Easy Way Out-Quick Interpretation of Musculoskeletal Radiographs: The Lower Extremity
- Affiliations
-
- 1Department of Radiology, Research Institute of Radiological Science, Medical Convergence Research Institute, and Severance Biomedical Science Institute, Yonsei University College of Medicine, Seoul, Korea. radiologie@gmail.com
- 2Department of Radiology, Inje University College of Medicine, Haeundae Paik Hospital, Busan, Korea.
- KMID: 2394041
- DOI: http://doi.org/10.3348/jksr.2017.77.5.263
Abstract
- Radiograph remains an important diagnostic tool for detection of musculoskeletal diseases despite recent advances in computed tomography (CT) or magnetic resonance imaging (MRI). Many musculoskeletal disorders are primarily diagnosed by identifying characteristic features on radiographs, which are known to have diagnostic value. In addition, radiographs provide basic information for determining the necessity of cross-sectional imaging such as CT or MRI. Therefore, radiologists should be aware of the radiographic findings of musculoskeletal diseases and they should apply them to establish the diagnosis. This article presents a review of the important radiographic findings that enable the diagnosis of musculoskeletal diseases of the lower extremity.
MeSH Terms
Figure
-
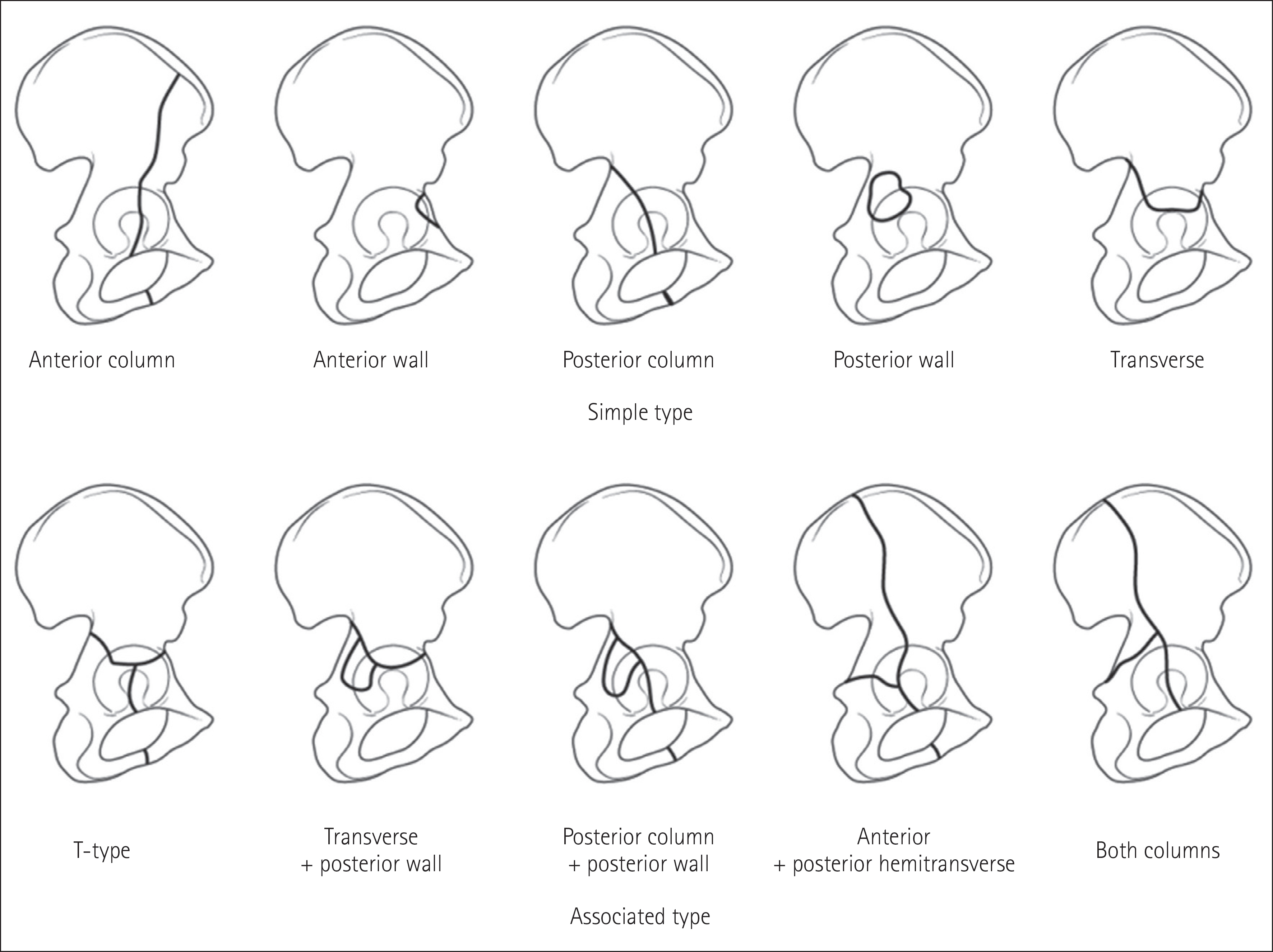
Fig. 1. Letournel classification for acetabular fractures.
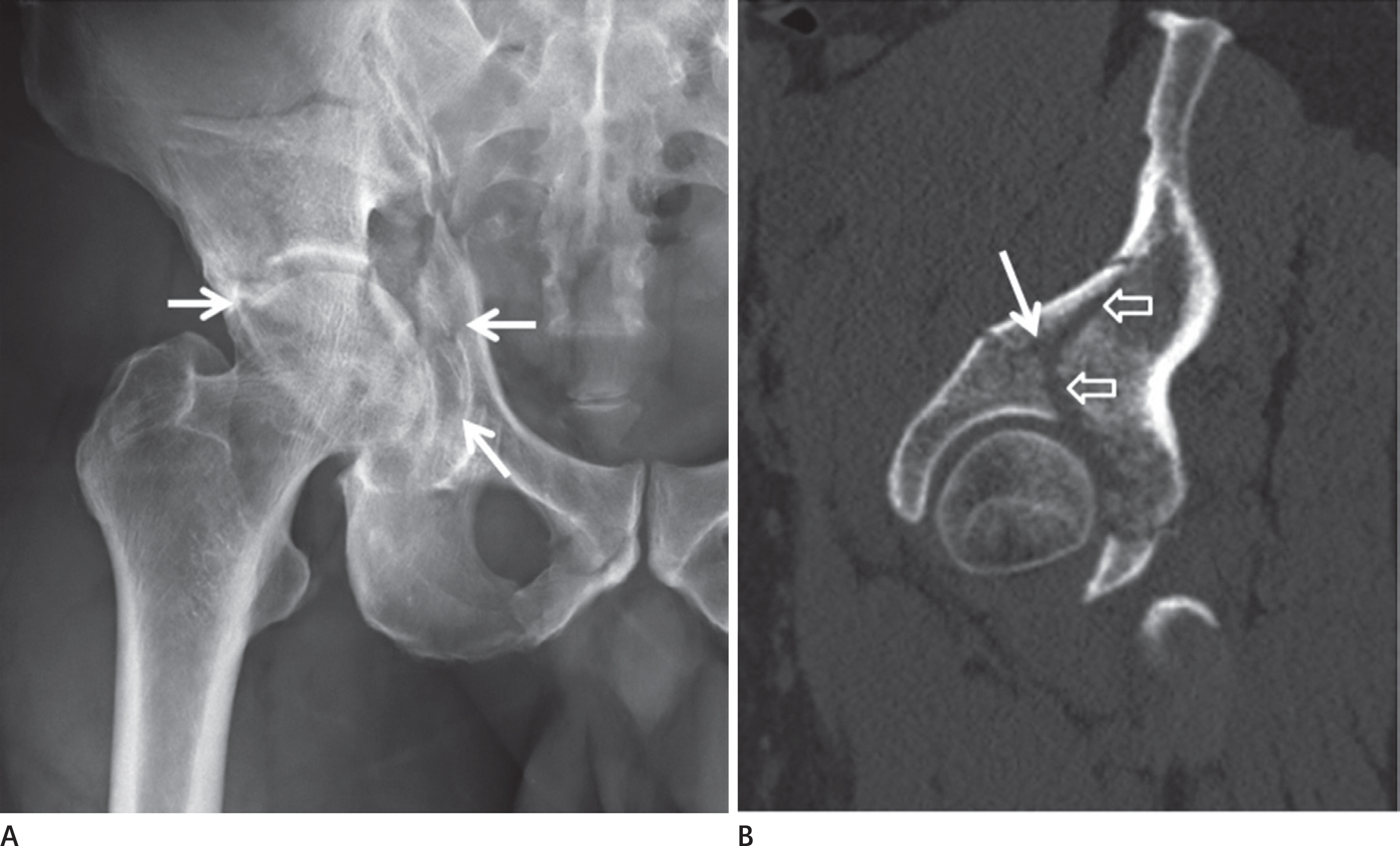
Fig. 2. Acetabular fracture: both column fracture of the associated type. Both column fracture of the right acetabulum is seen on (A) anteropos-terior radiograph and (B) CT sagittal reformation image (arrows). On CT sagittal reformation image, fracture lines extending into the ischium (ar-row) and ilium (hollow arrows) are seen. CT = computed tomography
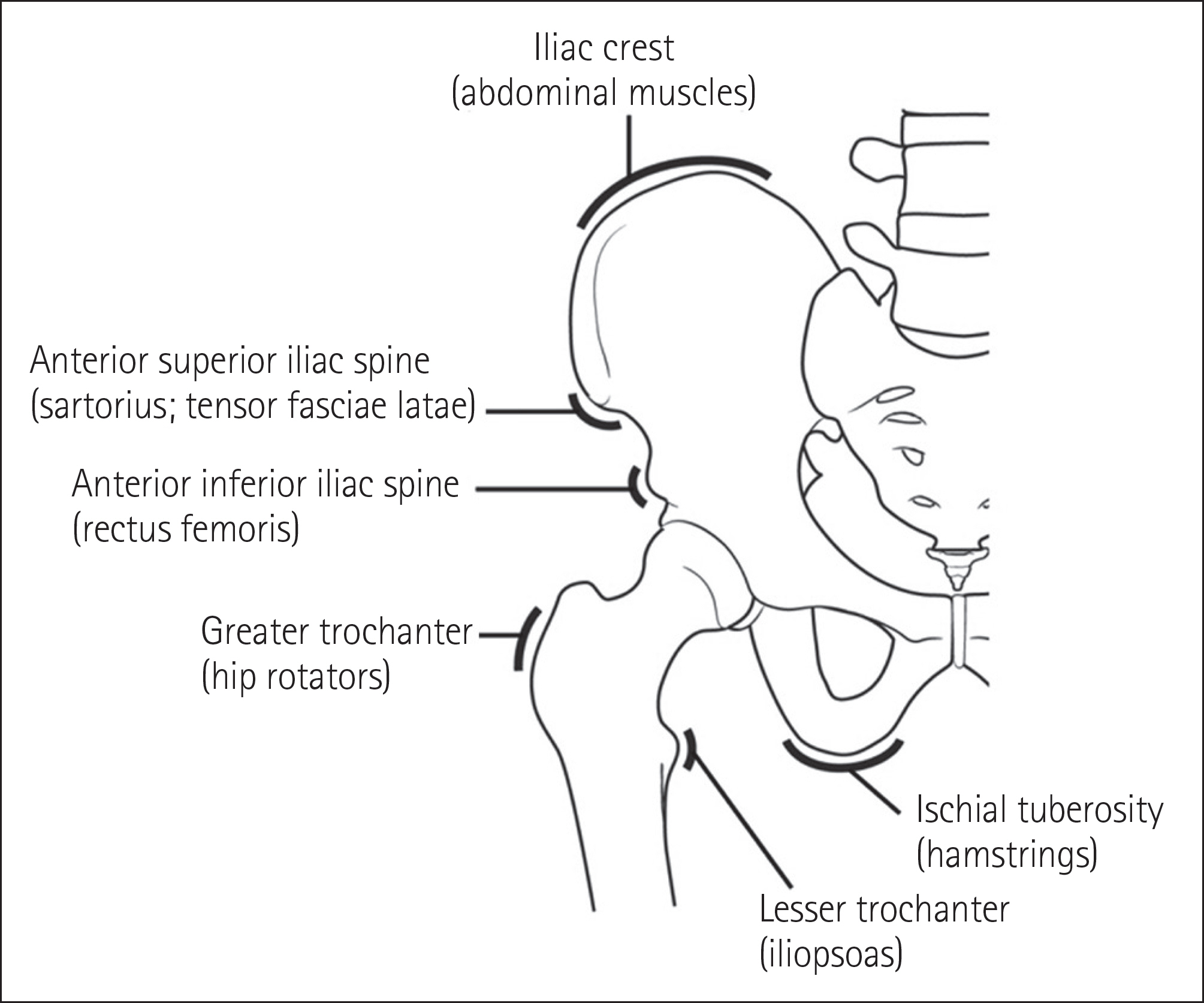
Fig. 3. The type of pelvic avulsion fracture.
