtraction image demonstrating distal catheter access via the MMA. (D) Final Onyx (Medtronic) cast demonstrating obliteration of the fistula.

Fig. 3 A 63-year-old male presenting with right cerebellar hemorrhage. (A) Axial computed tomography (CT) scan demonstrating a right cerebellar hemorrhage. (B) CT angiography sagittal reconstruction demonstrating venous ectasia and fistulapoint at the torcula herophilii. (C) Left vertebral injection. Lateral angiogram demonstrating main arterial feeder from the posterior meningeal artery (PM). (D) Left vertebral injection. Arrow demonstrating PM loop where the PM is crossing the tentorial ridge. Distal endovascular access proved impossible because of this loop. Because no other viable arteries were available, the patient went for surgery.
Reference
-
1. Byrne JV, Garcia M. Tentorial dural fistulas: endovascular management and description of the medial dural-tentorial branch of the superior cerebellar artery. AJNR Am J Neuroradiol. 2013; 9. 34(9):1798–1804. PMID: 23660293.
Article2. Cognard C, Gobin YP, Pierot L, Bailly AL, Houdart E, Casasco A, et al. Cerebral dural arteriovenous fistulas: clinical and angiographic correlation with a revised classification of venous drainage. Radiology. 1995; 3. 194:671–680. PMID: 7862961.
Article3. Daniels DJ, Vellimana AK, Zipfel GJ, Lanzino G. Intracranial hemorrhage from dural arteriovenous fistulas: clinical features and outcome. Neurosurg Focus. 2013; 5. 34(5):E15. PMID: 23634919.
Article4. Davies MA, Ter Brugge K, Willinsky R, Wallace MC. The natural history and management of intracranial dural arteriovenous fistulae. Part 2: aggressive lesions. Interv Neuroradiol. 1997; 12. 3(4):303–311. PMID: 20678361.5. Dmytriw AA, Schwartz ML, Cusimano MD, Mendes Pereira V, Krings T, Tymianski M, et al. Gamma Knife radiosurgery for the treatment of intracranial dural arteriovenous fistulas. Interv Neuroradiol. 2017; 4. 23:211–220. PMID: 28156167.
Article6. Gandhi D, Chen J, Pearl M, Huang J, Gemmete JJ, Kathuria S. Intracranial dural arteriovenous fistulas: classification, imaging findings, and treatment. AJNR Am J Neuroradiol. 2012; 6. 33:1007–1013. PMID: 22241393.
Article7. Hiramatsu M, Sugiu K, Hishikawa T, Haruma J, Tokunaga K, Date I, et al. Epidemiology of dural arteriovenous fistula in Japan: Analysis of Japanese Registry of Neuroendovascular Therapy (JR-NET2). Neurol Med Chir (Tokyo). 2014; 1. 54(1):63–71.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Tentorial Dural Arteriovenous Fistula Treated Using Transarterial Onyx Embolization
- Tentorial meningioma encroaching the transverse sinuses and sigmoid sinus junction area associated with dural arteriovenous fistulous malformation: a case report
- Surgical Treatment of Carotid-Cavernous Fistula and Intracranial Dural Arteriovenous Malformations
- Endovascular management of cavernous sinus dural arteriovenous fistulas: Overall review and considerations
- Tentorial Dural Arteriovenous Fistula Presenting With Progressive Encephalomyelopathy
