Ulnar Collateral Ligament Tear Combined with Medial Epicondylitis of the Elbow
- Affiliations
-
- 1Department of Orthopaedic Surgery, Good Samsun Hospital, Busan, Korea. hljo88@hanmail.net
- KMID: 2389653
- DOI: http://doi.org/10.5763/kjsm.2017.35.2.125
Abstract
- Medial epicondylitis, also known as "golfer's elbow," is a common overuse syndrome of the elbow and predominantly affects the origin of the common flexor tendon. We report two unique cases of medial epicondylitis complicated by chronic complete tear of the ulnar collateral ligament and common flexor tendon origin. Physical examination showed a focal huge swelling of medial epicondylar region of the dominant elbow and magnetic resonance imaging revealed complete tear of the ulnar collateral ligament and common flexor tendon and extravasation of intra-articular effusion. Satisfactory results were achieved with ulnar collateral ligament reconstruction and simultaneous repair of the common flexor tendon origin.
MeSH Terms
Figure
-

Fig. 1 Patient 1. (A) Photograph of right elbow shows focal swelling (white arrow) in medial epicondylar region. (B) Anteroposterior plain radiograph shows sclerosis of medial epicondylar margin. Bilateral gravity valgus stress long axis sonographic images in (C) injured and (D) uninjured elbow show focal hypoechoic focus (asterisk) corresponding to the tears of pronator-flexor muscles and ulnar collateral ligament, and increased ulnohumeral distance (d) in injured elbow. U: ulna, H: humerus.
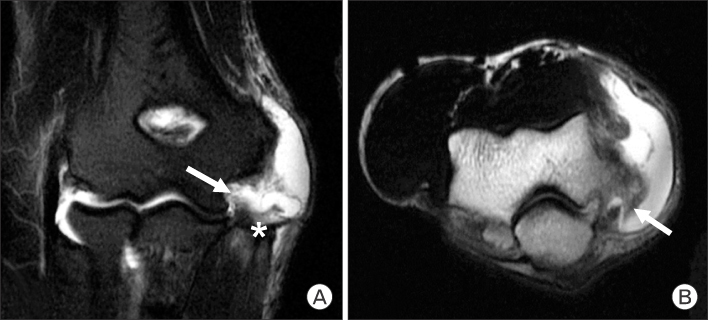
Fig. 2 Magnetic resonance imaging of right elbow in patient 1. (A) Coronal T2-weighted fast spin echo image of the elbow shows complete tear of flexor-pronator tendon (asterisk) and humeral origin of ulnar collateral ligament (white arrow). Also note marked extravasation of high signal intensity joint effusion. (B) Axial T2-weighted fast spin-echo image of the elbow shows abnormal high signal intensity joint effusion and tear of posterior band of ulnar collateral ligament and joint capsule (white arrow).
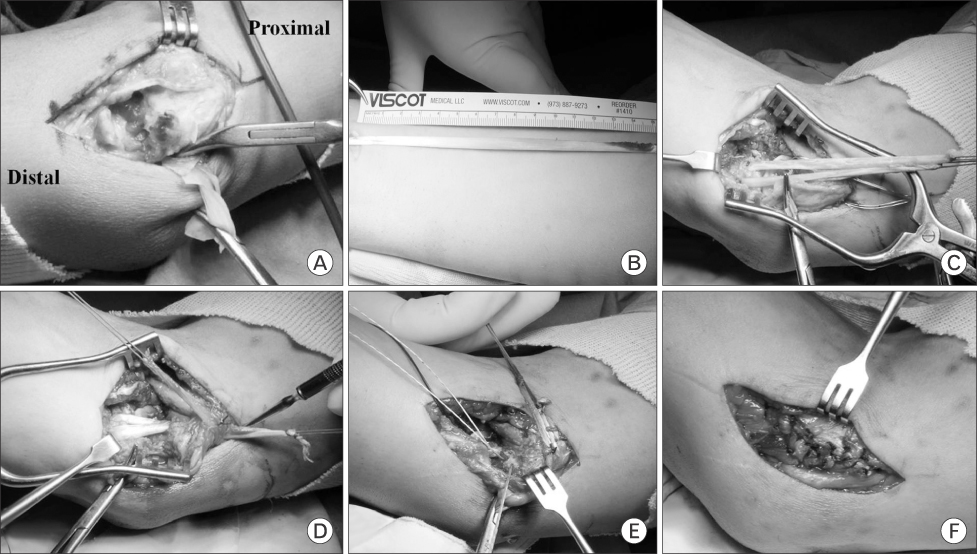
Fig. 3 Operative photographs of patient 1. (A) Complete tear of flexor muscle and marked proliferation of pinkish granulation tissue. (B) Harvesting of ipsilateral palmaris longus tendon. (C) Tendon graft passage through ulnar tunnel. (D) Tensioning of graft in humeral tunnel with docking technique. (E) Suture anchor repair of pronator and common flexor tendon. (F) Final construct of repair.