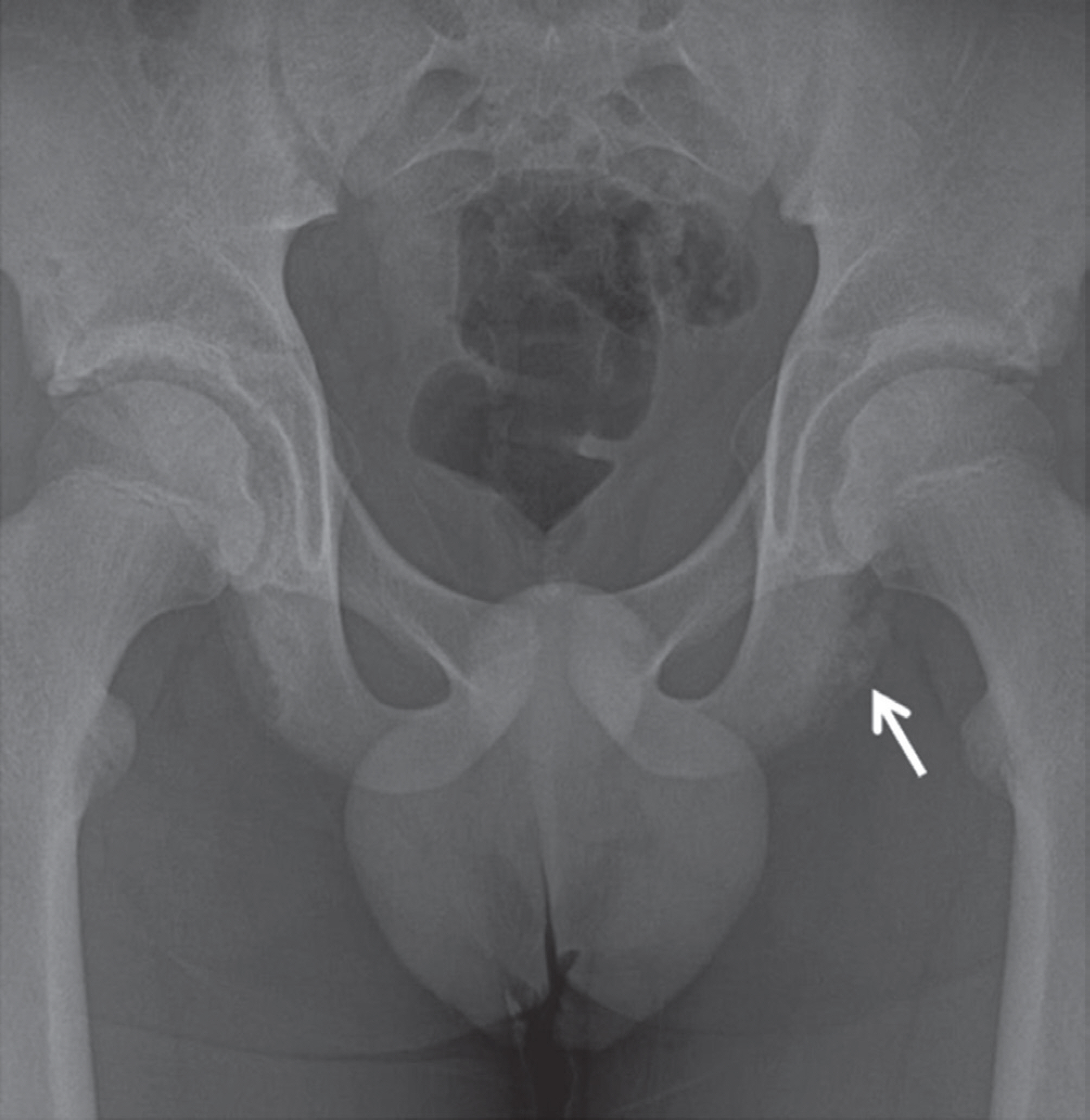
Fig. 4. Avulsion fracture of the ischial tuberosity. There is an avulsion fracture of the left ischial tuberosity (arrow) on which the left hamstring muscle originates.
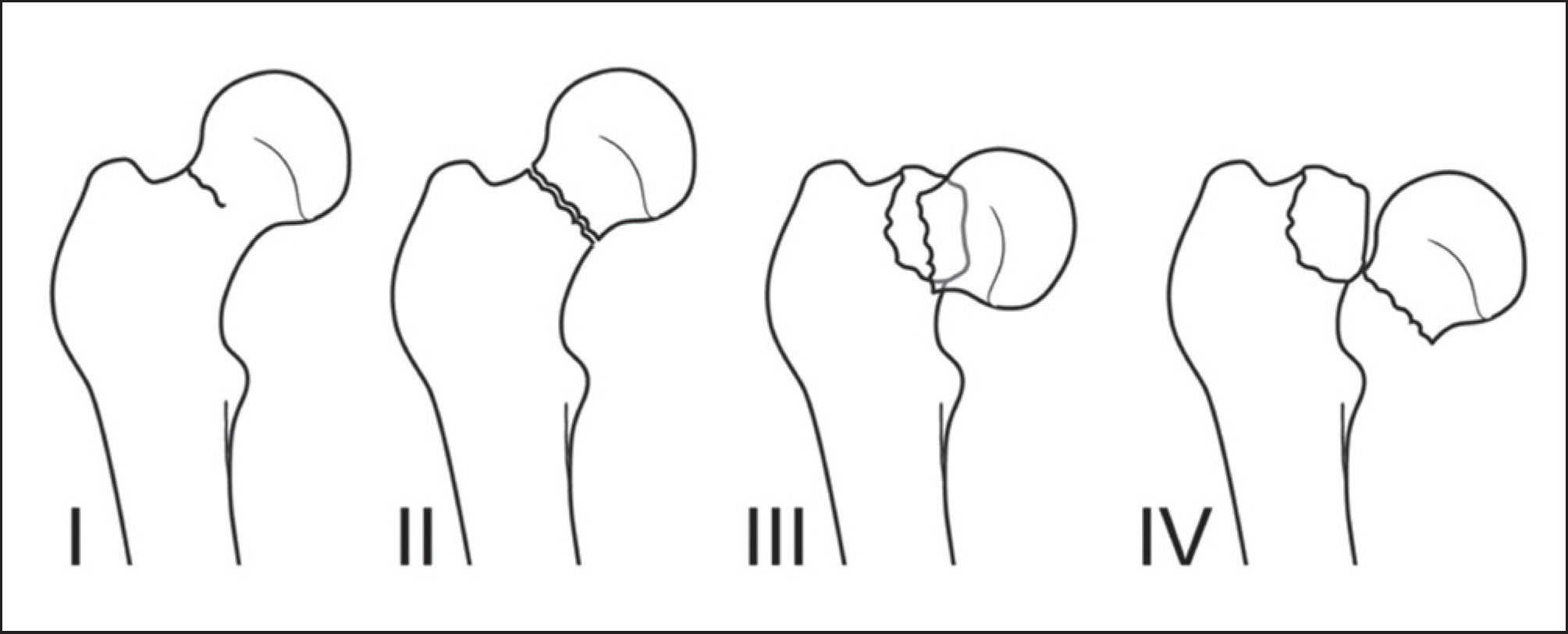
Fig. 5. Garden classification of femoral neck fractures.
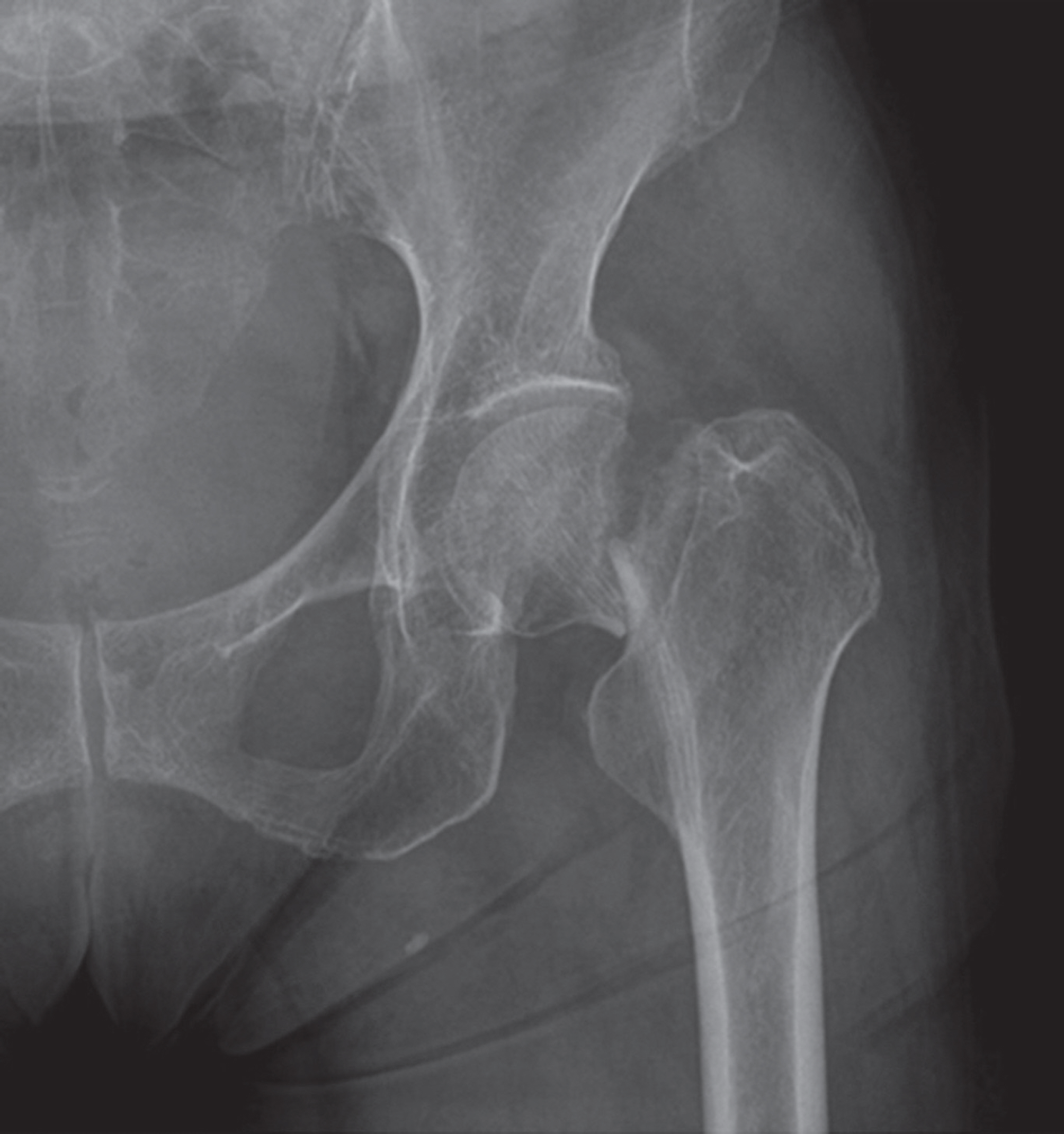
Fig. 6. Femoral neck fracture, Garden stage IV. There is a completely dis-placed fracture of the left femoral neck on the anteroposterior radiograph.

