Nerve Transfer to Restore Upper Extremity Function
- Affiliations
-
- 1Department of Orthopaedic Surgery, Seoul National University Hospital, Seoul National University College of Medicine, Seoul, Korea. orthoyhl@snu.ac.kr
- KMID: 2391212
- DOI: http://doi.org/10.12790/jkssh.2017.22.3.154
Abstract
- The term "˜Nerve Transfer' means the transfer of a normal or nearly normal fascicle or nerve branch to an important sensory or motor nerve that has sustained irreparable proximal damage. It is a kind of salvage procedure performed when the proximal part of a peripheral nerve is totally damaged and impossible to be repaired. In case of irreparable preganglionic injury, it is difficult to recovery the nerve function by only nerve graft. In this case, the uninjured nerve around the brachial plexus could be transferred to restore the function of the upper extremities. Previous studies have reported a high recovery rate for the function of the upper limb above the elbow and recent efforts have been made to restore the function of the upper limb below the elbow including hand functions. The purpose of this article is to review the type of nerve transfer to restore upper extremity function, operative technique, outcomes and complication.
Figure
-
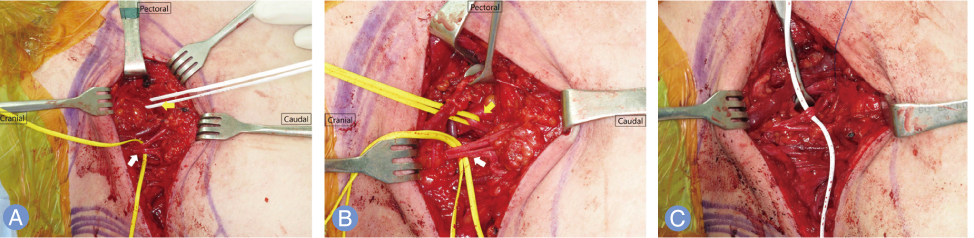
Fig. 1 Spinal accessory nerve transfer (distal motor branch) to suprascapular nerve for the patients with suprascapular nerve palsy due to brachial plexus injury. (A) Distal motor branch of spinal accessory nerve. Inferior loop (white arrow), distal motor branch of spinal accessory nerve; superior loop (yellow arrow), omohyoid muscle. (B) Superior loop (yellow arrow), suprascapular nerve; inferior loop (white arrow), distal motor branch of spinal accessory nerve. (C) Transfer distal motor branch of spinal accessory nerve to suprascapular nerve.
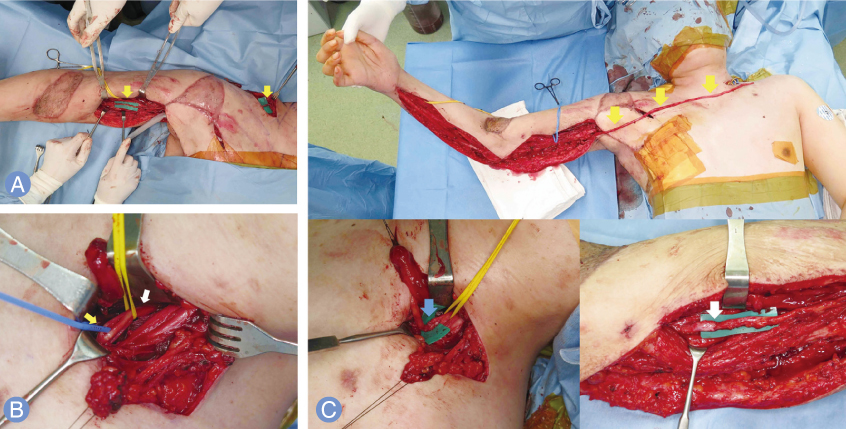
Fig. 2 This patient sustained whole arm type brachial plexus injury. His suprascapular nerve function remained, and the intercostal nerve could not be used as a donor due to damage of the chest wall. We did spinal accessory nerve (distal motor branch) transfer to musculocutaneous nerve (motor branch to brachialis and biceps muscle) with sural nerve graft. After that, contralateral C7 nerve (ventral division) transfer to median nerve using vascularized pedicled ulnar nerve graft was done. (A) Spinal accessory nerve was used to neurotize the musculocutaneous nerve (motor branch to brachialis and biceps muscle) with an interpositional sural nerve graft (yellow arrow). (B) Contralateral C7 nerve were dissected for transfer. Right loop (white arrow), C7 root; left loop (yellow arrow), anterior division. (C) Ipsilateral ulnar nerve was used as pedicled graft based on the superior ulnar collateral vessels to neurotize the median nerve. Its distal end is cut at the wrist level and mobilized in its full length to reach to contralateral C7 nerve (yellow arrows). The distal stump of the ulnar nerve is passed under the skin of the upper part of the chest to the contralateral C7 nerve. The anterior division of C7 nerve is matched and coapted to the distal end of the ulnar nerve (blue arrow). The proximal end of the ulnar nerve was sutured to median nerve (white arrow).
