The Magnetic Resonance (MR) Imaging Features of Myxoid Liposarcoma Arising from the Mesentery: a Case Report
- Affiliations
-
- 1Department of Radiology, Wonkwang University Hospital, Iksan, Korea. yjyh@wku.ac.kr
- 2Imaging Science Research Center, Wonkwang University Hospital, Iksan, Korea.
- KMID: 2400379
- DOI: http://doi.org/10.13104/imri.2017.21.4.252
Abstract
- Primary mesenteric liposarcoma is rare. It is difficult to make an accurate preoperative diagnosis of the myxoid type of liposarcoma by using imaging such as ultrasound or computed tomography (CT) due to the very small amount of fat that is located in the tumor. We report a case of primary myxoid liposarcoma of the mesentery which was difficult to differentiate from other solid mesenteric tumors with a myxoid component such as low grade fibromyxoid sarcoma, myxoid leiomyosarcoma or myxoma. Use of chemical shift magnetic resonance (MR) imaging to detect small fat components and its cystic appearance with solid components on the MR images can be useful to differentiate myxoid liposarcoma from the other mesenteric tumors with a myxoid component.
MeSH Terms
Figure
-
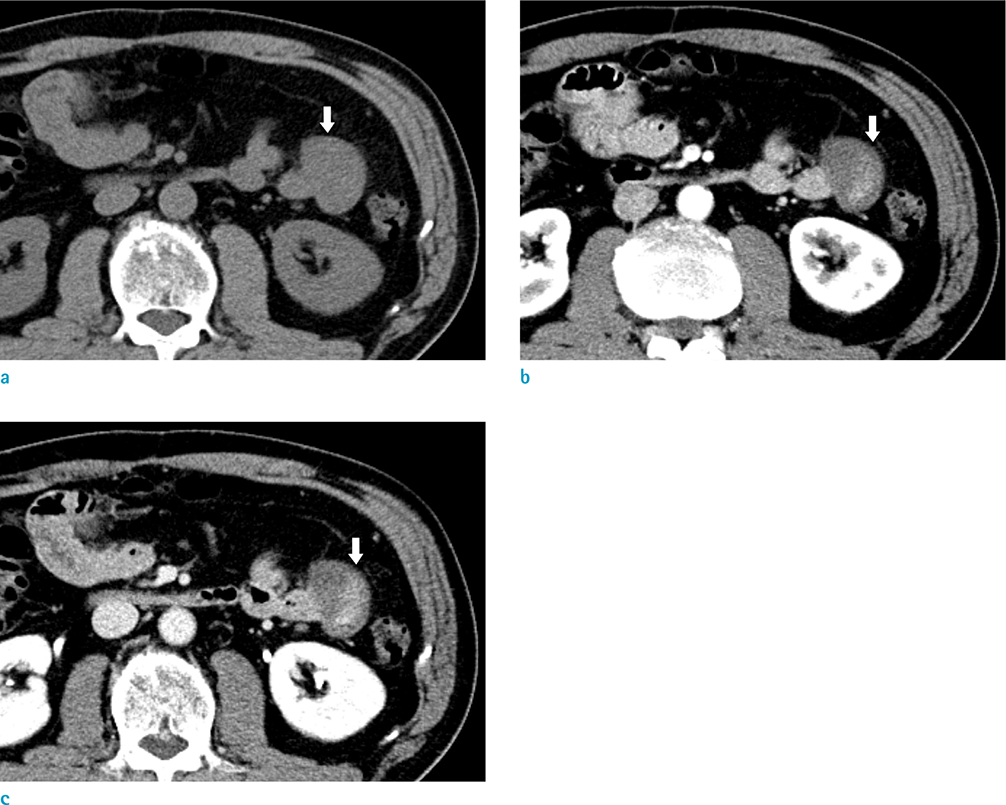
Fig. 1 A 49-year-old man with myxoid liposarcoma arising from the mesentery. An abdominal pre-contrast CT image (a) shows a 5-cm-sized, well defined homogeneous low attenuated mass (arrow) and abutting antimesenteric border of the jejunum. The mass shows heterogeneous enhancement (arrow) on the arterial phase (b) and a persistent enhancement pattern (arrow) on the portal phase (c).

