J Korean Endocr Soc.
2006 Dec;21(6):536-541.
A Case of Autoimmune Hypoglycemia due to Insulin Antibody in Patient with End Stage Renal Disease
- Affiliations
-
- 1Department of Internal Medicine, Yonsei University College of Medicine, Korea.
Abstract
- Fasting hypoglycemia results from several mechanisms. Autoimmune hypoglycemia is one of the rare causes of hypoglycemia, and characterized by hyperinsulinemia, fasting hypoglycemia and the presence of autoantibodies to insulin or insulin receptor. We report here on a 64-year-old male patient with autoimmune hypoglycemia with end stage renal disease. He had no history of diabetes or insulin use. He had experienced several severe hypoglycemic events. The serum C-peptide level was 7.48 ng/mL and the insulin concentration was 115.4 micro U/mL when the fasting plasma glucose level was 88 mg/dL. The insulin to glucose ratio was 5.42, which suggested the presence of insulinoma. Yet the radiologic studies, including magnetic resonance cholangiopancreatography, endoscopic ultrasonography and selective calcium stimulated venous sampling revealed no evidence of insulinoma. The insulin autoantibody level was 62 micro U/mL. Therefore, we could diagnosis the autoimmune hypoglycemia. The hypoglycemia was treated with prednisolone and the patient recovered from this. His insulin level decreased to 21.11 micro U/mL and the insulin autoantibody level decreased to 34 micro U/mL. Hypoglycemia in the hemodialysis patients is not uncommon. One should bear in mind autoimmune hypoglycemia as one of the causes of hypoglycemia in patients with no history of diabetes.
MeSH Terms
-
Autoantibodies
Blood Glucose
C-Peptide
Calcium
Cholangiopancreatography, Magnetic Resonance
Diagnosis
Endosonography
Fasting
Glucose
Humans
Hyperinsulinism
Hypoglycemia*
Insulin*
Insulinoma
Kidney Failure, Chronic*
Male
Middle Aged
Prednisolone
Receptor, Insulin
Renal Dialysis
Autoantibodies
C-Peptide
Calcium
Glucose
Insulin
Prednisolone
Receptor, Insulin
Figure
-

Fig. 1 Pancreatobiliary magnetic resonance cholangiopancreatography & magnetic resonance image show no definite evidence of tumor.
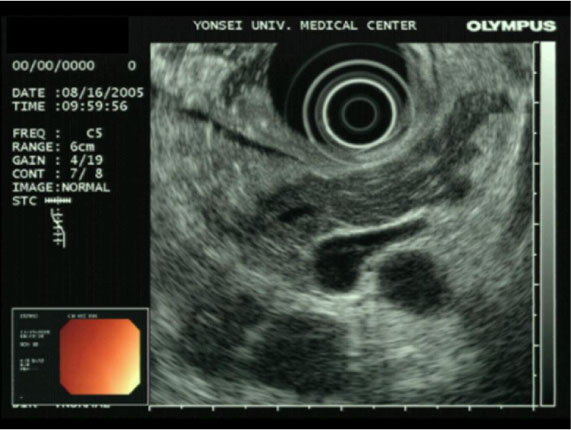
Fig. 2 Endoscopic ultrasonogram shows no definite mass lesion presented in pancreas.

Figure 3 Celiac angiography shows normal findings.
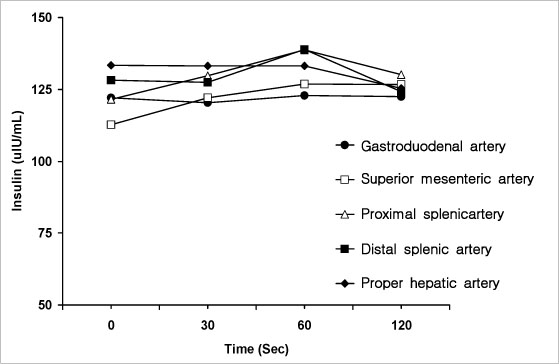
Fig. 4 Insulin levels during selective arterial calcium stimulation venous sampling.