Fig. 7. Bisphosphonate-related fracture. A. There is focal thickening of the lateral cortex of the right proximal femur (arrow) on the AP radiograph. B. After three months, a transverse fracture is seen on the AP radiograph. AP = anteroposterior
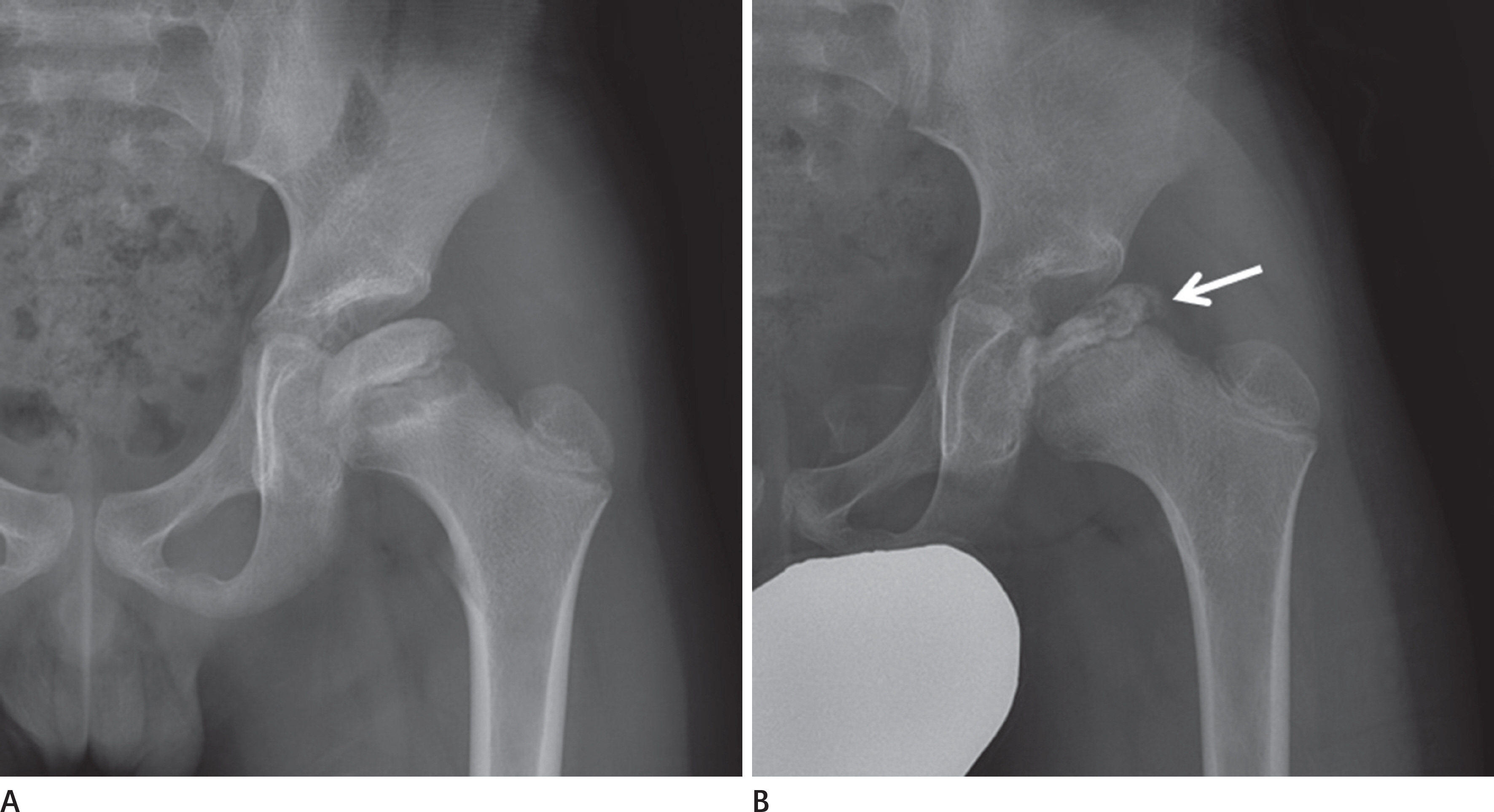
Fig. 8. Legg-Calvé-Perthes disease. A. Sclerosis of the proximal epiphysis of the left femur is seen on the AP radiograph. B. Fragmentation and flattening of the proximal epiphysis of the left femur (arrow) are seen on the nine-month follow-up AP radiograph. AP = anteroposterior
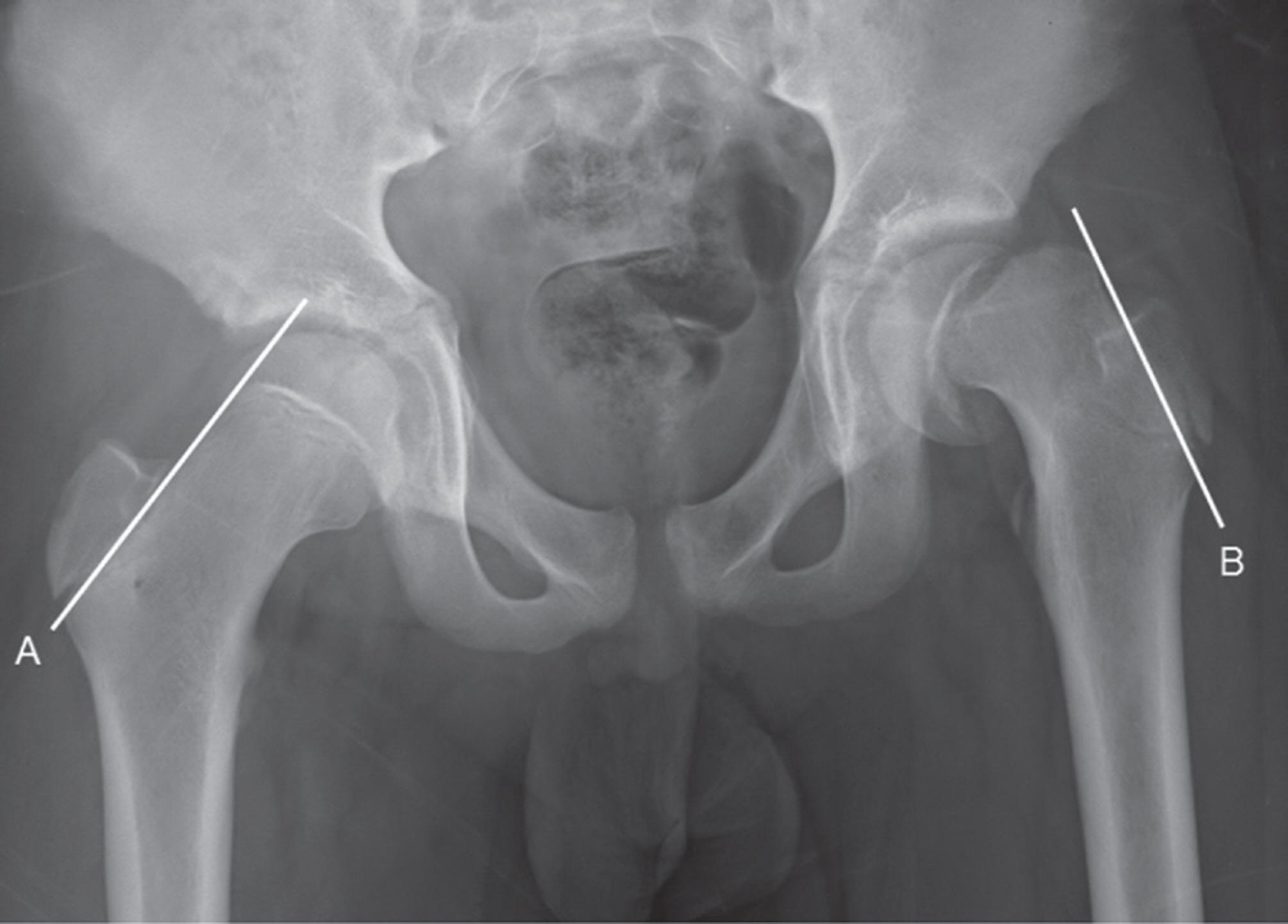
Fig. 9. Slipped capital femoral epiphysis. The left femoral head is dis-placed medially compared to the right femoral head. The growth plate of the left femur is also widened compared to that of the right femur. The right Klein line (A) intersects the right femoral head; however, the left Klein line (B) does not intersect the left femoral head.
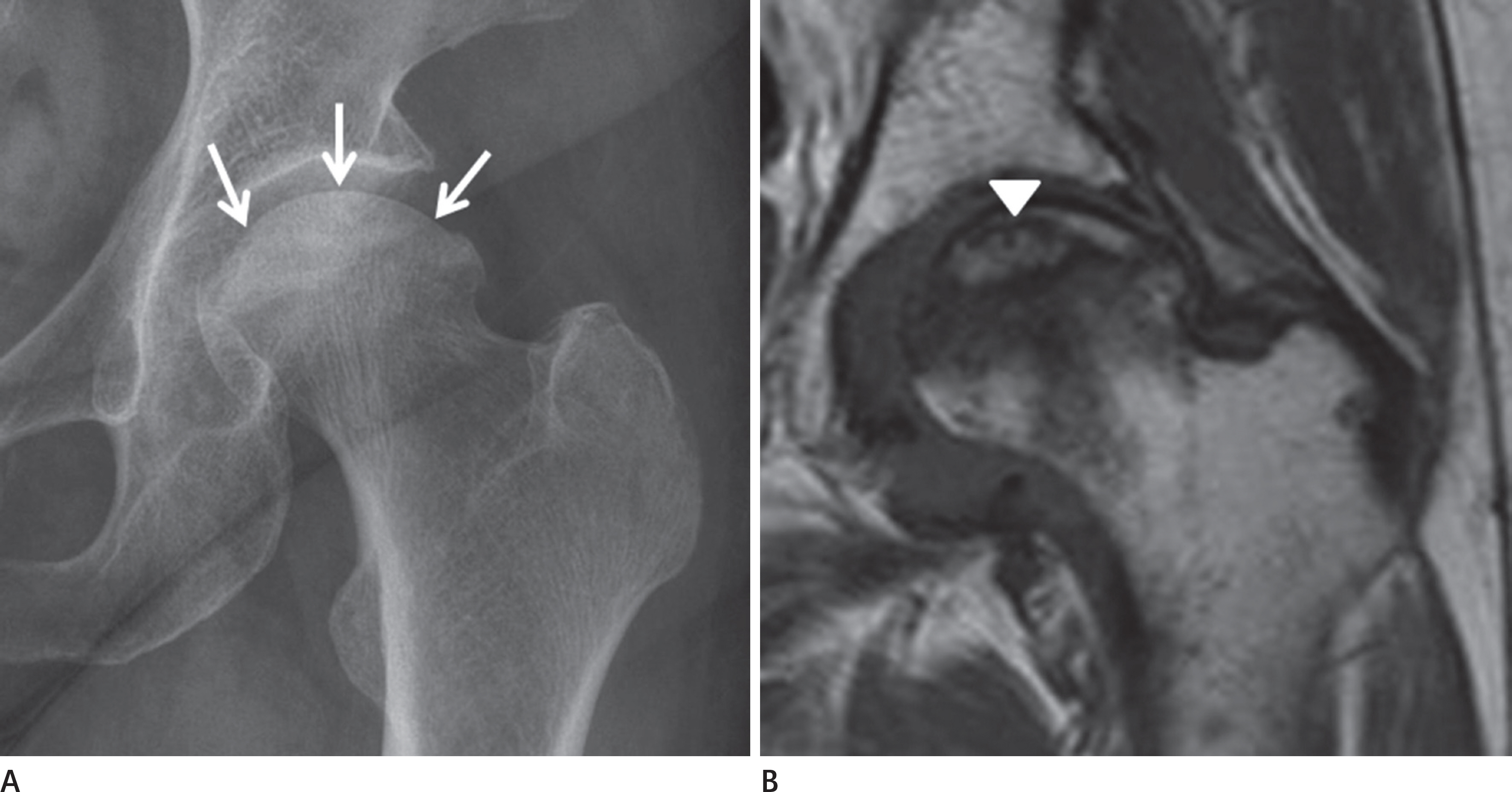
Fig. 10. Femoral head avascular necrosis, stage III. A. The shape of the left femoral head is different from normal sphericity and the superior articular surface is flattened (arrows). B. Flattening of the femoral head and low signal intensity caused by bone marrow edema are observed on T1-weighted coronal magnetic reso-nance image. There is a subchondral fracture on the superior aspect of the femoral head (arrowhead).
