Korean Circ J.
2017 Jul;47(4):516-522. 10.4070/kcj.2016.0163.
Long-Term Prognosis for Patients with Kawasaki Disease Complicated by Large Coronary Aneurysm (diameter ≥6 mm)
- Affiliations
-
- 1Department of Pediatrics, Seoul National University Children's Hospital, Seoul, Korea. ped9526@snu.ac.kr
- 2Department of Pediatrics, Sejong General Hospital, Bucheon, Korea.
- 3Department of Pediatrics, Seoul National University Boramae Hospital, Seoul, Korea.
- 4Department of Pediatrics, Bundang Seoul National University Hospital, Seongnam, Korea.
- KMID: 2392890
- DOI: http://doi.org/10.4070/kcj.2016.0163
Abstract
- BACKGROUND AND OBJECTIVES
Some patients with Kawasaki disease (KD) develop large coronary aneurysms and subsequent coronary stenosis or obstruction, leading to ischemic heart disease. This study examined the long-term outcomes of patients with KD complicated by large coronary aneurysms.
SUBJECTS AND METHODS
The medical records of 71 patients (53 men and 18 women) diagnosed with large coronary aneurysms (diameter ≥6 mm) between December 1986 and December 2013 were retrospectively reviewed from our institutional database.
RESULTS
The mean age at onset was 4.6±3.3 years, and the mean follow-up duration was 12.5±6.9 years. Maximum coronary artery internal diameter ranged from 6.1 to 25 mm. Giant coronary aneurysms occurred in 48 patients and coronary aneurysms 6-8 mm in diameter developed in 23 patients. Coronary stenosis and/or complete occlusion occurred in 30 patients (42.3%). Catheter and/or surgical interventions (mean: 1.5 interventions, range: 1-5 interventions) were performed in 20 patients (28.2%), 9 months to 18 years after KD onset, resulting in 33.7% cumulative coronary intervention rates at 20 years after onset. There were no differences in cumulative coronary intervention rates between two coronary aneurysm groups (6-8 mm vs. ≥8 mm). Myocardial infarction occurred in 7 patients with a giant aneurysm and there was one death.
CONCLUSIONS
Long-term survival of patients with KD complicated by large coronary aneurysm was good even though 28.2% of patients underwent multiple catheter or surgical interventions. Careful follow-up is also necessary in KD patients with coronary aneurysms 6-8 mm in diameter, such as those with giant aneurysms.
MeSH Terms
Figure
-
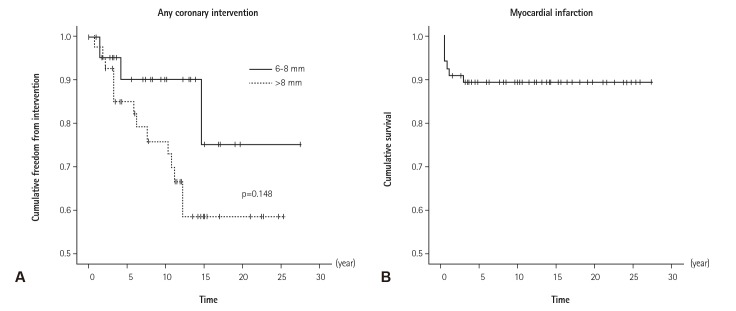
Fig. 1 Kaplan-Meier actuarial freedom from cardiac events. (A) Freedom from any intervention between coronary aneurysm size (6-8 mm vs. ≥8 mm). Trans-catheter and/or surgical coronary interventions were performed in 20 patients, resulting in a 33.7% cumulative coronary intervention rate at 20 years after KD onset. There were no differences in cumulative coronary intervention rates between two coronary aneurysm groups (p=0.148). (B) Freedom from myocardial infarction. The median elapsed time from KD onset to myocardial infarction was 3.0 months (range: 0.5-31.2 months). Cumulative survival rate was 89.6% and most myocardial infarction occurred in the first year after onset of giant coronary aneurysm. KD: Kawasaki disease.