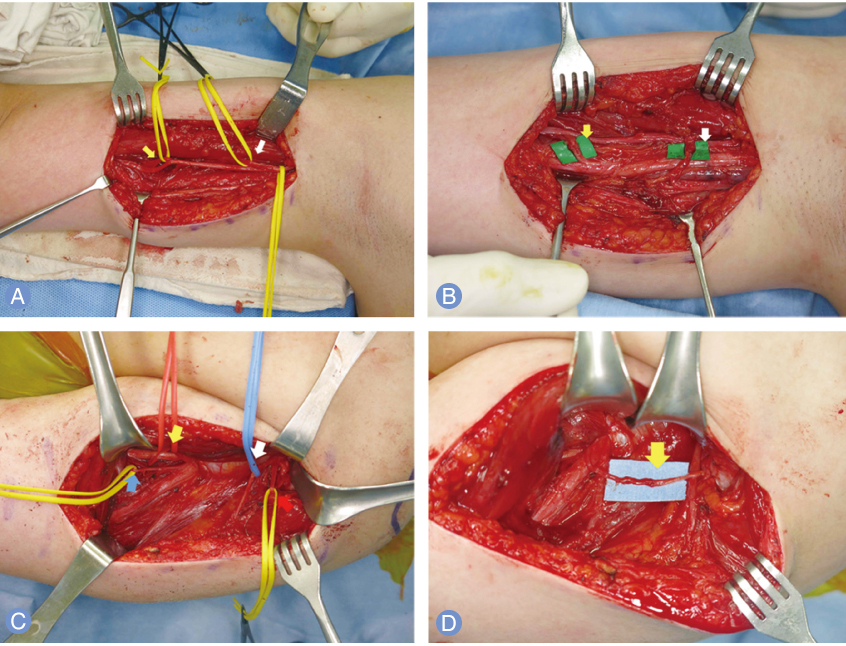
Fig. 3 This patient sustained brachial plexus injury with paralysis of musculocutaneous nerve and axillary nerve. We did ulnar nerve fascicular transfer to the brachialis motor branch and median nerve fascicular transfer to the biceps motor branch on supine position. After that, triceps motor branch was transfered to the axillary nerve. (A) Left loop (yellow arrow), brachialis motor branch of musculocutaneous nerve; right loop (white arrow), biceps motor branch of musculocutaneous nerve. (B) After ulnar nerve fascicular transfer to the brachialis motor branch (yellow arrow) and median nerve fascicular transfer to the biceps motor branch (white arrow). (C) Left side of inferior loop (blue arrow), triceps motor branch of the radial nerve; right side of inferior loop (red arrow), deltoid motor branch of the axillary nerve; left side of superior loop (yellow arrow), ulnar nerve; right side of superior loop (white arrow), sensory branch of axillary nerve. (D) After transfer of the triceps motor branch to the axillary nerve (yellow arrow).
Reference
-
1. Tuttle HK. Exposure of the brachial plexus with nervetransplantation. JAMA. 1913; 61:15–17.
Article2. Bertelli JA, Ghizoni MF. Transfer of the accessory nerve to the suprascapular nerve in brachial plexus reconstruction. J Hand Surg Am. 2007; 32:989–998.
Article3. Suzuki K, Doi K, Hattori Y, Pagsaligan JM. Long-term results of spinal accessory nerve transfer to the suprascapular nerve in upper-type paralysis of brachial plexus injury. J Reconstr Microsurg. 2007; 23:295–299.
Article4. Cardenas-Mejia A, O'Boyle CP, Chen KT, Chuang DC. Evaluation of single-, double-, and triple-nerve transfers for shoulder abduction in 90 patients with supraclavicular brachial plexus injury. Plast Reconstr Surg. 2008; 122:1470–1478.
Article5. Chuang DC, Lee GW, Hashem F, Wei FC. Restoration of shoulder abduction by nerve transfer in avulsed brachial plexus injury: evaluation of 99 patients with various nerve transfers. Plast Reconstr Surg. 1995; 96:122–128.6. Malessy MJ, de Ruiter GC, de Boer KS, Thomeer RT. Evaluation of suprascapular nerve neurotization after nerve graft or transfer in the treatment of brachial plexus traction lesions. J Neurosurg. 2004; 101:377–389.