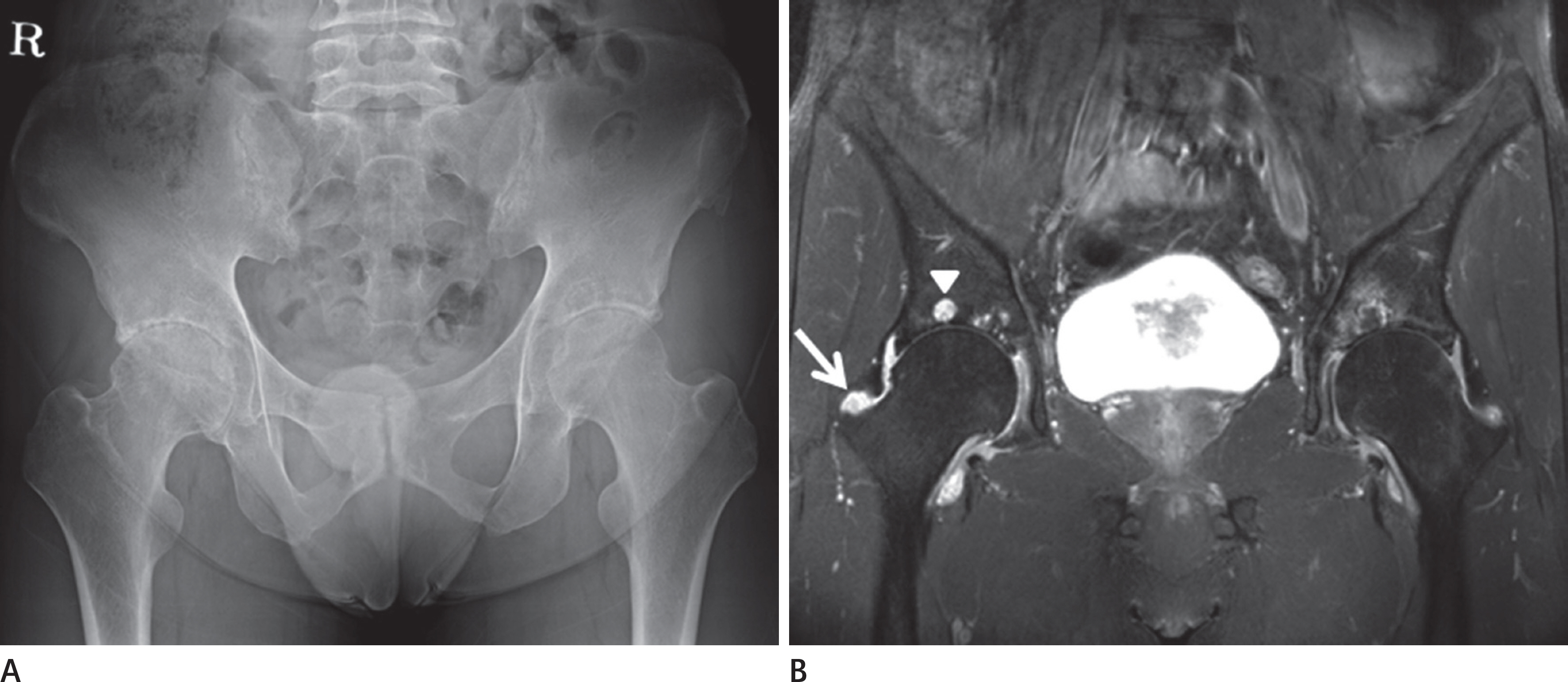
Fig. 11. Rheumatoid arthritis of the hip joint. A. Symmetric joint space narrowing of bilateral hip joints in the axial direction is seen on the anteroposterior radiograph. B. Symmetric joint space narrowing of bilateral hip joints in the axial direction is also seen on fat-suppressed T2-weighted coronal magnetic reso-nance image. Synovial proliferation (arrow) and a subchondral cyst (arrowhead) in the acetabulum of the right hip joint are noted.

Fig. 12. Distal femur fracture, AO/OTA classification, type C3. There is a complex fracture with displacement (arrows) involving the medial con-dyle, the lateral condyle, and the intercondylar area on (A) anteroposterior and (B) lateral radiographs. An abnormal opacity is seen in the soft tissue area on the lateral aspect of the lateral condyle (arrowheads).

Fig. 13. Schatzker classification of tibial plateau fractures.
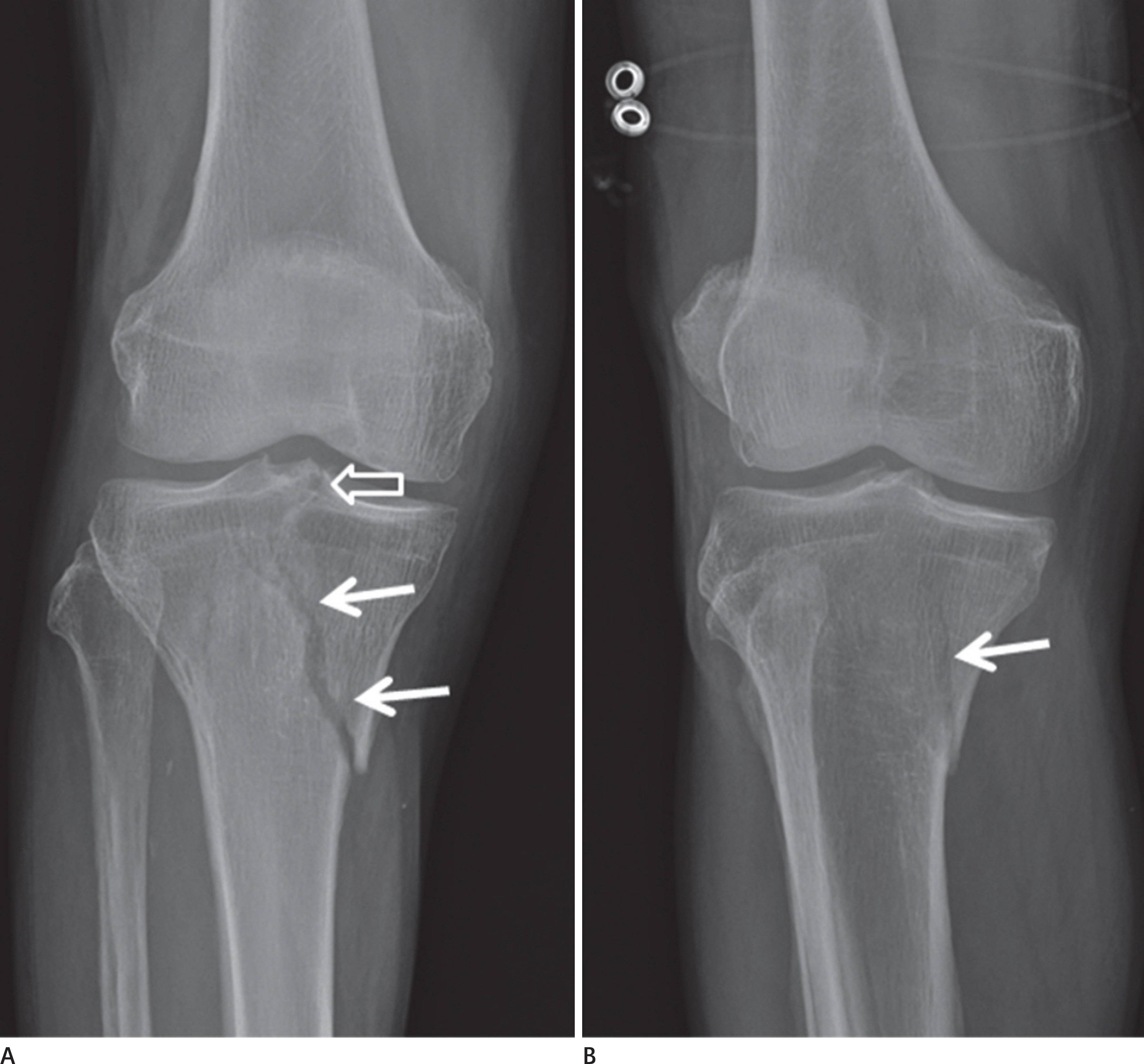
Fig. 14. Tibial plateau fracture, Schatzker classification, type IV. The fracture line is seen in the medial tibial plateau (arrows) and the intercondy-lar eminence (hollow arrow) on the (A) anteroposterior radiograph and (B) the oblique radiograph.

Fig. 15. Physeal injury of the knee joint, Salter-Harris classification, type I. The medial aspect of the growth plate of the left distal femur is wid-ened (arrows) on the (A) anteroposterior radiograph and (B) the left lateral radiograph compared with the growth plate of the right distal femur.

Fig. 16. Patellar complex fracture. A complex fracture (arrows) is seen on anteroposterior (A) and lateral (B) radiographs. Soft tissue swelling (arrowhead) in the prepatellar area is also seen on the lateral radiograph.
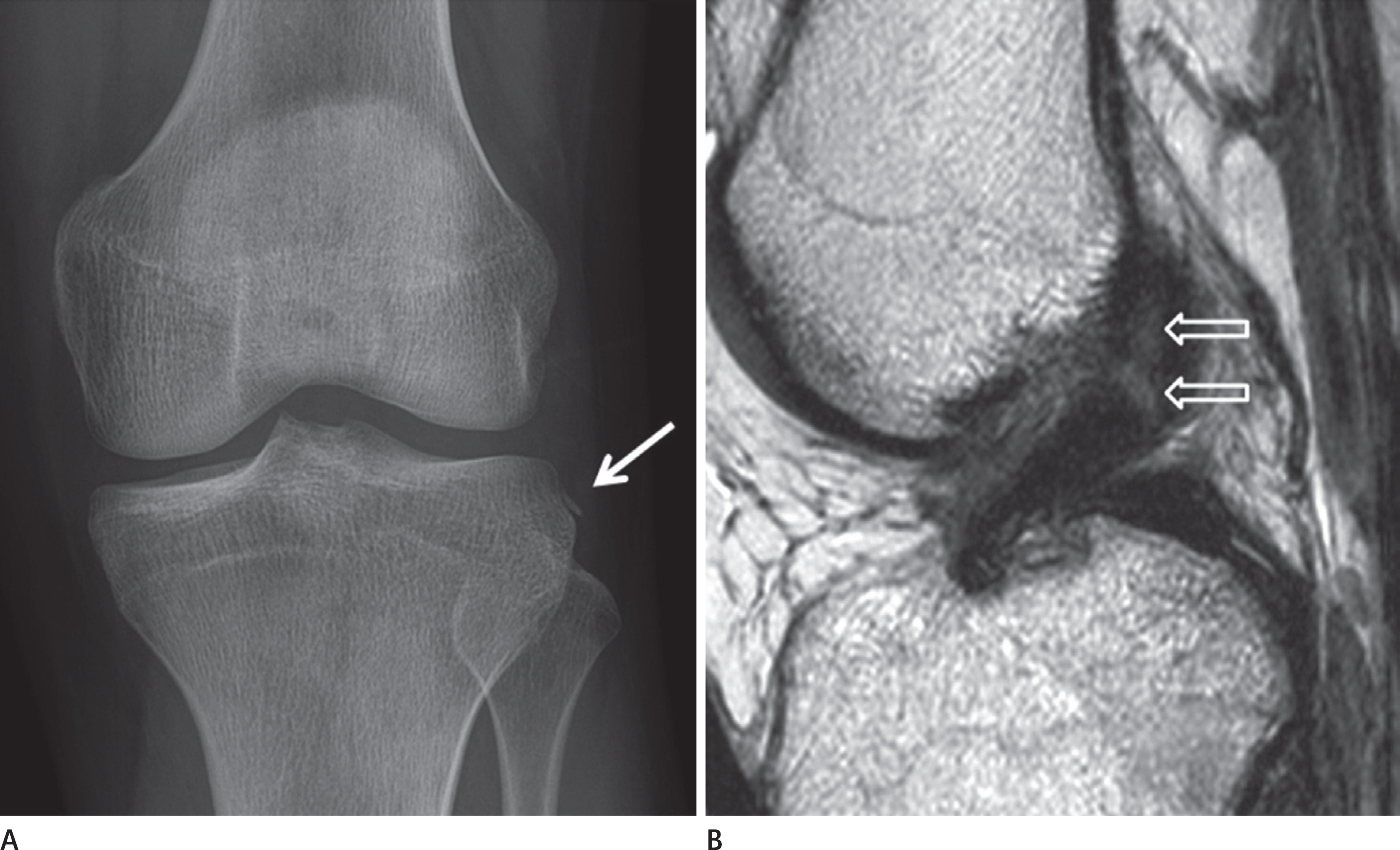
Fig. 17. Segond fracture. A. A segond fracture is seen on the lateral aspect of the lateral tibial plateau on the anteroposterior radiograph (arrow). B. There is a rupture in the proximal portion of the anterior cruciate ligament (hollow arrows) on T2-weighted sagittal magnetic resonance images.