Reference
-
1. Hirata Y, Ishizu H, Ouchi N, Motomura S, Abe M, Hara Y, Wakasugi H, Takahashi I, Sakano H, Tanaka M, Kawano H, Kanesaki T. Insulin autoimmunity in a case of spontaneous hypoglycemia. J Jpn Diabetes Soc. 1970. 13:312–320.2. Uchigata Y, Eguchi Y, Takayama-Hasumi S, Omori Y. Insulin autoimmune syndrome (Hirata Disease): clinical features and epidemiology in Japan. Diabetes Res Clin Pract. 1994. 22:89–94.3. Takayama-Hasumi S, Eguchi Y, Sato A, Morita C, Hirata Y. Insulin autoimmune syndrome is the third leading cause of spontaneous hypoglycemia attacks in Japan. Diabetes Res Clin Pract. 1990. 10:211–214.4. Cho BY, Lee HK, Koh CS, Min HK. Spontaneous hypoglycemia and insulin autoantibodies in a patient with Graves' disease. Diabetes Res Clin Pract. 1987. 3:119 –124.5. Park SH, Lee SW, Jeong GH, Choi CH, Lee SH, Han JH, Kim JG, Ha SW, Kim BW. Two cases of autoimmune insulin syndrome with hypoglycemia. J Kor Soc Endocrinol. 2001. 16:508–513.6. Block MB, Rubenstein AH. Spontaneous hypoglycemia in diabetic patients with renal insufficiency. JAMA. 1970. 213:1863–1866.7. Arem R. Hypoglycemia associated with renal failure. Endocrinol Metab Clin North Am. 1989. 18:103–121.8. Mak RH. Impact of end-stage renal disease and dialysis on glycemic control. Semin Dial. 2000. 13:4–8.9. Berson S, Yalow R, Bauman A, Rothschild MA, Newerly K. Insulin 131I metabolism in human subjects: demonstration of insulin binding globulin in the circulation of insulin treated subjects. J Clin Invest. 1956. 35:170–190.10. Redmon B, Nuttall F. Autoimmune hypoglycemia. Endocrinol Metab Clin North Am. 1999. 28:603–618.11. Wilkin TJ, Mirza I, Hammonds P, Bone A, Webster K. Graves' disease of the beta cell: glucose dysregulation due to islet-cell stimulating antibodies. Lancet. 1988. 332:1155–1158.12. Eguchi Y, Uchigata Y, Yao K, Yokoyama H, Hirata Y, Omri Y. Longitudinal changes of serum insulin concentration and insulin antibody features in persistent insulin autoimmune syndrome (Hirata's disease). Autoimmunity. 1994. 19:279–284.13. Redmon B, Pyzdrowski KL, Elson MK, Kay NE, Dalmasso AP, Nuttall FQ. Brief report: Hypoglycemia due to a monoclonal insulin-binding antibody in multiple myeloma. N Engl J Med. 1992. 326:994–998.14. Uchigata Y, Eguchi Y, Takayama-Hasumi S, Omon Y, Hirata Y, Kuwata S, Tokunaga K, Miyamoto M, Juji T. Strong association of insulin autoimmune syndrome with HLA-DR4. Lancet. 1992. 339:393–394.15. Uchigata Y, Kuwata S, Tsushima T, Tokunaga K, Miyamoto M, Tsuchikawa K, Hirata Y, Juji T, Omori Y. Patients with Graves' disease who developed insulin autoimmune syndrome (Hirata disease) possess HLA Bw62/Cw4/DR4 carrying DRB1*0406. J Clin Endocrinol Metab. 1993. 77:249–254.16. Hirata Y, Uchigata Y. Insulin autoimmune syndrome in Japan. Diabetes Res Clin Pract. 1994. 24:153–157.17. Moreira RO, Lima GA, Peixoto PC, Farias ML, Vaisman M. Insulin autoimmune syndrome: case report. Sao Paulo Med J. 2004. 122:178–180.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A case of autoimmune hypoglycemia during treatment with anti-tuberculosis drugs
- A Case of Autoimmune Hypoglycemia Complicated with Diabetic Ketoacidosis
- A case of insulin autoimmune syndrome
- Spontaneous Hypoglycemia due to Insulin Antibody after Insulin Treatment of Diabetic Ketoacidosis
- Anti-tuberculosis Treatment-Induced Insulin Autoimmune Syndrome
