Clinical characteristics and treatment outcomes of isolated myeloid sarcoma without bone marrow involvement: a single-institution experience
- Affiliations
-
- 1Department of Internal Medicine, Yonsei University Wonju College of Medicine, Wonju, Korea.
- 2Department of Internal Medicine, Yonsei University College of Medicine, Seoul, Korea. jwcheong70@yuhs.ac
- 3Graduate School of Medical Science and Engineering, Korea Advanced Institute of Science and Technology, Daejeon, Korea.
- KMID: 2390980
- DOI: http://doi.org/10.5045/br.2017.52.3.184
Abstract
- BACKGROUND
Isolated myeloid sarcoma (MS) is a rare extramedullary tumor mass composed of malignant myeloid precursor cells without any evidence of leukemia in the peripheral blood and bone marrow. We describe the clinical characteristics and outcomes of patients diagnosed with isolated MS at our institution.
METHODS
We retrospectively reviewed 9 of 497 acute myeloid leukemia (AML) patients (1.8%) with isolated MS. Isolated MS patients were divided into 2 groups according to the first-line treatment strategy: systemic treatment only (S) or local treatment with or without systemic treatment (LS).
RESULTS
The most common site of MS occurrence was the head and neck area (N=4, 44.4%), followed by the anterior mediastinum (N=2, 22.2%) and the gastrointestinal tract (N=2, 22.2%). The tumors of 4 patients (44.4%) eventually evolved to AML, in a median time of 13.4 months (range, 2.4-20.1 mo). The number of patients achieving complete remission after first-line treatment was higher in the LS group (N=5, 83.3%) than in the S group (N=1, 33.3%) (P =0.226). All patients in the LS group survived, but those in the S group died (P=0.012).
CONCLUSION
Accurate and rapid diagnosis using various modalities and the early initiation of intensive combined treatment may be the optimal strategies to reduce the risk of isolated MS subsequently evolving to AML. To fully understand the characteristics of isolated MS, a larger number of patients from a multinational study is necessary.
Keyword
MeSH Terms
Figure
-
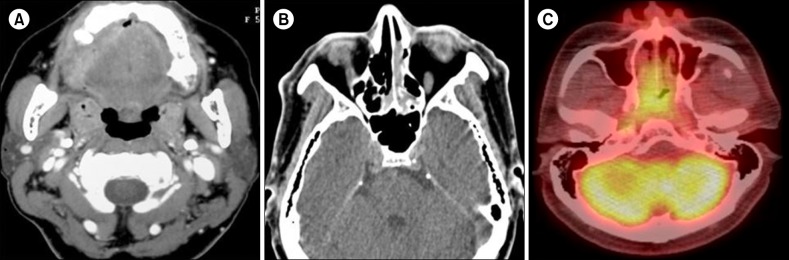
Fig. 1 Computed tomography (CT) findings of 56-year-old woman with primary gingival involvement (A) and 48-year-old man with nasal cavity and naso-oropharynx involvement by myeloid sarcoma (B, C). (A) Contrast-enhanced axial CT scan of the neck shows lytic destruction of the right side alveolar bone. (B) Contrast-enhanced axial CT scan of the neck shows diffuse thickening of the nasal cavity. (C) 18Fluorine-labeled glucose axial PET scan shows strong focal uptake by the same lesions seen on the CT scan.
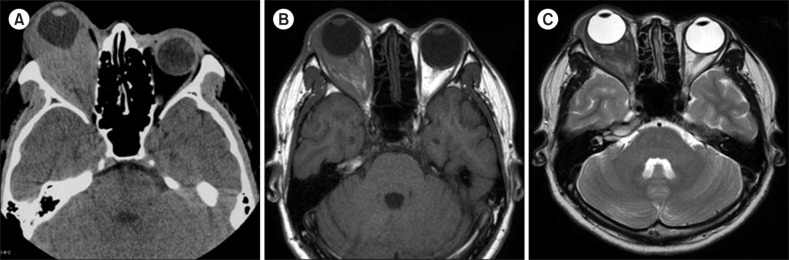
Fig. 2 Computed tomography (CT) and magnetic resonance imaging (MRI) findings of a 24-year-old man with involvement of the right orbit by myeloid sarcoma who reported right eye proptosis. (A) Contrast-enhanced axial CT scan of the orbit shows a homogeneously enhancing soft tissue mass in the intra-conal and extra-conal spaces of the right orbit. (B) T1-weighted axial MRI scan of the orbit shows a right orbit mass iso-intense to the periorbital muscle. (C) T2-weighted axial MRI scan of the orbit shows a right orbit mass mildly hyper-intense to the periorbital muscle.