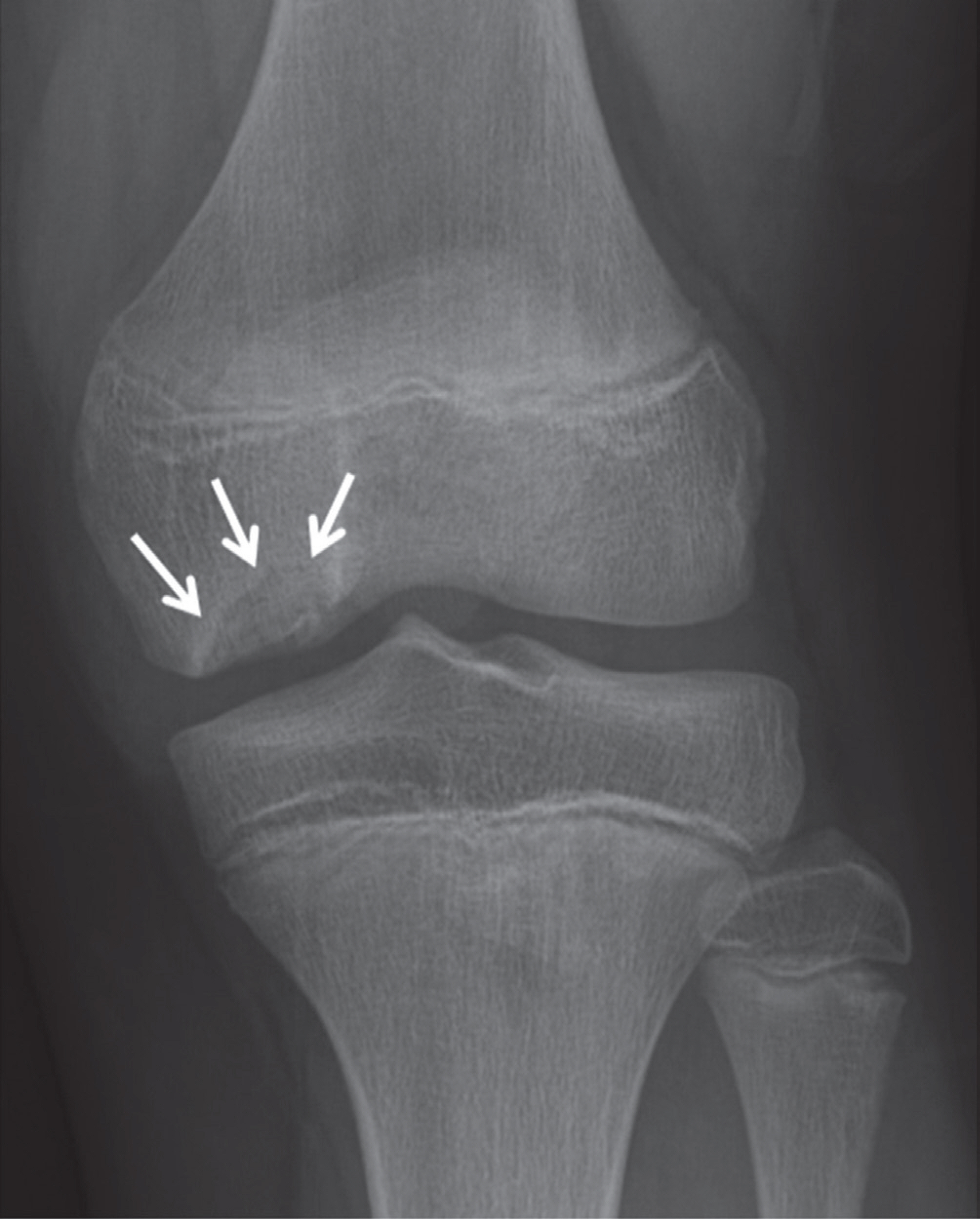
Fig. 18. Osteochondritis dissecans. The bone fragment makes contact with the articular surface of the femoral condyle and is surrounded by the radiolucent line (arrows) on the anteroposterior radiograph.
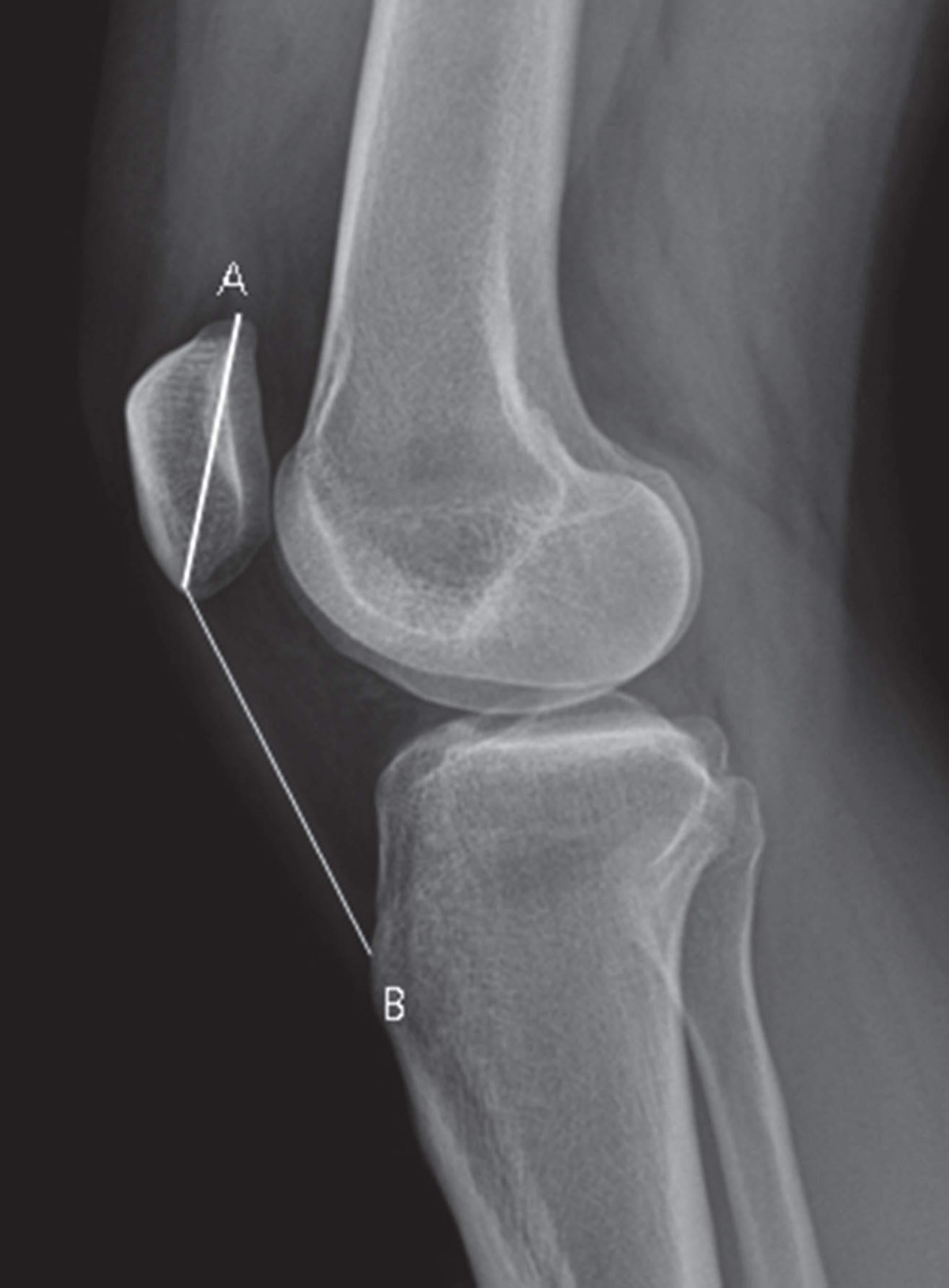
Fig. 19. Patella alta. The longest length of the patella (A) is 4.2 cm and the longest length of the patellar tendon (B) is 6.4 cm on the lateral ra-diograph; therefore, the Insall-Salvati index is 1.52. A diagnosis of pa-tella alta can be made because the Insall-Salvati index is more than 1.2.
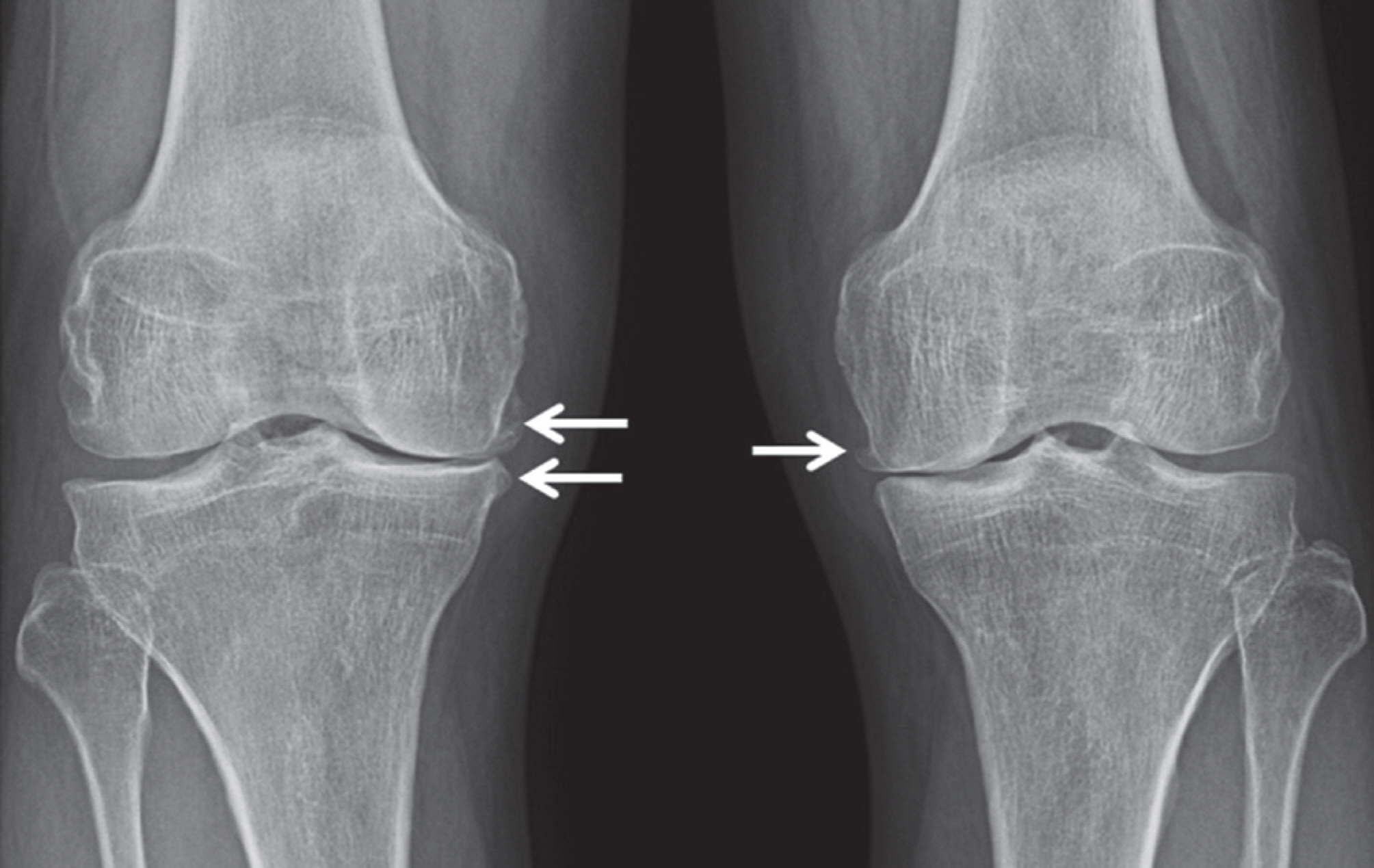
Fig. 20. Degenerative osteoarthritis of the knee joint. There is progres-sive joint space narrowing at the medial aspect of the knee joint com-pared to the lateral aspect of the knee joint. Also, there are osteo-phytes (arrows) on the medial aspect of the knee joint. The diagnosis of Kellgren-Lawrence grade 3 osteoarthritis in bilateral knee joints can be made.
