Successful laparoscopic management of uterine serosal pregnancy
- Affiliations
-
- 1Department of Obstetrics and Gynecology, CHA Bundang Medical Center, CHA University, Seongnam, Korea.
- 2Comprehensive Gynecologic Cancer Center, Department of Obstetrics and Gynecology, CHA Bundang Medical Center, CHA University, Seongnam, Korea. oursk79@cha.ac.kr
- 3Department of Pathology, CHA Bundang Medical Center, CHA University, Seongnam, Korea.
- KMID: 2386284
- DOI: http://doi.org/10.5468/ogs.2017.60.4.391
Abstract
- Uterine serosal pregnancy is an extremely rare form of ectopic pregnancy. This is a report of a 35-year-old primigravida woman who was diagnosed with uterine serosal pregnancy via laparoscopic intervention. A 35-year-old woman (gravida 1, para 0) was referred from a local clinic for a ruptured left tubal pregnancy at amenorrhea 5+0 weeks with elevated serum beta human chorionic gonadotropin (16,618 mIU/mL). A pregnancy on the left posterior wall of the uterine serosa was diagnosed during the operation and successfully treated with laparoscopic surgery as a conservative management strategy to enable fertility preservation. With the advantages of ultrasonography and laparoscopy, an early diagnosis of a primary abdominal pregnancy located on the left posterior wall of the uterine serosa was made, prior to the occurrence of severe intra-abdominal massive hemorrhage, which was then treated laparoscopically as a conservative management strategy enabling the preservation of fertility.
MeSH Terms
Figure
-
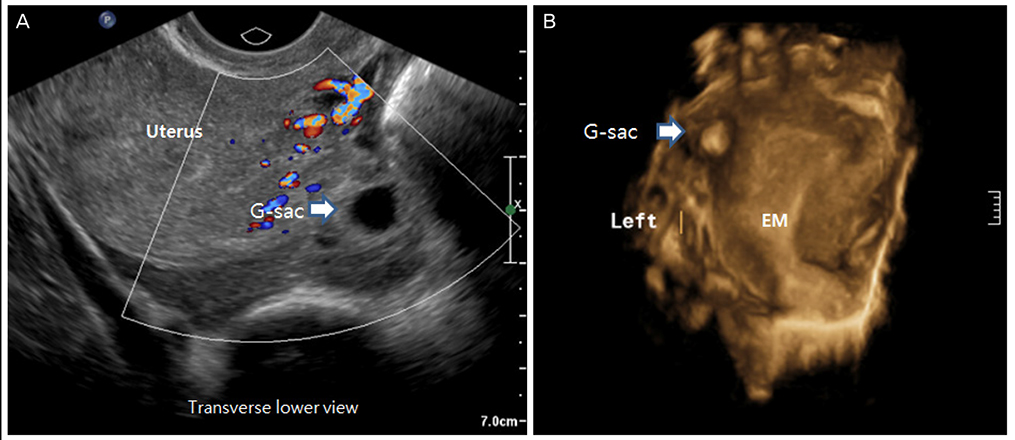
Fig. 1 (A) Preoperative two-dimensional transvaginal sonogram revealed a gestational sac (G-sac) that was separated from the uterus, with a certain amount of hemoperitoneum, suggesting the presence of an ectopic pregnancy. (B) Three-dimensional transvaginal sonogram revealed a 1.8-cm mass located adjacent to the left cornus, clearly outside the endometrium (EM).
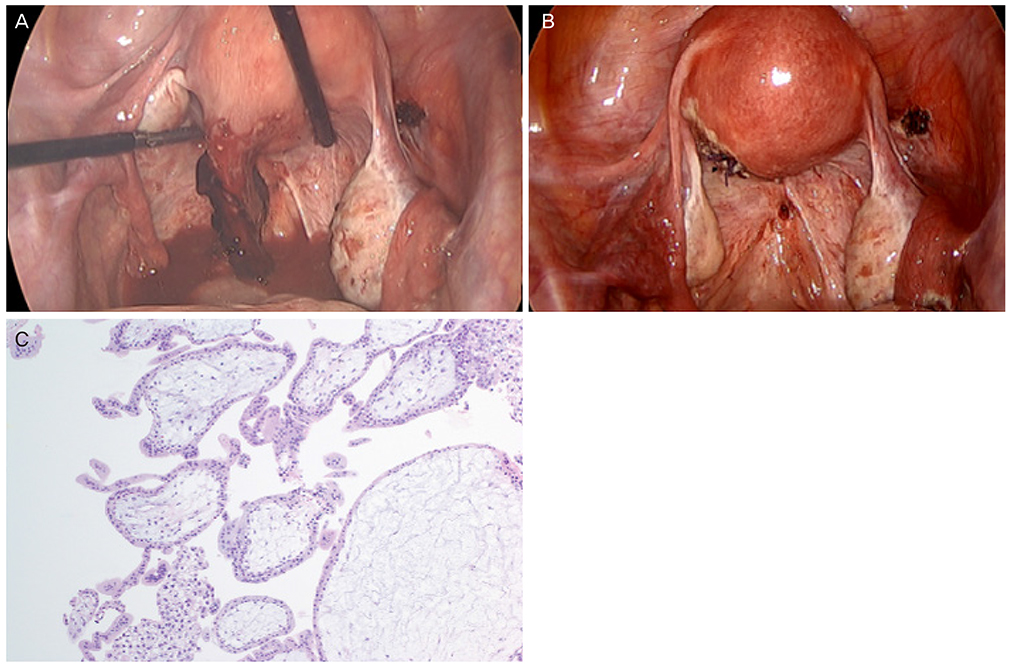
Fig. 2 Laparoscopic and pathologic findings. (A) An approximately 2.0-cm ruptured ectopic mass at the left posterior serosa of the uterus was observed. Both adnexae were grossly normal. (B) After removing the ectopic mass, chromopertubation was successfully performed on both tubes, and the scar was meticulous sutured. (C) Microscopic photograph of trophoblastic villi removed from the uterine serosa (H&E, ×200).
