Ann Hepatobiliary Pancreat Surg.
2017 Nov;21(4):194-198. 10.14701/ahbps.2017.21.4.194.
Clinical usefulness of FDG-PET in patients with hepatocellular carcinoma undergoing surgical resection
- Affiliations
-
- 1Division of Hepatobiliary Surgery, Department of Surgery and Liver Transplantation, Chosun University Hospital, Gwangju, Korea. cnk@chosun.ac.kr
- 2Department of Nuclear Medicine, Chosun University Hospital, Gwangju, Korea.
- KMID: 2397798
- DOI: http://doi.org/10.14701/ahbps.2017.21.4.194
Abstract
- BACKGROUNDS/AIMS
Diagnosis and staging of hepatocellular carcinoma (HCC) is critical because of the variety of treatment methods and prognosis. [¹â¸F]fludeoxyglucose-positron emission tomography/computed tomography ([¹â¸F]FDG-PET/CT) has been suggested as a diagnostic modality in HCC. The purpose of this study is to evaluate the accuracy of FDG-PET for staging of HCC after surgical resection and histological confirmation.
METHODS
We retrospectively collected data of 56 patients that underwent FDG-PET before surgical resection for HCC March 2011-May 2017, all of whom were suitable for resection by conventional HCC staging. Results of the maximal standardized uptake value (SUVmax) were compared with histological confirmation.
RESULTS
A larger tumor size was related with higher SUVmax (≥4.9). The serum alpha-feto protein was associated with SUVmax. Recurrence rate was higher in patients with higher SUVmax and patients with lower SUVmax had a better survival rate.
CONCLUSIONS
The SUVmax correlates well with tumor size and factors associated with biological behavior of HCC such as alpha-feto protein, and it could be a beneficial modality in providing prognostic information for HCC.
Keyword
MeSH Terms
Figure
-
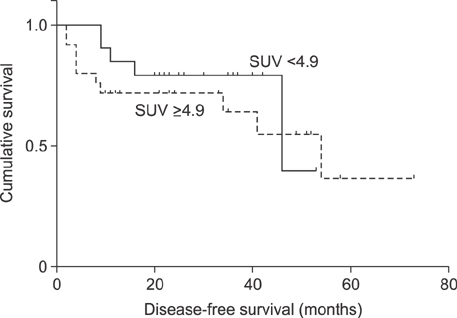
Fig. 1 Disease-free survival rate in group of standard uptake value (SUV)≥4.9 and SUV<4.9.

Fig. 2 Over-all survival rate in in group of standard uptake value (SUV)≥4.9 and SUV<4.9.
Reference
-
1. Yang JD, Roberts LR. Hepatocellular carcinoma: a global view. Nat Rev Gastroenterol Hepatol. 2010; 7:448–458.2. Trojan J, Schroeder O, Raedle J, Baum RP, Herrmann G, Jacobi V, et al. Fluorine-18 FDG positron emission tomography for imaging of hepatocellular carcinoma. Am J Gastroenterol. 1999; 94:3314–3319.3. Cho E, Jun CH, Kim BS, Son DJ, Choi WS, Choi SK. 18F-FDG PET CT as a prognostic factor in hepatocellular carcinoma. Turk J Gastroenterol. 2015; 26:344–350.4. Asman Y, Evenson AR, Even-Sapir E, Shibolet O. [18F]fludeoxyglucose positron emission tomography and computed tomography as a prognostic tool before liver transplantation, resection, and loco-ablative therapies for hepatocellular carcinoma. Liver Transpl. 2015; 21:572–580.5. Kim MJ, Kim YS, Cho YH, Jang HY, Song JY, Lee SH, et al. Use of 18F-FDG PET to predict tumor progression and survival in patients with intermediate hepatocellular carcinoma treated by transarterial chemoembolization. Korean J Intern Med. 2015; 30:308–315.6. Murakami K. FDG-PET for hepatobiliary and pancreatic cancer: Advances and current limitations. World J Clin Oncol. 2011; 2:229–236.7. Seo S, Hatano E, Higashi T, Hara T, Tada M, Tamaki N, et al. Fluorine-18 fluorodeoxyglucose positron emission tomography predicts tumor differentiation, P-glycoprotein expression, and outcome after resection in hepatocellular carcinoma. Clin Cancer Res. 2007; 13:427–433.8. Moon CM, Bang S, Chung JB, Park SW, Song SY, Yun M, et al. Usefulness of 18F-fluorodeoxyglucose positron emission tomography in differential diagnosis and staging of cholangiocarcinomas. J Gastroenterol Hepatol. 2008; 23:759–765.9. Bar-Shalom R, Yefremov N, Guralnik L, Gaitini D, Frenkel A, Kuten A, et al. Clinical performance of PET/CT in evaluation of cancer: additional value for diagnostic imaging and patient management. J Nucl Med. 2003; 44:1200–1209.10. Wang XY, Chen D, Zhang XS, Chen ZF, Hu AB. Value of 18F-FDG-PET/CT in the detection of recurrent hepatocellular carcinoma after hepatectomy or radiofrequency ablation: a comparative study with contrast-enhanced ultrasound. J Dig Dis. 2013; 14:433–438.11. Khan MA, Combs CS, Brunt EM, Lowe VJ, Wolverson MK, Solomon H, et al. Positron emission tomography scanning in the evaluation of hepatocellular carcinoma. J Hepatol. 2000; 32:792–797.12. Abuodeh Y, Naghavi AO, Ahmed KA, Venkat PS, Kim Y, Kis B, et al. Prognostic value of pre-treatment F-18-FDG PET-CT in patients with hepatocellular carcinoma undergoing radioembolization. World J Gastroenterol. 2016; 22:10406–10414.13. Lin CY, Liao CW, Chu LY, Yen KY, Jeng LB, Hsu CN, et al. Predictive value of 18F-FDG PET/CT for vascular invasion in patients with hepatocellular carcinoma before liver transplantation. Clin Nucl Med. 2017; 42:e183–e187.14. Yang SH, Suh KS, Lee HW, Cho EH, Cho JY, Cho YB, et al. The role of (18)F-FDG-PET imaging for the selection of liver transplantation candidates among hepatocellular carcinoma patients. Liver Transpl. 2006; 12:1655–1660.15. Boussouar S, Itti E, Lin SJ, Decaens T, Evangelista E, Chiaradia M, et al. Functional imaging of hepatocellular carcinoma using diffusion-weighted MRI and (18)F-FDG PET/CT in patients on waiting-list for liver transplantation. Cancer Imaging. 2016; 16:4.16. Tsai TJ, Chau GY, Lui WY, Tsay SH, King KL, Loong CC, et al. Clinical significance of microscopic tumor venous invasion in patients with resectable hepatocellular carcinoma. Surgery. 2000; 127:603–608.17. Vauthey JN, Lauwers GY, Esnaola NF, Do KA, Belghiti J, Mirza N, et al. Simplified staging for hepatocellular carcinoma. J Clin Oncol. 2002; 20:1527–1536.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Hepatocellular Carcinoma with Right Atrial Invasion Detected by PET/CT
- A Case of Thyroid Cancer Detected with Pet Scan
- Bilateral Ovarian Metastases of Hepatocellular Carcinoma Diagnosed with 18F‑Fluorocholine PET/CT in a Patient with Endometriosis
- Usefulness of 18 F-FDG PET/CT and Multiphase CT in the Differential Diagnosis of Hepatocellular Carcinoma and Combined Hepatocellular CarcinomaCholangiocarcinoma
- F-18 FDG PET Images of the Cervix at Various Time Points after the Loop Electrosurgical Excision Procedure