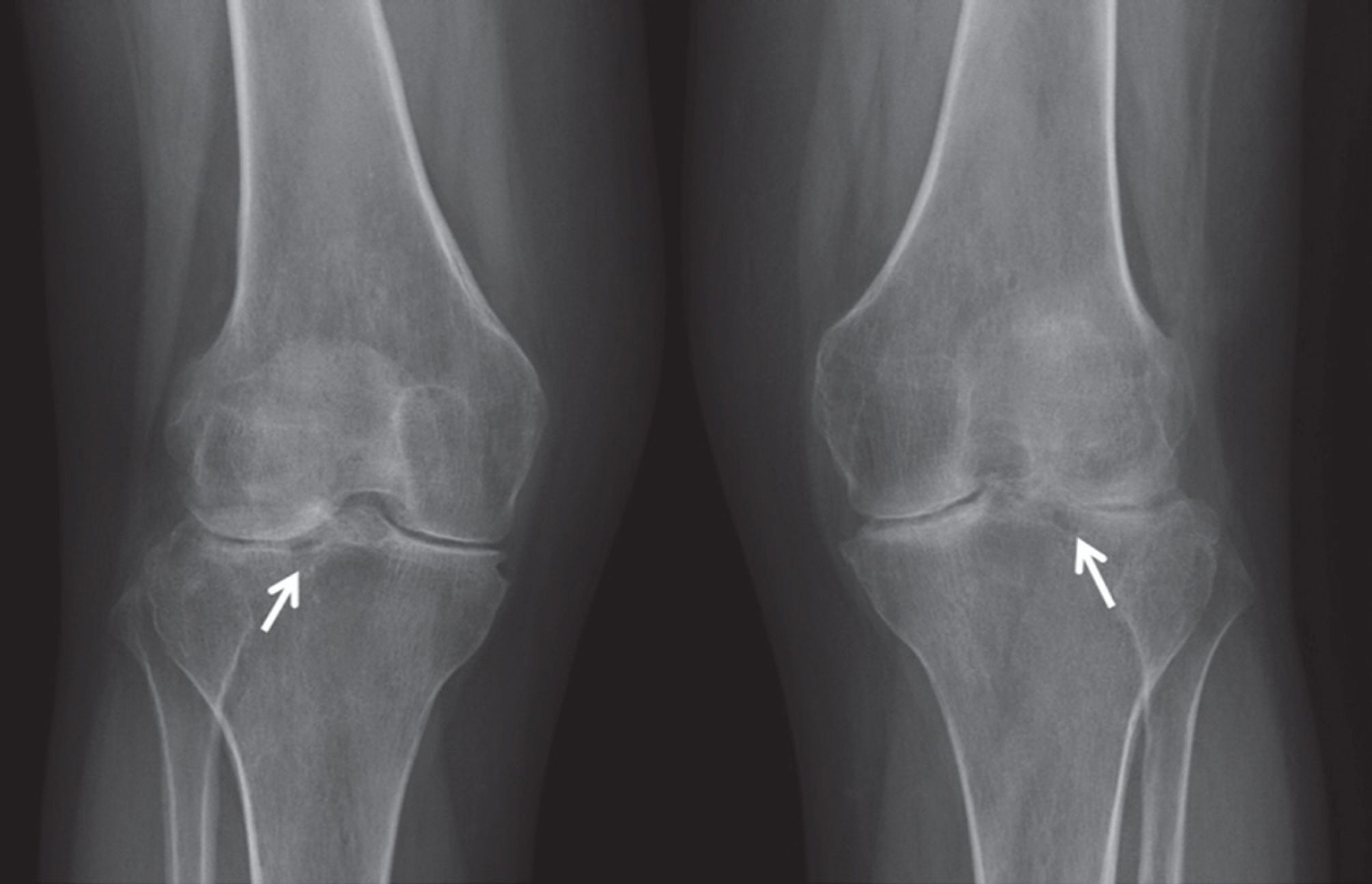
Fig. 21. Rheumatoid arthritis of the knee joint. There is symmetric joint space narrowing of bilateral knee joints. Subchondral cysts (arrows) and sclerosis are seen in the bilateral lateral tibial plateau.

Fig. 22. Lauge-Hansen classification of ankle joint fractures.
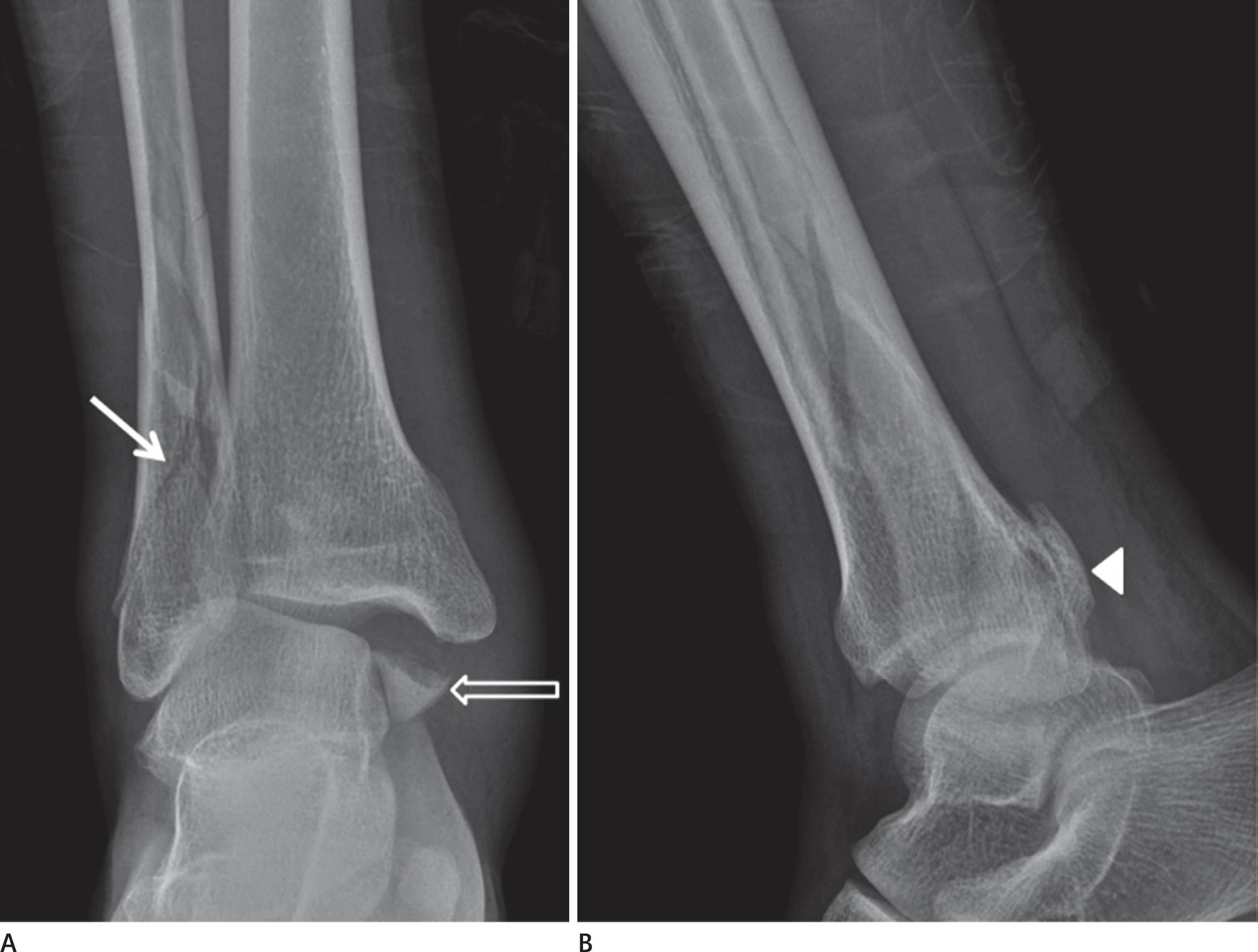
Fig. 23. Ankle joint fracture: supination–external rotation. A. A spiral fracture of the lateral malleolus (arrow) and a transverse fracture of the medial malleolus (hollow arrow) are seen on the anteroposte-rior radiograph. B. A fracture of the posterior tibial lip (arrowhead) is noted.