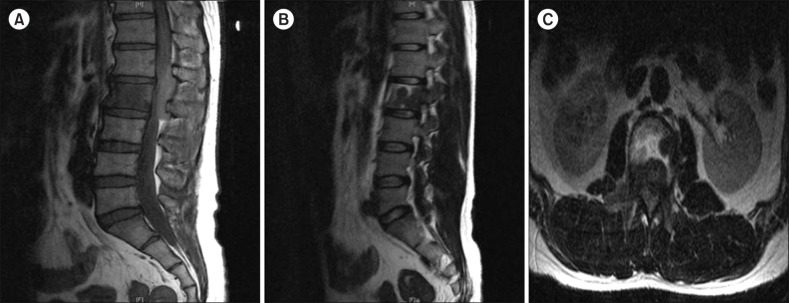
Fig. 3 Magnetic resonance imaging (MRI) findings of a 34-year-old man with involvement of the second lumbar vertebral body by myeloid sarcoma who reported back pain and bilateral leg weakness. (A) Sagittal T1-weighted MRI scan of the spine shows an epidural and paravertebral mass iso-intense to muscle at the second lumbar vertebra level. (B) Sagittal T2-weighted MRI scan of the spine shows an epidural and paravertebral mass iso-intense or mildly hyper-intense to muscle at the second lumbar vertebra level. (C) Axial T2-weighted MRI scan of the spine shows a heterogeneously enhancing epidural mass with enhancement similar to or greater than that of normal muscle.
Cited by 1 articles
-
A Case of Myeloid Sarcoma in the Nasal Cavity Occurred in the Patient with Leukemic Transformation in Myelodysplastic Syndrome
Dong Hoo Lee, Sung Yool Park, Ha Young Park, Seong Kook Park
Korean J Otorhinolaryngol-Head Neck Surg. 2020;63(2):81-84. doi: 10.3342/kjorl-hns.2019.00017.
Reference
-
1. Campidelli C, Agostinelli C, Stitson R, Pileri SA. Myeloid sarcoma: extramedullary manifestation of myeloid disorders. Am J Clin Pathol. 2009; 132:426–437. PMID: 19687319.2. Kitagawa Y, Sameshima Y, Shiozaki H, et al. Isolated granulocytic sarcoma of the small intestine successfully treated with chemotherapy and bone marrow transplantation. Int J Hematol. 2008; 87:410–413. PMID: 18365139.
Article3. Pileri SA, Ascani S, Cox MC, et al. Myeloid sarcoma: clinicopathologic, phenotypic and cytogenetic analysis of 92 adult patients. Leukemia. 2007; 21:340–350. PMID: 17170724.
Article4. Kaygusuz G, Kankaya D, Ekinci C, Topçuoğlu P, Kuzu I. Myeloid sarcomas: a clinicopathologic study of 20 cases. Turk J Haematol. 2015; 32:35–42. PMID: 25805673.
Article5. Yilmaz AF, Saydam G, Sahin F, Baran Y. Granulocytic sarcoma: a systematic review. Am J Blood Res. 2013; 3:265–270. PMID: 24396704.6. Mirza MK, Sukhanova M, Stölzel F, et al. Genomic aberrations in myeloid sarcoma without blood or bone marrow involvement: characterization of formalin-fixed paraffin-embedded samples by chromosomal microarrays. Leuk Res. 2014; 38:1091–1096. PMID: 25088808.
Article7. Tsimberidou AM, Kantarjian HM, Estey E, et al. Outcome in patients with nonleukemic granulocytic sarcoma treated with chemotherapy with or without radiotherapy. Leukemia. 2003; 17:1100–1103. PMID: 12764375.
Article8. Breccia M, Mandelli F, Petti MC, et al. Clinico-pathological characteristics of myeloid sarcoma at diagnosis and during follow-up: report of 12 cases from a single institution. Leuk Res. 2004; 28:1165–1169. PMID: 15380340.
Article9. Dores GM, Devesa SS, Curtis RE, Linet MS, Morton LM. Acute leukemia incidence and patient survival among children and adults in the United States, 2001-2007. Blood. 2012; 119:34–43. PMID: 22086414.
Article10. Swerdlow SH, Campo E, Harris NL, editors. WHO classification of tumours of haematopoietic and lymphoid tissues. 4th ed. Lyon, France: IARC Press;2008.11. Neiman RS, Barcos M, Berard C, et al. Granulocytic sarcoma: a clinicopathologic study of 61 biopsied cases. Cancer. 1981; 48:1426–1437. PMID: 7023656.