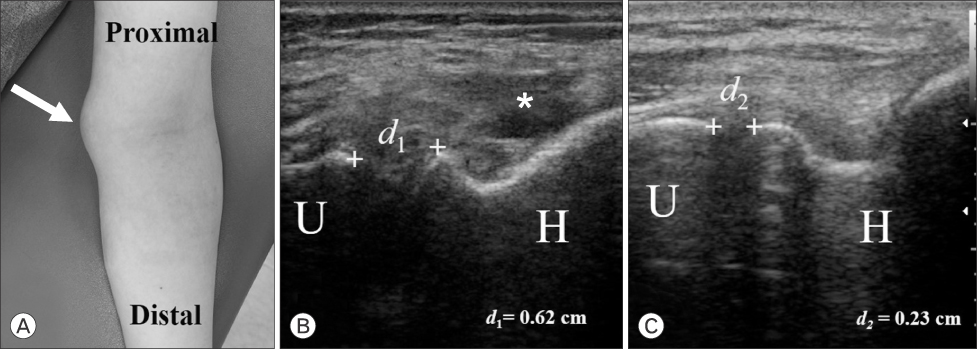
Fig. 4 Patient 2. (A) Photograph of left elbow shows focal swelling (white arrow) in medial epicondylar region. (B) Anteroposterior plain radiograph shows no significant abnormal findings. Bilateral gravity valgus stress long axis sonographic images in (B) injured and (C) uninjured elbow show focal hypoechoic focus (asterisk) corresponding to the tears of pronator-flexor muscles and ulnar collateral ligament, and increased ulnohumeral distance (d) in injured elbow. U: ulna, H: humerus.
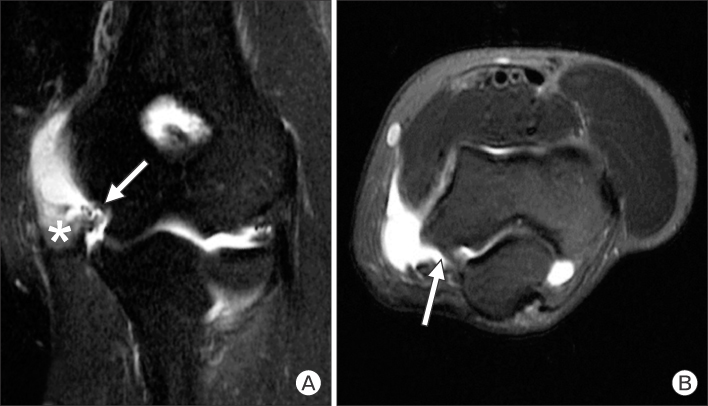
Fig. 5 Magnetic resonance imaging of left elbow in patient 2. (A) Coronal T2-weighted image of the elbow shows complete tear of flexor-pronator tendon (asterisk) and humeral origin of ulnar collateral ligament (white arrow). (B) Axial T2-weighted image shows maintained posterior band of ulnar collateral ligament and joint capsule (white arrow).
Reference
-
1. Ciccotti MC, Schwartz MA, Ciccotti MG. Diagnosis and treatment of medial epicondylitis of the elbow. Clin Sports Med. 2004; 23:693–705.2. Shiri R, Viikari-Juntura E, Varonen H, Heliovaara M. Prevalence and determinants of lateral and medial epicondylitis: a population study. Am J Epidemiol. 2006; 164:1065–1074.3. Kurvers H, Verhaar J. The results of operative treatment of medial epicondylitis. J Bone Joint Surg Am. 1995; 77:1374–1379.4. Vinod AV, Ross G. An effective approach to diagnosis and surgical repair of refractory medial epicondylitis. J Shoulder Elbow Surg. 2015; 24:1172–1177.5. Otoshi K, Kikuchi S, Shishido H, Konno S. The proximal origins of the flexor-pronator muscles and their role in the dynamic stabilization of the elbow joint: an anatomical study. Surg Radiol Anat. 2014; 36:289–294.6. Ciccotti MG, Ramani MN. Medial epicondylitis. Tech Hand Up Extrem Surg. 2003; 7:190–196.7. Hwang TH, Cho HL, Kim HM, Park KB, Jo H. Gravity valgus stress ultrasonographic assessment of ulnar collateral ligament injury among baseball players. Korean J Sports Med. 2015; 33:75–82.8. Kijowski R, De Smet AA. Magnetic resonance imaging findings in patients with medial epicondylitis. Skeletal Radiol. 2005; 34:196–202.9. Smidt N, van der Windt DA, Assendelft WJ, Deville WL, Korthals-de Bos IB, Bouter LM. Corticosteroid injections, physiotherapy, or a wait-and-see policy for lateral epicondylitis: a randomised controlled trial. Lancet. 2002; 359:657–662.10. Jobe FW, Stark H, Lombardo SJ. Reconstruction of the ulnar collateral ligament in athletes. J Bone Joint Surg Am. 1986; 68:1158–1163.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Comparison of Ulnar Collateral Ligament Reconstruction Techniques in the Elbow of Sports Players
- Ultrasonographic differential diagnosis of medial elbow pain
- Management of Ulnar Collateral Ligament Injuries in Overhead Athletes
- Medial Instability of the Elbow
- The Ulnar Collateral Ligament is Always Torn in the Posterolateral Elbow Dislocation: A Suggestion on the new Mechanism of Dislocation Using MRI Findings
