Ann Dermatol.
2017 Apr;29(2):210-214. 10.5021/ad.2017.29.2.210.
Transoral Cross-Lip (Abbé-Estlander) Flap as a Viable and Effective Reconstructive Option in Middle Lower Lip Defect Reconstruction
- Affiliations
-
- 1Department of Dermatology, Uijeongbu St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Uijeongbu, Korea. frankyu123@hotmail.com
- KMID: 2394846
- DOI: http://doi.org/10.5021/ad.2017.29.2.210
Abstract
- The Abbé-Estlander flap surgery is a cross-lip procedure that is valuable in repairing a defect on the lower lip using a full-thickness flap, consisting of the skin, muscle and mucosa, from the upper lip. As usefulness and practicality of the flap in reconstruction of lower lip surgical defects in Asian ethnicity have not been documented, the authors present a case of successful lower lip reconstruction with a staged, Abbé-Estlander lip switching flap with commissuroplasty as an illustrative example. A 71-year-old male has presented with an ulcerating lip nodule in the middle one third of the lower lip, measuring about 1.5×2 cm across its long and short axes. Wide excision of the tumor was followed by delineation of the triangular Abbé-Estlander flap from the upper lip, in which the medial hinge point of the base was chosen as the pedicle. Then, the flap elevation was carried out from the lateral commissure and then was transferred into the lower lip defect. Three weeks later, commissuroplasty was performed to correct the rounding at the new commissure. The patient is currently performing his daily activities with no apparent compromise in orbicularis oris strength or oral continence. Given the size of the primary defect and the flap-to-defect ratio of size, the degree of microstomia was acceptable. Even with other myriad of reconstructive options at surgeons' disposal, the Abbé-Estlander lip-switching flap is a reliable, and less morbid method of lower lip reconstruction for Asian surgical candidates. The authors illustrate an exemplary case in which a relatively large lower lip defect was successfully repaired using an upper lip flap of a significantly smaller size in an Asian subject of advanced age, without any remarkable long term sequelae which have traditionally been associated with the trans-oral lip switching flap technique.
Keyword
MeSH Terms
Figure
-
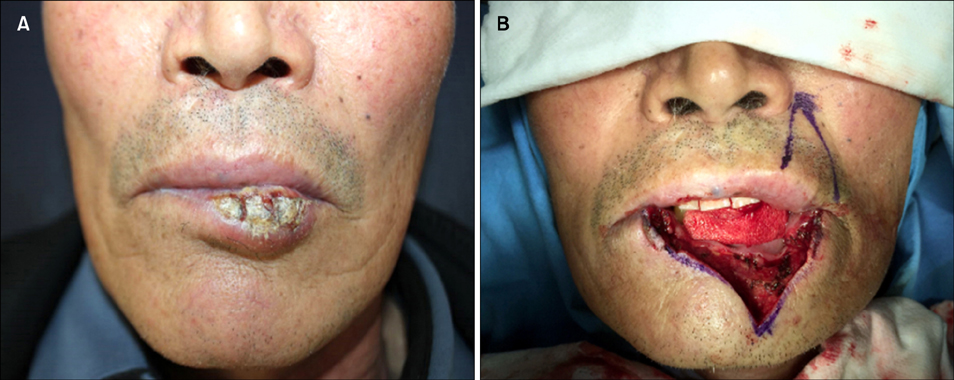
Fig. 1 (A) Clinical photograph of the lesion with extensive involvement of the mid-to-left portion of the lower lip. (B) Wide wedge excision of the primary tumor is followed by design of the flap.

Fig. 2 (A) At completion of the first stage operation and (B) 8 weeks postoperative.
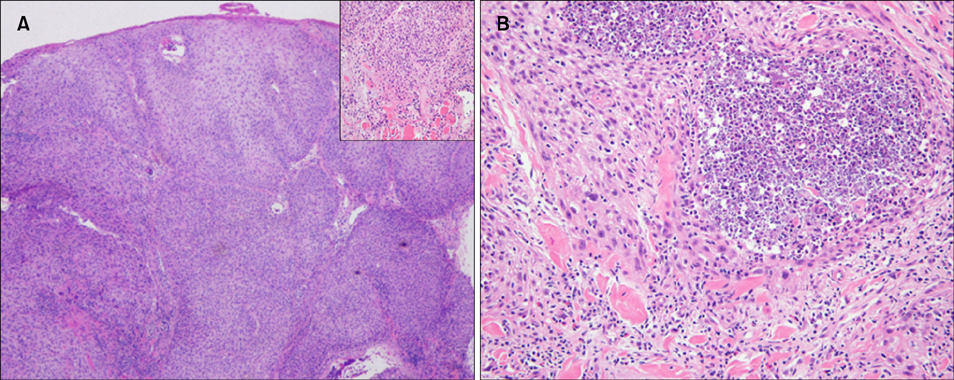
Fig. 3 Histopathological findings of the excised tumor at (A) low magnification (H&E, ×40) shows poorly-differentiated squamous cell carcinoma showing diffuse invasion. Superficial portion of the underlying skeletal muscle is also involved (inset: ×200). Nuclear pleomorphism and intratumoral nercrosis are evident in (B); H&E, ×200.