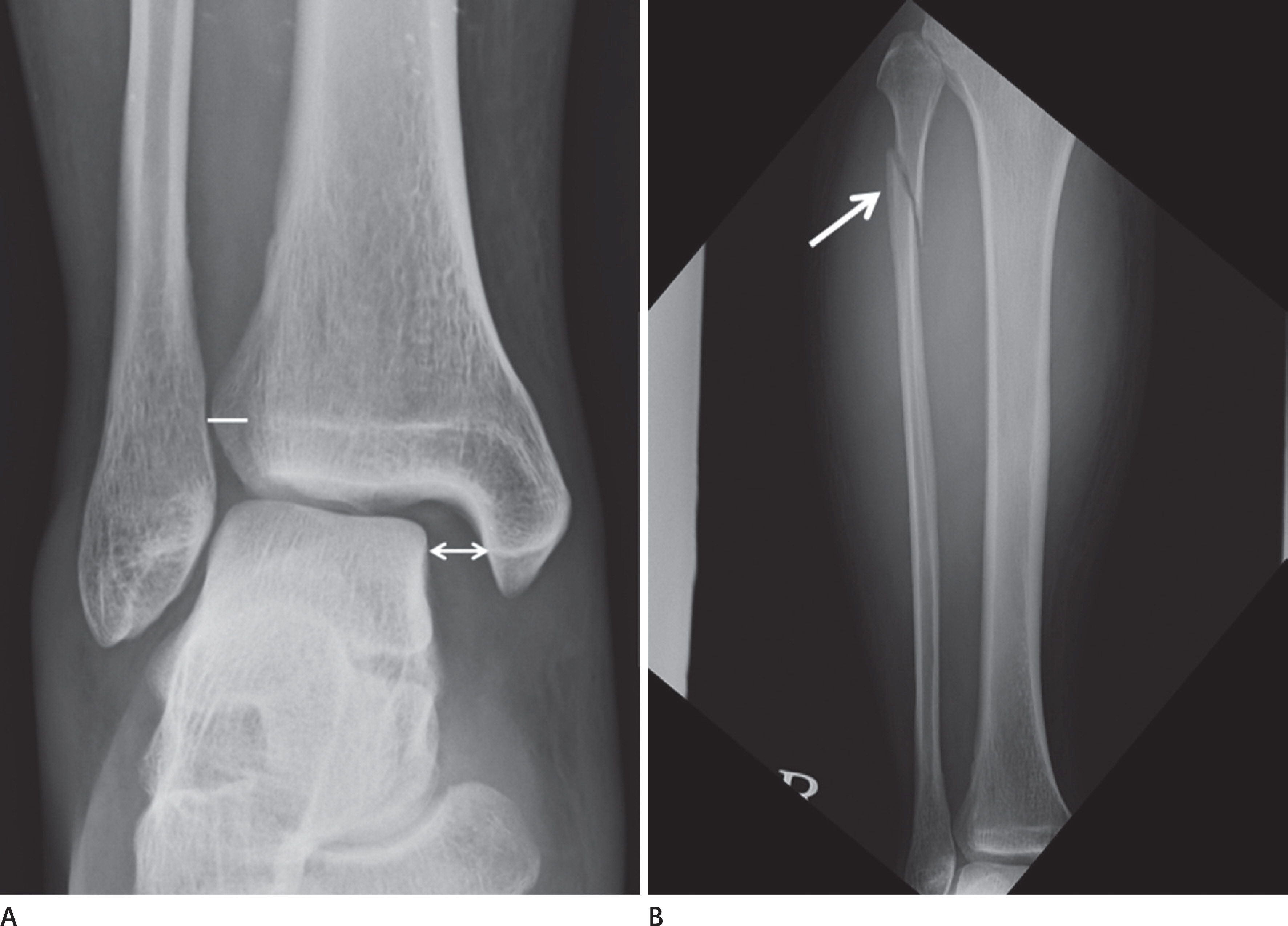
Fig. 24. Ankle joint fracture: pronation–external rotation. A. The distance between the lateral border of the medial malleolus and the medial border of the talus (medial clear space, arrow line) is 8.5 mm, and the distance between the lateral border of the tibia and the medial border of the fibula (tibiofibular overlap, white line) is 6.3 mm on the an-kle AP radiograph. Therefore, a tibiofibular syndesmosis injury is suspected. B. A fracture of the proximal fibula (arrow) is seen on the entire AP radiograph of the tibia and fibula. AP = anteroposterior

Fig. 25. Calcaneal complex fracture. There is a calcaneal complex fracture (arrows) on the (A) lateral radiograph and (B) computed tomography sagittal reformation image.

Fig. 26. Calcaneal stress fracture. An increased opacity line, which is parallel to the posterior border of the calcaneus (arrows), is noted.

Fig. 27. Osteochondral lesion of the talus. An oval-shaped decreased opacity lesion with a peripheral sclerotic border (arrow) is seen on the medial talar dome.

Fig. 28. Freiberg disease. The flattening of 2nd metatarsal head (arrows) is seen on foot anteroposterior radiograph (A) and internal oblique ra-diograph (B). The widening of 2nd MTP joint is seen compared with other MTP joints. MTP = metatarsophalangeal
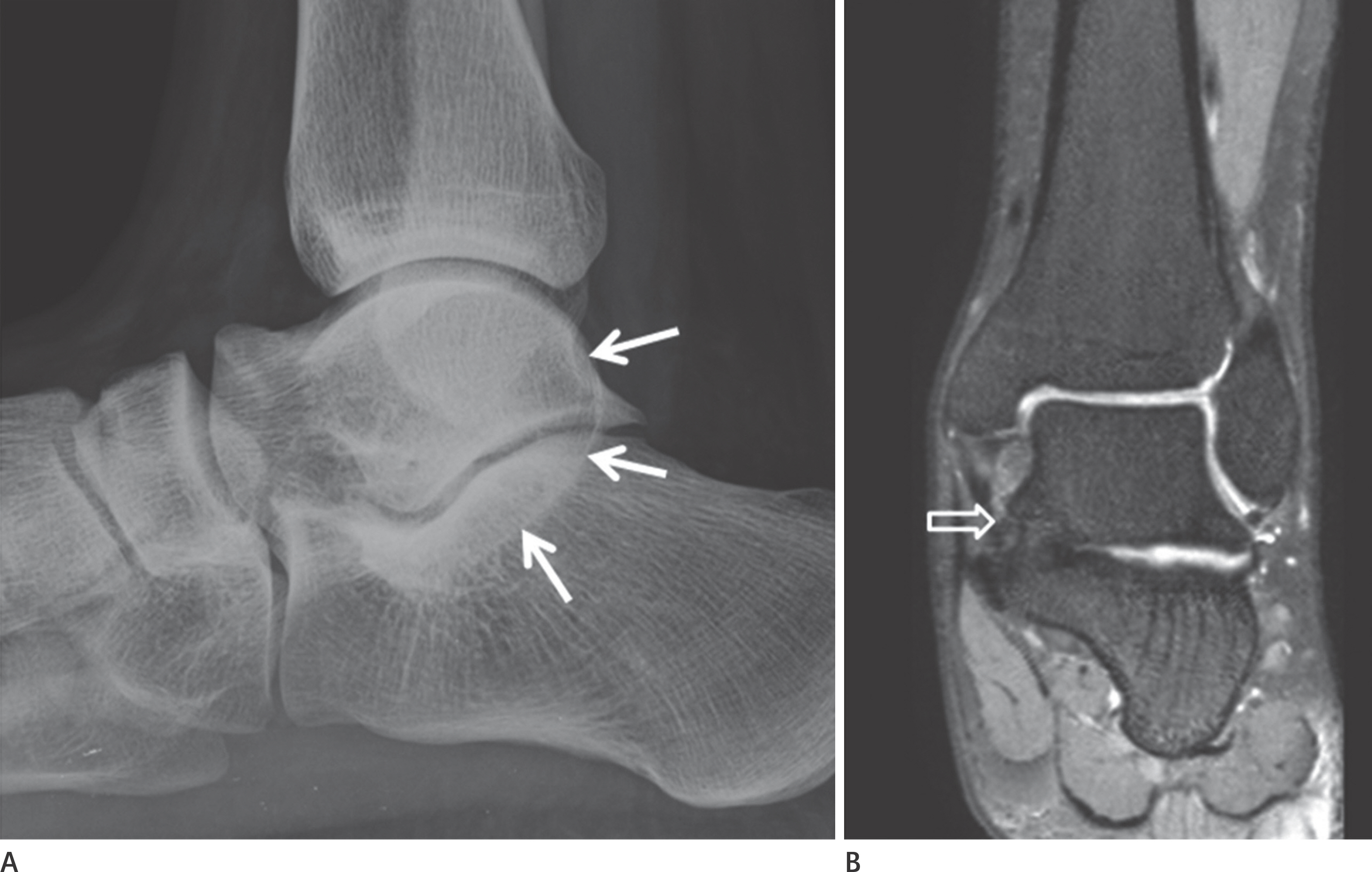
Fig. 29. Talocalcaneal coalition. A. The C-sign indicates continuation between the talar dome and the sustentaculum tali (arrows) on the lateral radiograph. B. There is continuation between the talar dome and the sustentaculum tali (hollow arrow) on the fat-suppressed proton density weighted coro-nal magnetic resonance image.

Fig. 30. Hallux valgus. The angle between the longitudinal axis of the 1st metatarsal bone and the longitudinal axis of the 1st proximal pha-lanx (hallux valgus angle) on the foot anteroposterior radiograph is 36 degrees on the right and 35 degrees on the left, respectively. In addition, the angle between the longitudinal axes of the 1st and 2nd metatarsal bones (first–second intermetatarsal angle) is 18 degrees on the right and 17 degrees on the left, respectively. Hallux valgus angles of bilateral feet are more than 15 degrees and first–second intermeta-tarsal angles are more than 10 degrees; therefore, a diagnosis of bilat-eral hallux valgus can be made.
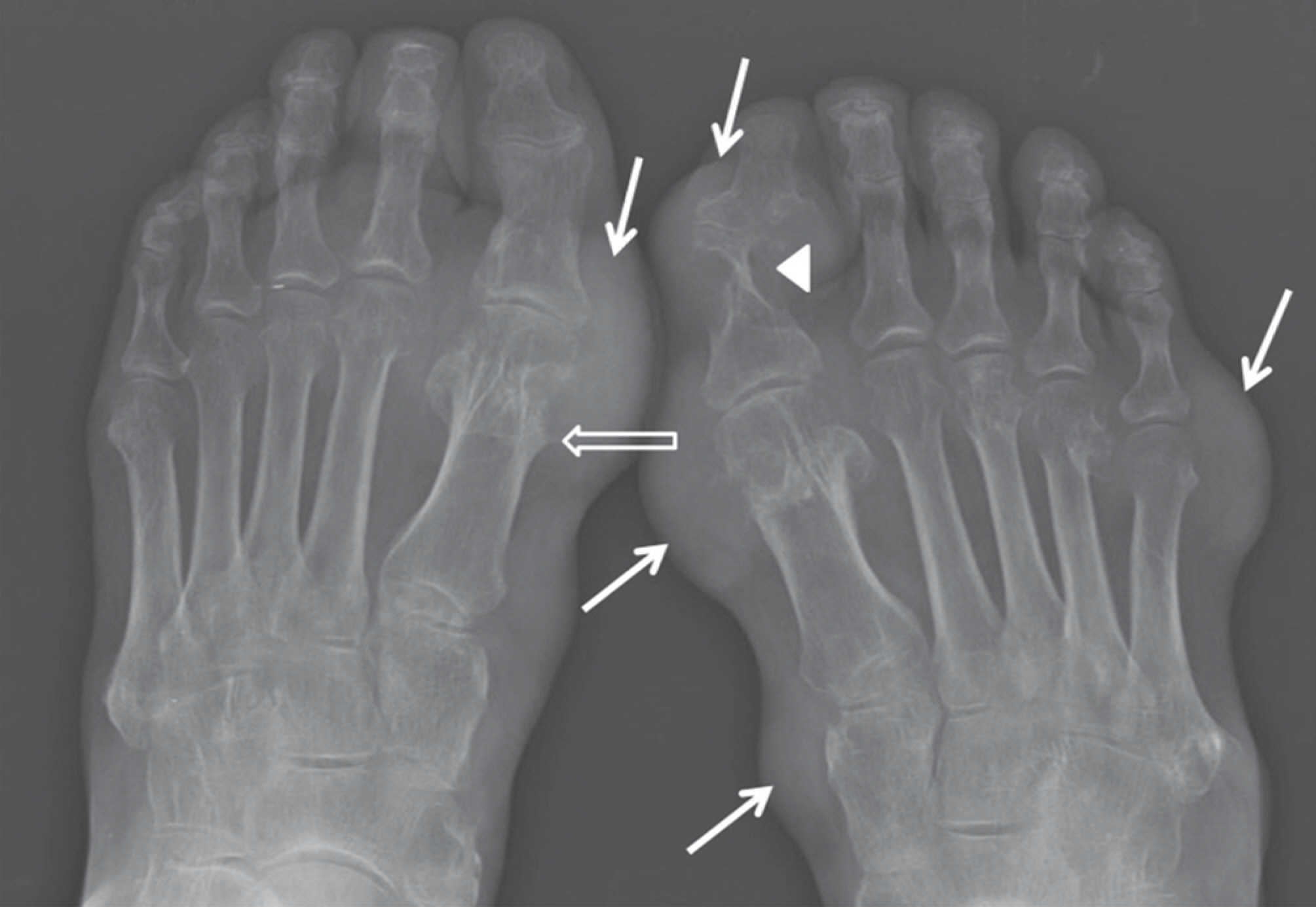
Fig. 31. Gout. There are several soft tissue opacities (arrows) on the medial and lateral aspects of bilateral feet. There are soft tissue opaci-ties and erosion on the lateral aspect of the right 1st proximal phalanx (arrowhead). The characteristic “overhanging edge” (hollow arrow) is seen on the medial aspect of the left 1st metatarsal head.