Reference
-
1. Yanagawa H, Nakamura Y, Yashiro M, Uehara R, Oki I, Kayaba K. Incidence of Kawasaki disease in Japan: the nationwide surveys of 1999-2002. Pediatr Int. 2006; 48:356–361. PMID: 16911079.2. Newburger JW, Takahashi M, Gerber MA, et al. Diagnosis, treatment, and long-term management of Kawasaki disease: a statement for health professionals from the Committee on rheumatic fever, endocarditis and Kawasaki disease, Council on cardiovascular disease in the young, American heart association. Circulation. 2004; 110:2747–2771. PMID: 15505111.3. Uehara R, Belay ED. Epidemiology of Kawasaki disease in Asia, Europe, and the United States. J Epidemiol. 2012; 22:79–85. PMID: 22307434.4. Onouchi Z, Hamaoka K, Sakata K, et al. Long-term changes in coronary artery aneurysms in patients with Kawasaki disease: comparison of therapeutic regimens. Circ J. 2005; 69:265–272. PMID: 15731529.5. Kato H, Sugimura T, Akagi T, et al. Long-term consequences of Kawasaki disease. A 10- to 21-year follow-up study of 594 patients. Circulation. 1996; 94:1379–1385. PMID: 8822996.6. Kato H, Koike S, Yamamoto M, Ito Y, Yano E. Coronary aneurysms in infants and young children with acute febrile mucocutaneous lymph node syndrome. J Pediatr. 1975; 86:892–898. PMID: 236368.7. Suda K, Iemura M, Nishiono H, et al. Long-term prognosis of patients with Kawasaki disease complicated by giant coronary aneurysms: a single-institution experience. Circulation. 2011; 123:1836–1842. PMID: 21502578.8. Jang GY, Kang IS, Choi JY, et al. Nationwide survey of coronary aneurysms with diameter >6 mm in Kawasaki disease in Korea. Pediatr Int. 2015; 57:367–372. PMID: 25406095.9. Akagi T, Rose V, Benson LN, Newman A, Freedom RM. Outcome of coronary artery aneurysms after Kawasaki disease. J Pediatr. 1992; 121(5 Pt 1):689–694. PMID: 1432415.10. AlHuzaimi A, Al Mashham Y, Potts JE, De Souza AM, Sandor GG. Echo-Doppler assessment of arterial stiffness in pediatric patients with Kawasaki disease. J Am Soc Echocardiogr. 2013; 26:1084–1089. PMID: 23800509.11. Gong F, Shiraishi H, Momoi MY. Follow-up of coronary artery lesions caused by Kawasaki disease and the value of coronary angiography. Chin Med J (Engl). 2002; 115:681–684. PMID: 12133534.12. Peng Y, Zeng J, Du Z, Sun G, Guo H. Usefulness of 64-slice MDCT for follow-up of young children with coronary artery aneurysm due to Kawasaki disease: initial experience. Eur J Radiol. 2009; 69:500–509. PMID: 18164157.13. Sohn S, Kim HS, Lee SW. Multidetector row computed tomography for follow-up of patients with coronary artery aneurysms due to Kawasaki disease. Pediatr Cardiol. 2004; 25:35–39. PMID: 14583832.14. Ohmoto-Sekine Y, Ishihara M, Hsieh SD, et al. Giant coronary artery aneurysms associated with Kawasaki disease detected on whole-heart magnetic resonance coronary angiographic screening. Intern Med. 2013; 52:977–980. PMID: 23648717.15. Kitamura S, Kameda Y, Seki T, et al. Long-term outcome of myocardial revascularization in patients with Kawasaki coronary artery disease. A multicenter cooperative study. J Thorac Cardiovasc Surg. 1994; 107:663–673. discussion 673-4. PMID: 8127095.16. Gu C, Fan S, Zhou H, et al. Surgical treatment of giant coronary artery aneurysm secondary to Kawasaki disease. Heart Surg Forum. 2009; 12:E241–E243. PMID: 19683998.17. Waki K, Arakaki Y, Mitsudo K. Long-term outcome of transcatheter polytetrafluoroethylene-covered stent implantation in a giant coronary aneurysm of a child with Kawasaki disease. Catheter Cardiovasc Interv. 2013; 81:713–716. PMID: 22605684.18. Muta H, Ishii M. Percutaneous coronary intervention versus coronary artery bypass grafting for stenotic lesions after Kawasaki disease. J Pediatr. 2010; 157:120–126. PMID: 20304414.19. Kato H, Ichinose E, Kawasaki T. Myocardial infarction in Kawasaki disease: clinical analyses in 195 cases. J Pediatr. 1986; 108:923–927. PMID: 3712157.20. Harada M, Akimoto K, Ogawa S, et al. National Japanese survey of thrombolytic therapy selection for coronary aneurysm: intracoronary thrombolysis or intravenous coronary thrombolysis in patients with Kawasaki disease. Pediatr Int. 2013; 55:690–695. PMID: 23919576.21. Lee J, Kim GB, Kwon BS, Bae EJ, Noh CI. Two cases of super-giant coronary aneurysms after kawasaki disease. Korean Circ J. 2014; 44:54–58. PMID: 24497892.22. Muta H, Ishii M, Iemura M, Matsuishi T. Health-related quality of life in adolescents and young adults with a history of Kawasaki disease. J Pediatr. 2010; 156:439–443. PMID: 19969307.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Long-Term Outcome of Kawasaki Disease Complicated by a Large Coronary Aneurysm
- Long Term Follow-up Study of Patients with Kawasaki Disease
- A Clinical Observation of Kawasaki Disease at High Risk of Coronary Artery Aneurysm
- Thrombolytic Therapy and Long Term Follow-up Study in a Child with Kawasaki Disease Complicated by Giant Coronary Aneurysm with Thrombosis
- Percutaneous Transluminal Coronary Angioplasty for Coronary Artery Stenosis in an Adult Kawasaki Disease with Coronary Aneurysm : A Case Report and Review