Fig. 2 An abdominal MR image of myxoid liposarcoma arising from the mesentery. The mass exhibits a low signal intensity with multifocal tiny high signal intensity foci (arrows) on the in-phase T1-weighted images (a), which are shown as signal drops (open arrows) on the out-of-phase chemical shift T1-weighted MR images (b) suggesting multifocal small lipid foci in the tumor. Also, multiple lobulated bright cyst-like hyper signal intensity foci (arrows) were present on the T2-weighted images (c). Even though these lesions seem like water, they are not pure cysts since it contains myxoid components. There is no definite grossly fat suppressed lesion on the T2-weighted fat saturation MR images (d). The tumor showed a high signal intensity on the diffusion weighted images (DWI) with a high b-value (800 s/mm2) (e) and a low value on the apparent diffusion coefficient (ADC) map (f), suggesting diffusion restriction. It indicates high cellularity and is correlated with the enhancing portion on the abdominal CT.
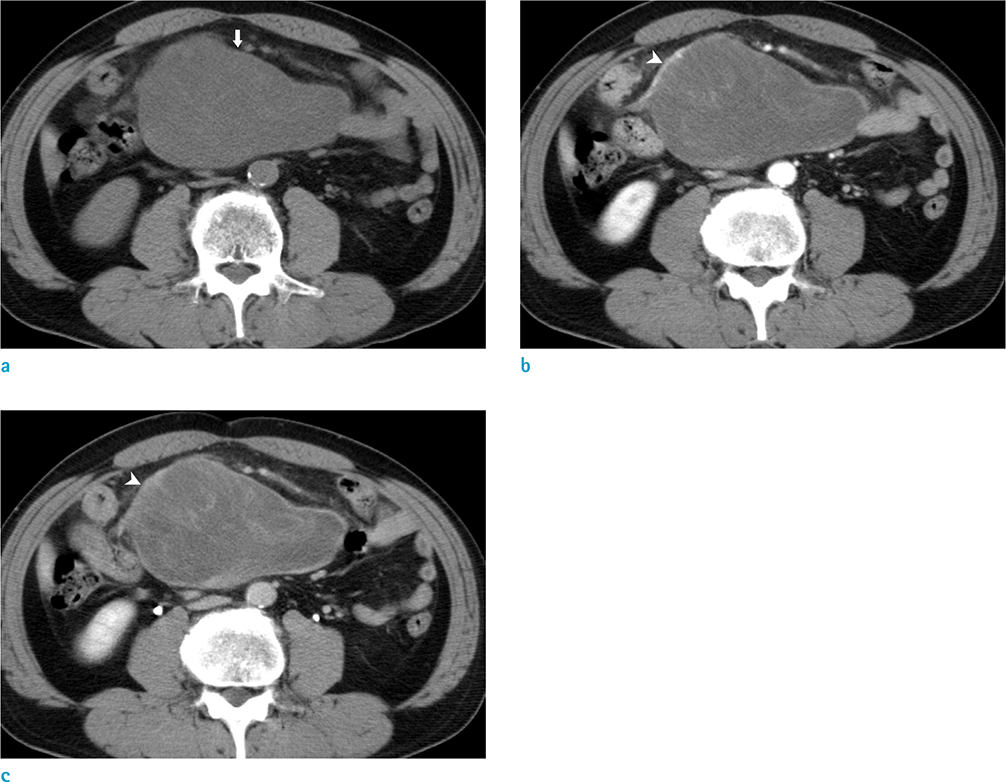
Fig. 3 Preoperative abdominal CT images 2 years ago. On the pre-contrast CT image (a), about a 15-cm-sized welldefined low attenuated mass is located in the mesentery. The tumor shows heterogeneous enhancement (arrow) on the arterial phase (b) and portal venous phase (c). The mesenteric vessels are displaced (arrowheads). When compared with the latest abdominal CT images, it is evident that the previous tumor has less cellularity than that of the recurred tumor.