Article7. Uerpairojkit C, Leechavengvongs S, Witoonchart K, Malungpaishorpe K, Raksakulkiat R. Nerve transfer to serratus anterior muscle using the thoracodorsal nerve for winged scapula in C5 and C6 brachial plexus root avulsions. J Hand Surg Am. 2009; 34:74–78.
Article8. Songcharoen P, Mahaisavariya B, Chotigavanich C. Spinal accessory neurotization for restoration of elbow flexion in avulsion injuries of the brachial plexus. J Hand Surg Am. 1996; 21:387–390.
Article9. Merrell GA, Barrie KA, Katz DL, Wolfe SW. Results of nerve transfer techniques for restoration of shoulder and elbow function in the context of a meta-analysis of the English literature. J Hand Surg Am. 2001; 26:303–314.
Article10. Oberlin C, Beal D, Leechavengvongs S, Salon A, Dauge M, Sarcy J. Nerve transfer to biceps muscle using a part of ulnar nerve for C5–C6 avulsion of the brachial plexus: anatomical study and report of four cases. J Hand Surg Am. 1994; 19:232–237.
Article11. Leechavengvongs S, Witoonchart K, Uerpairojkit C, Thuvasethakul P, Ketmalasiri W. Nerve transfer to biceps muscle using a part of the ulnar nerve in brachial plexus injury (upper arm type): a report of 32 cases. J Hand Surg Am. 1998; 23:711–716.
Article12. Sungpet A, Suphachatwong C, Kawinwonggowit V, Patradul A. Transfer of a single fascicle from the ulnar nerve to the biceps muscle after avulsions of upper roots of the brachial plexus. J Hand Surg Br. 2000; 25:325–328.
Article13. Teboul F, Kakkar R, Ameur N, Beaulieu JY, Oberlin C. Transfer of fascicles from the ulnar nerve to the nerve to the biceps in the treatment of upper brachial plexus palsy. J Bone Joint Surg Am. 2004; 86:1485–1490.
Article14. Sedain G, Sharma MS, Sharma BS, Mahapatra AK. Outcome after delayed Oberlin transfer in brachial plexus injury. Neurosurgery. 2011; 69:822–827.
Article15. Liverneaux PA, Diaz LC, Beaulieu JY, Durand S, Oberlin C. Preliminary results of double nerve transfer to restore elbow flexion in upper type brachial plexus palsies. Plast Reconstr Surg. 2006; 117:915–919.
Article16. Mackinnon SE, Novak CB, Myckatyn TM, Tung TH. Results of reinnervation of the biceps and brachialis muscles with a double fascicular transfer for elbow flexion. J Hand Surg Am. 2005; 30:978–985.
Article17. Carlsen BT, Kircher MF, Spinner RJ, Bishop AT, Shin AY. Comparison of single versus double nerve transfers for elbow flexion after brachial plexus injury. Plast Reconstr Surg. 2011; 127:269–276.
Article18. Ray WZ, Pet MA, Yee A, Mackinnon SE. Double fascicular nerve transfer to the biceps and brachialis muscles after brachial plexus injury: clinical outcomes in a series of 29 cases. J Neurosurg. 2011; 114:1520–1528.
Article19. Leechavengvongs S, Witoonchart K, Uerpairojkit C, Thuvasethakul P. Nerve transfer to deltoid muscle using the nerve to the long head of the triceps, part II: a report of 7 cases. Nerve transfer to biceps muscle using a part of the ulnar nerve in brachial plexus injury (upper arm type): a report of 32 cases. J Hand Surg Am. 2003; 28:633–638.20. Bahm J, Noaman H, Becker M. The dorsal approach to the suprascapular nerve in neuromuscular reanimation for obstetric brachial plexus lesions. Plast Reconstr Surg. 2005; 115:240–244.21. Gu YD. Cervical nerve root transfer from the healthy side in the treatment of brachial plexus root avulsion. Zhonghua Yi Xue Za Zhi. 1989; 69:563–565.22. Chuang DC, Wei FC, Noordhoff MS. Cross-chest C7 nerve grafting followed by free muscle transplantations for the treatment of total avulsed brachial plexus injuries: a preliminary report. Plast Reconstr Surg. 1993; 92:717–725.23. Chuang DC. Neurotization procedures for brachial plexus injuries. Hand Clin. 1995; 11:633–645.