Reference
-
1. Ekele BA, Ahmed Y, Nnadi D, Ishaku K. Abdominal pregnancy: ultrasound diagnosis aided by the balloon of a Foley catheter. Acta Obstet Gynecol Scand. 2005; 84:701–702.2. Atrash HK, Friede A, Hogue CJ. Abdominal pregnancy in the United States: frequency and maternal mortality. Obstet Gynecol. 1987; 69(3 Pt 1):333–337.3. Poole A, Haas D, Magann EF. Early abdominal ectopic pregnancies: a systematic review of the literature. Gynecol Obstet Invest. 2012; 74:249–260.4. Park WI, Jeon YM, Lee JY, Shin SY. Subserosal pregnancy in a previous myomectomy site: a variant of intramural pregnancy. J Minim Invasive Gynecol. 2006; 13:242–244.5. Kang MJ, Joo JK, Kang JH, Joo IS, Park Y, Seo KY. Primary uterine serosal pregnancy with myometrial invasion. Korean J Obstet Gynecol. 2012; 55:213–217.6. Choi YY, Kim JS, Koh MW. A case of uterine serosal pregnancy with both ovarian cysts. Korean J Obstet Gynecol. 2005; 48:778–783.7. Nkusu Nunyalulendho D, Einterz EM. Advanced abdominal pregnancy: case report and review of 163 cases reported since 1946. Rural Remote Health. 2008; 8:1087.8. Alto WA. Abdominal pregnancy. Am Fam Physician. 1990; 41:209–214.9. Kumar P, Malhotra N. Ectopic pregnancy. In : Kumar P, Malhotra N, editors. Jeffcoate's principles of gynaecology. New Delhi: JP Brothers Medical Publishing;2008. Vol. 7:p. 157–159.10. Hallatt JG, Grove JA. Abdominal pregnancy: a study of twenty-one consecutive cases. Am J Obstet Gynecol. 1985; 152:444–449.11. Lee GS, Hur SY, Kown I, Shin JC, Kim SP, Kim SJ. Diagnosis of early intramural ectopic pregnancy. J Clin Ultrasound. 2005; 33:190–192.12. Liang C, Li X, Zhao B, Du Y, Xu S. Demonstration of the route of embryo migration in retroperitoneal ectopic pregnancy using contrast-enhanced computed tomography. J Obstet Gynaecol Res. 2014; 40:849–852.13. Persson J, Reynisson P, Masback A, Epstein E, Saldeen P. Histopathology indicates lymphatic spread of a pelvic retroperitoneal ectopic pregnancy removed by robot-assisted laparoscopy with temporary occlusion of the blood supply. Acta Obstet Gynecol Scand. 2010; 89:835–839.14. Lawrence A, Jurkovic D. Three-dimensional ultrasound diagnosis of interstitial pregnancy. Ultrasound Obstet Gynecol. 1999; 14:292–293.15. Harika G, Gabriel R, Carre-Pigeon F, Alemany L, Quereux C, Wahl P. Primary application of three-dimensional ultrasonography to early diagnosis of ectopic pregnancy. Eur J Obstet Gynecol Reprod Biol. 1995; 60:117–120.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Intrauterine Pregnancy after Laparoscopic Bilateral Uterine Artery Ligation for Treatment Uterine Myoma
- Primary uterine serosal pregnancy with myometrial invasion
- Successful laparoscopic treatment of an omental pregnancy
- Repetitive Spontaneous Uterine Rupture in the First Trimester after Laparoscopic Myomectomy: A Case Report and Review of Literature
- Laparoscopic Cholecystectomy in the Second Trimester of Pregnancy