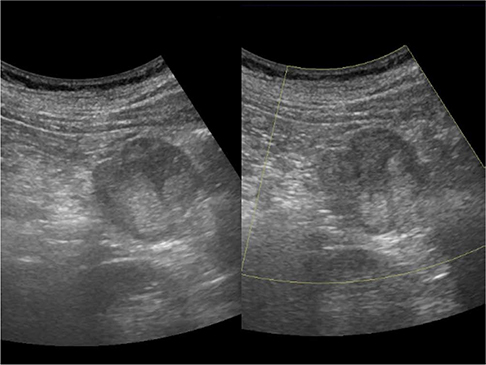
Fig. 4 An abdominal ultrasonography shows about a 5-cm-sized round shaped and heterogeneous echoic mass without internal hypervascularity as evidenced in the color Doppler ultrasonography. Liposarcoma is usually avascular to moderately vascular tumor. Also, there is no evidence of a pure cystic portion in the tumor.

Fig. 5 Photograph of the surgical resection specimen of the myxoid liposarcoma and the microscopic examination of the resected specimen. The specimen (a) shows a round well-defined whitish myxoid mass. It is easily distinguishable by the presence of a normal lipid (arrows), immature lipid components (arrowheads), and myxoid components (open arrows). On the section, the cut surface shows a hemorrhagic lesion at the serosal aspect. These hemorrhagic lesions are correlated with the enhancing aspect on the abdominal CT, which suggests high vascularity. Histopathologic exam (Hematoxylin & Eosin staining, × 200) (b) shows multiple lipoblasts (arrows) and the vessels (arrowhead) are seen in the myxoid spindle cell mesenchymal background.
Reference
-
1. Fletcher CDM, Bridge JA, Hogendoorn P, Mertens F. WHO classification of tumours of soft tissue and bone. 4th ed. Lyon: IARC;2013.2. Jain SK, Mitra A, Kaza RC, Malagi S. Primary mesenteric liposarcoma: an unusual presentation of a rare condition. J Gastrointest Oncol. 2012; 3:147–150.3. Dufay C, Abdelli A, Le Pennec V, Chiche L. Mesenteric tumors: diagnosis and treatment. J Visc Surg. 2012; 149:e239–e251.
Article4. Sung MS, Kang HS, Suh JS, et al. Myxoid liposarcoma: appearance at MR imaging with histologic correlation. Radiographics. 2000; 20:1007–1019.
Article5. Shin NY, Kim MJ, Chung JJ, Chung YE, Choi JY, Park YN. The differential imaging features of fat-containing tumors in the peritoneal cavity and retroperitoneum: the radiologic-pathologic correlation. Korean J Radiol. 2010; 11:333–345.
Article6. Murphey MD, Arcara LK, Fanburg-Smith J. From the archives of the AFIP: imaging of musculoskeletal liposarcoma with radiologic-pathologic correlation. Radiographics. 2005; 25:1371–1395.7. Alatise OI, Oke OA, Olaofe OO, Omoniyi-Esan GO, Adesunkanmi AR. A huge low-grade fibromyxoid sarcoma of small bowel mesentery simulating hyper immune splenomegaly syndrome: a case report and review of literature. Afr Health Sci. 2013; 13:736–740.
Article8. Petscavage-Thomas JM, Walker EA, Logie CI, Clarke LE, Duryea DM, Murphey MD. Soft-tissue myxomatous lesions: review of salient imaging features with pathologic comparison. Radiographics. 2014; 34:964–980.
Article9. Sheth S, Horton KM, Garland MR, Fishman EK. Mesenteric neoplasms: CT appearances of primary and secondary tumors and differential diagnosis. Radiographics. 2003; 23:457–473.
Article10. Ishiguro S, Yamamoto S, Chuman H, Moriya Y. A case of resected huge ileocolonic mesenteric liposarcoma which responded to pre-operative chemotherapy using doxorubicin, cisplatin and ifosfamide. Jpn J Clin Oncol. 2006; 36:735–738.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Liposarcoma Arising in the Mesentery
- Identification of Fat in Myxoid Matrix-Rich Mesenteric Lipoblastoma Using In-Phase and Opposed-Phase MRI: A Case Report
- Myxoid Liposarcoma of Spermatic Cord Misdiagnosed for Hemangioma
- Liposarcoma: MR Findings in the Histologic Subtypes
- Primary Multiple Mesenteric Liposarcoma of the Transverse Mesocolon