Reference
-
1.Renner JB. Conventional radiography in musculoskeletal imaging. Radiol Clin North Am. 2009. 47:357–372.
Article2.Potok PS., Hopper KD., Umlauf MJ. Fractures of the acetabu-lum: imaging, classification, and understanding. Radio-graphics. 1995. 15:7–23. discussion 23-24.
Article3.Lee SM., Lee YH. Trauma. Kang HS, Hong SH, Kang CH, editors. Musculoskeletal radiology. Reston: Bummun Education;2013. 267–339.4.Murphy D., Kaliszer M., Rice J., McElwain JP. Outcome after acetabular fracture. Prognostic factors and their inter-relationships. Injury. 2003. 34:512–517.5.Metzmaker JN., Pappas AM. Avulsion fractures of the pelvis. Am J Sports Med. 1985. 13:349–358.
Article6.Frandsen PA., Andersen E., Madsen F., Skjødt T. Garden's clas-sification of femoral neck fractures. An assessment of inter-observer variation. J Bone Joint Surg Br. 1988. 70:588–590.
Article7.Bachiller FG., Caballer AP., Portal LF. Avascular necrosis of the femoral head after femoral neck fracture. Clin Orthop Relat Res. 2002. 399:87–109.
Article8.Rosenberg ZS., La Rocca Vieira R., Chan SS., Babb J., Akyol Y., Rybak LD, et al. Bisphosphonate-related complete atypical subtrochanteric femoral fractures: diagnostic utility of ra-diography. AJR Am J Roentgenol. 2011. 197:954–960.
Article9.Schilcher J., Michaëlsson K., Aspenberg P. Bisphosphonate use and atypical fractures of the femoral shaft. N Engl J Med. 2011. 364:1728–1737.
Article10.Fisher RL. An epidemiological study of Legg-Perthes disease. J Bone Joint Surg Am. 1972. 54:769–778.
Article11.Dillon JE., Connolly SA., Connolly LP., Kim YJ., Jaramillo D. MR imaging of congenital/developmental and acquired disor-ders of the pediatric hip and pelvis. Magn Reson Imaging Clin N Am. 2005. 13:783–797.
Article12.Wilcox PG., Weiner DS., Leighley B. Maturation factors in slipped capital femoral epiphysis. J Pediatr Orthop. 1988. 8:196–200.
Article13.Boles CA., el-Khoury GY. Slipped capital femoral epiphysis. Radiographics. 1997. 17:809–823.
Article14.Boyer DW., Mickelson MR., Ponseti IV. Slipped capital femo-ral epiphysis. Long-term follow-up study of one hundred and twenty-one patients. J Bone Joint Surg Am. 1981. 63:85–95.
Article15.Kamal D., Traistaru R., Alexandru DO., Grecu DC., Mogoanta L. Epidemiologic study of avascular necrosis of the femoral head. Curr Health Sci J. 2013. 39:169–174.16.Jawad MU., Haleem AA., Scully SP. In brief: ficat classification: avascular necrosis of the femoral head. Clin Orthop Relat Res. 2012. 470:2636–2639.
Article17.Ha DH., Na JB. Pelvis and hip joint. Kang HS, Hong SH, Kang CH, editors. Musculoskeletal radiology. Reston: Bummun Education;2013. 627–669.18.Tannast M., Siebenrock KA., Anderson SE. Femoroacetabular impingement: radiographic diagnosis--what the radiolo-gist should know. Am J Roentgenol. 2007. 188:1540–1552.
Article19.Dixon T., Benjamin J., Lund P., Graham A., Krupinski E. Femoral neck buttressing: a radiographic and histologic analysis. Skeletal Radiol. 2000. 29:587–592.
Article20.Brower A. Arthritis in black and white. Philadelphia, PA: Saunders;2012. 170–199.21.Kolmert L., Wulff K. Epidemiology and treatment of distal femoral fractures in adults. Acta Orthop Scand. 1982. 53:957–962.
Article22.Sanders TG., Medynski MA., Feller JF., Lawhorn KW. Bone con-tusion patterns of the knee at MR imaging: footprint of the mechanism of injury. Radiographics. 2000. 20:Spec No:. S135–S151.
Article23.Arneson TJ., Melton LJ 3rd., Lewallen DG., O'Fallon WM. Epi-demiology of diaphyseal and distal femoral fractures in Rochester, Minnesota, 1965-1984. Clin Orthop Relat Res. 1988. 234:188–194.
Article24.Marsh JL., Slongo TF., Agel J., Broderick JS., Creevey W., De-Coster TA, et al. Fracture and dislocation classification com-pendium-2007: Orthopaedic Trauma Association classification, database and outcomes committee. J Orthop Trauma. 2007. 21(10 Suppl):S1–S133.25.Markhardt BK., Gross JM., Monu JU. Schatzker classification of tibial plateau fractures: use of CT and MR imaging im-proves assessment. Radiographics. 2009. 29:585–597.
Article26.O WH., Craig C., Banks HH. Epiphyseal injuries. Pediatr Clin North Am. 1974. 21:407–422.27.Lipp EJ. Athletic physeal injury in children and adolescents. Orthop Nurs. 1998. 17:17–22.28.Greenspan A. Lower limb, part II. Greenspan A, editor. Or-thopedic imaging: a practical approach. 5th ed.Philadel-phia: Lippincott Williams & Wilkins;2011. 258–307.29.Dupuis CS., Westra SJ., Makris J., Wallace EC. Injuries and conditions of the extensor mechanism of the pediatric knee. Radiographics. 2009. 29:877–886.
Article30.Gottsegen CJ., Eyer BA., White EA., Learch TJ., Forrester D. Avulsion fractures of the knee: imaging findings and clini-cal significance. Radiographics. 2008. 28:1755–1770.
Article31.Escobedo EM., Mills WJ., Hunter JC. The “reverse Segond" fracture: association with a tear of the posterior cruciate lig-ament and medial meniscus. AJR Am J Roentgenol. 2002. 178:979–983.32.White EA., Patel DB., Matcuk GR., Forrester DM., Lundquist RB., Hatch GF 3rd, et al. Cruciate ligament avulsion fractures: anatomy, biomechanics, injury patterns, and approach to management. Emerg Radiol. 2013. 20:429–440.
Article33.Griffith JF., Antonio GE., Tong CW., Ming CK. Cruciate liga-ment avulsion fractures. Arthroscopy. 2004. 20:803–812.
Article34.Hunter TB., Peltier LF., Lund PJ. Radiologic history exhibit. Musculoskeletal eponyms: who are those guys? Radiograph-ics. 2000. 20:819–836.35.McAnally JL., Southam SL., Mlady GW. New thoughts on the origin of Pellegrini-Stieda: the association of PCL injury and medial femoral epicondylar periosteal stripping. Skeletal Radiol. 2009. 38:193–198.
Article36.Sundararajan SR., Rajasekaran S., Bernard SL. Displaced ante-rior cruciate ligament avulsion fractures: arthroscopic sta-ple fixation. Indian J Orthop. 2011. 45:324–329.
Article37.Juhng SK., Park JG. Knee, part II. Kang HS, Hong SH, Kang CH, editors. Musculoskeletal radiology. Reston: Bummun Edu-cation;2013. 715–744.38.De Smet AA., Fisher DR., Burnstein MI., Graf BK., Lange RH. Val-ue of MR imaging in staging osteochondral lesions of the talus (osteochondritis dissecans): results in 14 patients. AJR Am J Roentgenol. 1990. 154:555–558.
Article39.Stevens MA., El-Khoury GY., Kathol MH., Brandser EA., Chow S. Imaging features of avulsion injuries. Radiographics. 1999. 19:655–672.
Article40.Insall J., Salvati E. Patella position in the normal knee joint. Radiology. 1971. 101:101–104.
Article41.Caton J., Deschamps G., Chambat P., Lerat JL., Dejour H. [Patella infera. Apropos of 128 cases]. Rev Chir Orthop Reparatrice Appar Mot. 1982. 68:317–325.42.Blackburne JS., Peel TE. A new method of measuring patel-lar height. J Bone Joint Surg Br. 1977. 59:241–242.
Article43.Dath R., Chakravarthy J., Porter KM. Patella dislocations. Trauma. 2006. 8:5–11.
Article44.Sung MS., Chun KA. Degenerative joint disease. Kang HS, Hong SH, Kang CH, editors. Musculoskeletal radiology. Reston: Bummun Education;2013. 147–163.45.Kellgren JH., Lawrence JS. Radiological assessment of osteo-arthrosis. Ann Rheum Dis. 1957. 16:494–502.
Article46.Arimoto HK., Forrester DM. Classification of ankle fractures: an algorithm. AJR Am J Roentgenol. 1980. 135:1057–1063.
Article47.Arastu MH., Demcoe R., Buckley RE. Current concepts review: ankle fractures. Acta Chir Orthop Traumatol Cech. 2012. 79:473–483.48.Sclafani SJ. Ligamentous injury of the lower tibiofibular syndesmosis: radiographic evidence. Radiology. 1985. 156:21–27.
Article49.Greenspan A. Lower limb, part III. Greenspan A, editor. Or-thopedic imaging: a practical approach. 5th ed.Philadel-phia: Lippincott Williams & Wilkins;2011. 294–345.50.Badillo K., Pacheco JA., Padua SO., Gomez AA., Colon E., Vidal JA. Multidetector CT evaluation of calcaneal fractures. Ra-diographics. 2011. 31:81–92.
Article51.Hardcastle PH., Reschauer R., Kutscha-Lissberg E., Schoffmann W. Injuries to the tarsometatarsal joint. Incidence, classification and treatment. J Bone Joint Surg Br. 1982. 64:349–356.
Article52.Burroughs KE., Reimer CD., Fields KB. Lisfranc injury of the foot: a commonly missed diagnosis. Am Fam Physician. 1998. 58:118–124.53.Goiney RC., Connell DG., Nichols DM. CT evaluation of tarso-metatarsal fracture-dislocation injuries. AJR Am J Roentgen-ol. 1985. 144:985–990.
Article54.Alexander AH., Lichtman DM. Surgical treatment of tran-schondral talar-dome fractures (osteochondritis dissecans). Long-term follow-up. J Bone Joint Surg Am. 1980. 62:646–652.
Article55.Choi YS., Chun TJ. Foot and ankle. Kang HS, Hong SH, Kang CH, editors. Musculoskeletal radiology. Reston: Bummun Education;2013. 745–798.56.Naran KN., Zoga AC. Osteochondral lesions about the an-kle. Radiol Clin North Am. 2008. 46:995–1002.
Article57.Pearce DH., Mongiardi CN., Fornasier VL., Daniels TR. Avascu-lar necrosis of the talus: a pictorial essay. Radiographics. 2005. 25:399–410.
Article58.Park JS., Ryu KN. Osteonecrosis and osteochondrosis. Kang HS, Hong SH, Kang CH, editors. Musculoskeletal radiolo-gy. Reston: Bummun Education;2013. 229–265.59.Torriani M., Thomas BJ., Bredella MA., Ouellette H. MRI of meta-tarsal head subchondral fractures in patients with forefoot pain. AJR Am J Roentgenol. 2008. 190:570–575.
Article60.Ashman CJ., Klecker RJ., Yu JS. Forefoot pain involving the metatarsal region: differential diagnosis with MR imaging. Radiographics. 2001. 21:1425–1440.
Article61.Staheli LT., Chew DE., Corbett M. The longitudinal arch. A sur-vey of eight hundred and eighty-two feet in normal chil-dren and adults. J Bone Joint Surg Am. 1987. 69:426–428.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Dynamic Ultrasonography in Musculoskeletal System-Lower Extremity and Miscellaneous disorders
- Musculoskeletal ultrasound: athletic injuries of the lower extremity
- Dynamic Ultrasonography in Musculoskeletal System: Upper Extremity
- Commuting time and musculoskeletal pain in the relationship with working time: a cross-sectional study
- The Role of Fat Tissues in the Diagnosis of Musculoskeletal Imaging