Article24. Gu Y, Xu J, Chen L, Wang H, Hu S. Long term outcome of contralateral C7 transfer: a report of 32 cases. Chin Med J (Engl). 2002; 115:866–868.25. Gu YD. Contralateral C7 root transfer over the last 20 years in China. Chin Med J (Engl). 2007; 120:1123–1126.
Article26. Oberlin C, Durand S, Belheyar Z, Shafi M, David E, Asfazadourian H. Nerve transfers in brachial plexus palsies. Chir Main. 2009; 28:1–9.
Article27. Sammer DM, Kircher MF, Bishop AT, Spinner RJ, Shin AY. Hemi-contralateral C7 transfer in traumatic brachial plexus injuries: outcomes and complications. J Bone Joint Surg Am. 2012; 94:131–137.
Article28. Gu YD, Chen DS, Zhang GM, et al. Long-term functional results of contralateral C7 transfer. J Reconstr Microsurg. 1998; 14:57–59.
Article29. Songcharoen P, Wongtrakul S, Mahaisavariya B, Spinner RJ. Hemi-contralateral C7 transfer to median nerve in the treatment of root avulsion brachial plexus injury. J Hand Surg Am. 2001; 26:1058–1064.
Article30. Yang G, Chang KW, Chung KC. A systematic review of outcomes of contralateral C7 for the treatment of traumatic brachial plexus injury: part 2-donor-site morbidity of contralateral C7 transfer for traumatic brachial plexus injury. Plast Reconstr Surg. 2015; 136:480e–489e.31. Tu YK, Tsai YJ, Chang CH, Su FC, Hsiao CK, Tan JS. Surgical treatment for total root avulsion type brachial plexus injuries by neurotization: a prospective comparison study between total and hemicontralateral C7 nerve root transfer. Microsurgery. 2014; 34:91–101.
Article32. Liu J, Pho RW, Kour AK, Zhang AH, Ong BK. Neurologic deficit and recovery in the donor limb following cross-C7 transfer in brachial-plexus injury. J Reconstr Microsurg. 1997; 13:237–242.
Article33. Chuang DC, Cheng SL, Wei FC, Wu CL, Ho YS. Clinical evaluation of C7 spinal nerve transection: 21 patients with at least 2 years' follow-up. Br J Plast Surg. 1998; 51:285–290.
Article34. Sungpet A, Suphachatwong C, Kawinwonggowit V. Sensory abnormalities after the seventh cervical nerve root transfer. Microsurgery. 1999; 19:287–288.
Article35. Wang SF, Li PC, Xue YH, Yiu HW, Li YC, Wang HH. Contralateral C7 nerve transfer with direct coaptation to restore lower trunk function after traumatic brachial plexus avulsion. J Bone Joint Surg Am. 2013; 95:821–827.
Article36. Kimura J. Intrinsic hand muscles are innervated by C8 and T1, not C6 and C7, roots. Ann Thorac Surg. 2000; 69:665.
Article37. Gao KM, Lao J, Zhao X, Gu YD. Outcome of contralateral C7 nerve transferring to median nerve. Chin Med J (Engl). 2013; 126:3865–3868.38. Wang L, Zhao X, Gao K, Lao J, Gu YD. Reinnervation of thenar muscle after repair of total brachial plexus avulsion injury with contralateral C7 root transfer: report of five cases. Microsurgery. 2011; 31:323–326.
Article39. Waikakul S, Orapin S, Vanadurongwan V. Clinical results of contralateral C7 root neurotization to the median nerve in brachial plexus injuries with total root avulsions. J Hand Surg Br. 1999; 24:556–560.
Article40. Gorio A, Carmignoto G, Millesi H, Mingrino S. Reformation, maturation and stabilization of neuromuscular junctions in peripheral nerve regeneration. In : Gorio A, editor. Posttraumatic peripheral nerve regeneration. New York: Raven Press;1981. p. 481–492.41. Lin H, Lv D, Hou C, Chen D. Modified C-7 neurotization in the treatment of brachial plexus avulsion injury. J Neurosurg. 2011; 115:865–869.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Tendon Transfer for Radial Nerve Paralysis and Multiple Extensors Rupture
- Upper Limb Reconstruction in Tetraplegic Patients: A Primer for Spinal Cord Injury Specialists
- Nerve Repair and Nerve Grafting in Brachial Plexus Injuries
- Nerve Transfers to the Musculocutaneous and Suprascapular Nerve for Restoration of Elbow and Shoulder Function in Brachial Plexus Avulsion: An Early Experience
- Clinical Observation of Peripheral Nerve Injury of the Upper Extremity