Reference
-
1. Singh AK, Kar IB, Mishra N, Raut S. Karapandzic flap in reconstruction of post-traumatic lower lip defects: report of two cases. J Maxillofac Oral Surg. 2015; 14:858–861.
Article2. Shin HS, Moon SE, Cho KH, Huh CH. Size-reductive neoadjuvant immunotherapy using imiquimod in squamous cell carcinoma of the lower lip. Ann Dermatol. 2007; 19:75–80.
Article3. Ghassemi A, Prescher A, Riediger D, Axer H. Anatomy of the SMAS revisited. Aesthetic Plast Surg. 2003; 27:258–264.
Article4. Rong L, Lan SJ, Zhang D, Wang WS, Liu C, Peng WH. Reconstruction of the lower vermilion with a musculomucosal flap from the upper lip in the repair of extensive lower lip and chin defects. J Craniofac Surg. 2014; 25:1855–1858.
Article5. Mazzola RF, Lupo G. Evolving concepts in lip reconstruction. Clin Plast Surg. 1984; 11:583–617.
Article6. McGregor IA. Reconstruction of the lower lip. Br J Plast Surg. 1983; 36:40–47.
Article7. Degala S, Shetty SK, Monalisha . The karapandzic flap in lower lip reconstruction. J Maxillofac Oral Surg. 2015; 14:Suppl 1. 421–425.
Article8. Williams EF 3rd, Setzen G, Mulvaney MJ. Modified Bernard-Burow cheek advancement and cross-lip flap for total lip reconstruction. Arch Otolaryngol Head Neck Surg. 1996; 122:1253–1258.
Article9. Mellette JR Jr, Harrington AC. Applications of the crescentic advancement flap. J Dermatol Surg Oncol. 1991; 17:447–454.
Article10. Constantinidis J, Federspil P, Iro H. Functional and aesthetic objectives in the reconstruction of lip defects. Facial Plast Surg. 1999; 15:337–349.
Article11. Wilson JS, Walker EP. Reconstruction of the lower lip. Head Neck Surg. 1981; 4:29–44.
Article12. Czerninski R, Zini A, Sgan-Cohen HD. Lip cancer: incidence, trends, histology and survival: 1970-2006. Br J Dermatol. 2010; 162:1103–1109.
Article13. Eski M, Aykan A, Alhan D, Zor F, Isik S. Evaluation of the results of simultaneous open rhinoplasty and Abbe flap for the reconstruction of the secondary bilateral cleft and nasal deformity. J Plast Reconstr Aesthet Surg. 2015; 68:751–757.
Article14. Smith JW. The anatomical and physiologic acclimatization of tissue transplanted by the lip switch technique. Plast Reconstr Surg Transplant Bull. 1960; 26:40–56.
Article15. Thompson N, Pollard AC. Motor function in Abbe flaps. A histochemical study of motor reinnervation in transplanted muscle tissue of the lips in man. Br J Plast Surg. 1961; 14:66–75.16. Rea JL, Davis WE, Rittenhouse LK. Reinnervation of an Abbe-Estlander and a Gillies fan flap of the lower lip: electromyographic comparison. Arch Otolaryngol. 1978; 104:294–295.
Article17. Zhai QK, Tan XX, Jin ZL, Wang XK, Sun CF. Reconstruction for defects of the lower lip after tumor ablation. J Craniofac Surg. 2012; 23:552–555.
Article18. Kumar A, Shetty PM, Bhambar RS, Gattumeedhi SR, Kumar RM, Kumar H. Versatility of abbe-estlander flap in lip reconstruction-a prospective clinical study. J Clin Diagn Res. 2014; 8:NC18–NC121.19. Roldán JC, Teschke M, Fritzer E, Dunsche A, Härle F, Wiltfang J, et al. Reconstruction of the lower lip: rationale to preserve the aesthetic units of the face. Plast Reconstr Surg. 2007; 120:1231–1239.
Article20. Sun G, Lu M, Hu Q. Reconstruction of extensive lip and perioral defects after tumor excision. J Craniofac Surg. 2013; 24:360–362.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Extended Estlander flap for repairing a large upper lip defect involving the oral commissure
- Reconstruction of lower lip defect using the Abbe-Estlander flap: A case report
- A Case of Three Triangular Flaps as a Secondary Operative Procedure after Reconstruction of the Lower Lip by Estlander's Method
- Reconstruction of a large lower lip defect using a combination of Abbe and staircase flaps: a case report
- Modified Abbé flap for reconstruction of Cupid’s bow and vermilion tubercle in secondary cleft lip deformity