Article12. van Veen S, Kluin PM, de Keizer RJ, Kluin-Nelemans HC. Granulocytic sarcoma (chloroma). Presentation of an unusual case. Am J Clin Pathol. 1991; 95:567–571. PMID: 2014784.
Article13. Alexiev BA, Wang W, Ning Y, et al. Myeloid sarcomas: a histologic, immunohistochemical, and cytogenetic study. Diagn Pathol. 2007; 2:42. PMID: 17974004.
Article14. Shinagare AB, Krajewski KM, Hornick JL, et al. MRI for evaluation of myeloid sarcoma in adults: a single-institution 10-year experience. AJR Am J Roentgenol. 2012; 199:1193–1198. PMID: 23169708.
Article15. Noh BW, Park SW, Chun JE, Kim JH, Kim HJ, Lim MK. Granulocytic sarcoma in the head and neck: CT and MR imaging findings. Clin Exp Otorhinolaryngol. 2009; 2:66–71. PMID: 19565030.
Article16. Seok JH, Park J, Kim SK, Choi JE, Kim CC. Granulocytic sarcoma of the spine: MRI and clinical review. AJR Am J Roentgenol. 2010; 194:485–489. PMID: 20093613.
Article17. Ooi GC, Chim CS, Khong PL, et al. Radiologic manifestations of granulocytic sarcoma in adult leukemia. AJR Am J Roentgenol. 2001; 176:1427–1431. PMID: 11373207.
Article18. Eshghabadi M, Shojania AM, Carr I. Isolated granulocytic sarcoma: report of a case and review of the literature. J Clin Oncol. 1986; 4:912–917. PMID: 2423654.
Article19. Movassaghian M, Brunner AM, Blonquist TM, et al. Presentation and outcomes among patients with isolated myeloid sarcoma: a Surveillance, Epidemiology, and End Results database analysis. Leuk Lymphoma. 2015; 56:1698–1703. PMID: 25213180.
Article20. Yamauchi K, Yasuda M. Comparison in treatments of nonleukemic granulocytic sarcoma: report of two cases and a review of 72 cases in the literature. Cancer. 2002; 94:1739–1746. PMID: 11920536.21. Byrd JC, Edenfield WJ, Shields DJ, Dawson NA. Extramedullary myeloid cell tumors in acute nonlymphocytic leukemia: a clinical review. J Clin Oncol. 1995; 13:1800–1816. PMID: 7602369.
Article22. Meis JM, Butler JJ, Osborne BM, Manning JT. Granulocytic sarcoma in nonleukemic patients. Cancer. 1986; 58:2697–2709. PMID: 3465429.
Article23. Antic D, Elezovic I, Milic N, et al. Is there a "gold" standard treatment for patients with isolated myeloid sarcoma? Biomed Pharmacother. 2013; 67:72–77. PMID: 23218987.
Article24. Bakst R, Wolden S, Yahalom J. Radiation therapy for chloroma (granulocytic sarcoma). Int J Radiat Oncol Biol Phys. 2012; 82:1816–1822. PMID: 21962486.
Article25. Wong WS, Loong F, Ooi GC, Tse TC, Chim CS. Primary granulocytic sarcoma of the mediastinum. Leuk Lymphoma. 2004; 45:1931–1933. PMID: 15223657.
Article26. Vassiliou V, Christopoulos C, Kardamakis D, et al. Isolated granulocytic sarcoma involving the mediastinum and bilateral cervical lymph nodes. Eur J Haematol. 2007; 78:548. PMID: 17509108.
Article27. Chevallier P, Labopin M, Cornelissen J, et al. Allogeneic hematopoietic stem cell transplantation for isolated and leukemic myeloid sarcoma in adults: a report from the Acute Leukemia Working Party of the European group for Blood and Marrow Transplantation. Haematologica. 2011; 96:1391–1394. PMID: 21685467.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Intraparenchymal Myeloid Sarcoma and Subsequent Spinal Myeloid Sarcoma for Acute Myeloblastic Leukemia
- A rare case of isolated myeloid sarcoma of the small gut with inv(16)(p13;q22) without bone marrow involvement
- Granulocytic Sarcoma in Breast after Bone Marrow Transplantation
- Isolated Myeloid Sarcoma Presenting as Cord Compression by Paraspinal Mass
- Temporal Bone Myeloid Sarcoma
